
Abstract
Background
Traumatic brain injury (TBI) is a significant global health concern resulting in persistent physical, cognitive, and social impairments that affect daily functioning and quality of life. Resting-state functional magnetic resonance imaging (rs-fMRI) has emerged as a valuable neuroimaging modality offering novel insights into brain function at rest.
Summary
This integrative review synthesised evidence from studies indexed in PubMed, ScienceDirect, and Scopus on resting-state network (RSN) alterations and their association with cognitive dysfunction in TBI. Consistent alterations in functional connectivity were identified across multiple RSNs in TBI population, particularly within the default mode network (DMN), frontoparietal network (FPN), and salience network. DMN connectivity showed strong associations with attention, processing speed, and memory. FPN connectivity changes corresponded with executive function deficits, while sensorimotor network disruptions were linked to attentional impairments. Dynamic longitudinal changes in network connectivity further suggested underlying neuroplasticity mechanisms.
Key Message
Resting-state functional connectivity demonstrates as a potential sensitive biomarker for TBI diagnosis, prognosis, and rehabilitation monitoring. With implications for individualised rehabilitation, these findings highlight the need for a network oriented approach for understanding, diagnosing, and treating TBI. Future research should explore longitudinal changes in RSN connectivity and their implications for neuro-rehabilitation strategies.
Introduction
Traumatic brain injury (TBI) is a condition that is usually caused by road traffic accidents (RTA), falls or sports-related injury that results in a change in the brain’s functioning. 1 TBI is defined as an alteration in brain function, or other evidence of brain pathology, caused by an external mechanical force like a blow, jolt or penetrating injury to the head. It is classified by severity into mild (GCS 13–15), moderate (GCS 9–12) and severe (GCS ≤ 8) based on the Glasgow Coma Scale, loss of consciousness duration and post-traumatic amnesia. 2 Depending on the severity of injury, mild to severe TBI patients experience cognitive impairments, headaches, visual difficulties, sleep disturbances and post-traumatic epilepsy. 3
As a result of TBI, the neurons and neural pathways get damaged, which leads to disruptions in cognitive processing. Acute axonal injury and contusions impact brain regions associated with cognition, particularly the frontal and temporal lobes. 4 The impairments resulting from the injury frequently manifest as difficulties in attention, memory recall, reasoning and executive functioning. 5 Research has identified structural damage associated with the cognitive deficits (working memory and reasoning), which highlights the importance of intact white matter connections. 5
The wide use of functional magnetic resonance imaging (fMRI) helps us understand the neural mechanisms behind the alteration in brain connections due to TBI. These methods are used to correlate the results with neuropsychological outcomes like attention and memory deficits in chronic TBI patients. 6 According to the neuroimaging results, TBI might accelerate the neurodegenerative process over time, resulting in cognitive decline and functional deficits.7, 8 This explains the importance of identifying neuroimaging biomarkers that can predict cognitive outcomes and help in framing individualised rehabilitation techniques. 9
fMRI and diffusion tensor imaging (DTI) are used for analysing the functional and structural connections, to measure the brain’s activity and understand the underlying neurobiological mechanism. These methods provide insights by visualising the anatomical and functional changes in the brain due to TBI. 10 For instance, DTI-based research has shown changes in the white matter integrity that are associated with cognitive dysfunction following TBI, which proves a significant connection for cognitive function.11, 12 Likewise, the neuroimaging studies have shown subtle changes in functional networks, impacting cognitive functions even when there is no visible structural damage to the brain. This may be due to compensatory mechanisms supporting one another. 13
For individuals with TBI, identifying the neuroimaging biomarkers associated with cognitive impairments might be insightful in order to predict outcomes and guide rehabilitation programmes. 14 As the field of neuroimaging develops further, implementing these findings in clinical practice would be very crucial, as it can help the treating physician and the therapist to address the challenges faced by them and for precise diagnosis.
Furthermore, improvements in neuroimaging and analytic techniques have led to the discovery of resting state networks (RSNs), where the fMRI data is broken down into discrete functional units identified as networks. This method is called independent component analysis (ICA). 15 This has made it easier to comprehend how various brain regions interact while at rest and has created possibilities to investigate how these networks change in conditions like TBI. 16
Studies in this field have identified the RSNs, namely the default mode network (DMN), dorsal attention network (DAN), ventral attention network (VAN), salience network (SN), sensorimotor network (SMN), visual network (VN) and executive control network (ECN). Each one of these networks has a distinct contribution to cognitive processing. Research on RSNs in the field of TBI is limited when compared to its findings in psychiatric illnesses.17, 18
There are significant gaps in our knowledge of how exactly the RSNs and cognitive functions are correlated in TBI. Detailed research is required to provide comprehensive results and achieve a holistic understanding of the mechanism, though existing literature has focused only on specific cognitive functions. The integrative review aims to fill in the literature gap by compiling the existing studies in this field to give a better understanding on the relationship between functional connectivity and cognitive abilities like memory, attention, executive functioning and visuospatial skills, with the help of advanced neuroimaging techniques in TBI.
Methods
An integrative review of the literature was conducted using databases including PubMed, ScienceDirect and Scopus to identify studies examining resting-state functional MRI and cognitive outcomes in TBI. Relevant peer-reviewed articles focusing on RSN alterations and their associations with cognitive domains were examined. The literature was synthesised to identify recurring patterns, network-specific findings and conceptual links between functional connectivity and cognitive dysfunction in TBI. The information consolidation was carried out through a step-by-step process of data extraction, classification, integration and data analysis. The studies were categorised based on the cognitive functions and brain networks they examined. For each category, an overview of the research settings, study populations and experimental designs employed was noted. Additionally, the assessment utilised and the general conclusions drawn from these investigations were included. The time elapsed from injury to neuroimaging assessment was extracted where reported, as acute, sub-acute and chronic phases of TBI are associated with distinct changes in resting-state connectivity due to changing neurobiological processes such as oedema, diaschisis and neuroplasticity.10, 16 As this is an integrative review rather than a meta-analysis, formal pooling of effect sizes and confidence intervals was not performed. 19 The strength of evidence is reflected narratively based on the consistency, replication and directionality of results across studies, and findings should be interpreted as exploratory rather than definitive quantitative findings. A formal risk of bias assessment using a standardised tool was not conducted, as integrative reviews do not mandate formal bias appraisal. 20 However, potential sources of bias were considered qualitatively, including small sample sizes, cross-sectional study designs, heterogeneity of TBI severity and variability in neuroimaging acquisition parameters.
Results
Integrative Synthesis of Resting State Networks and Cognitive Functions
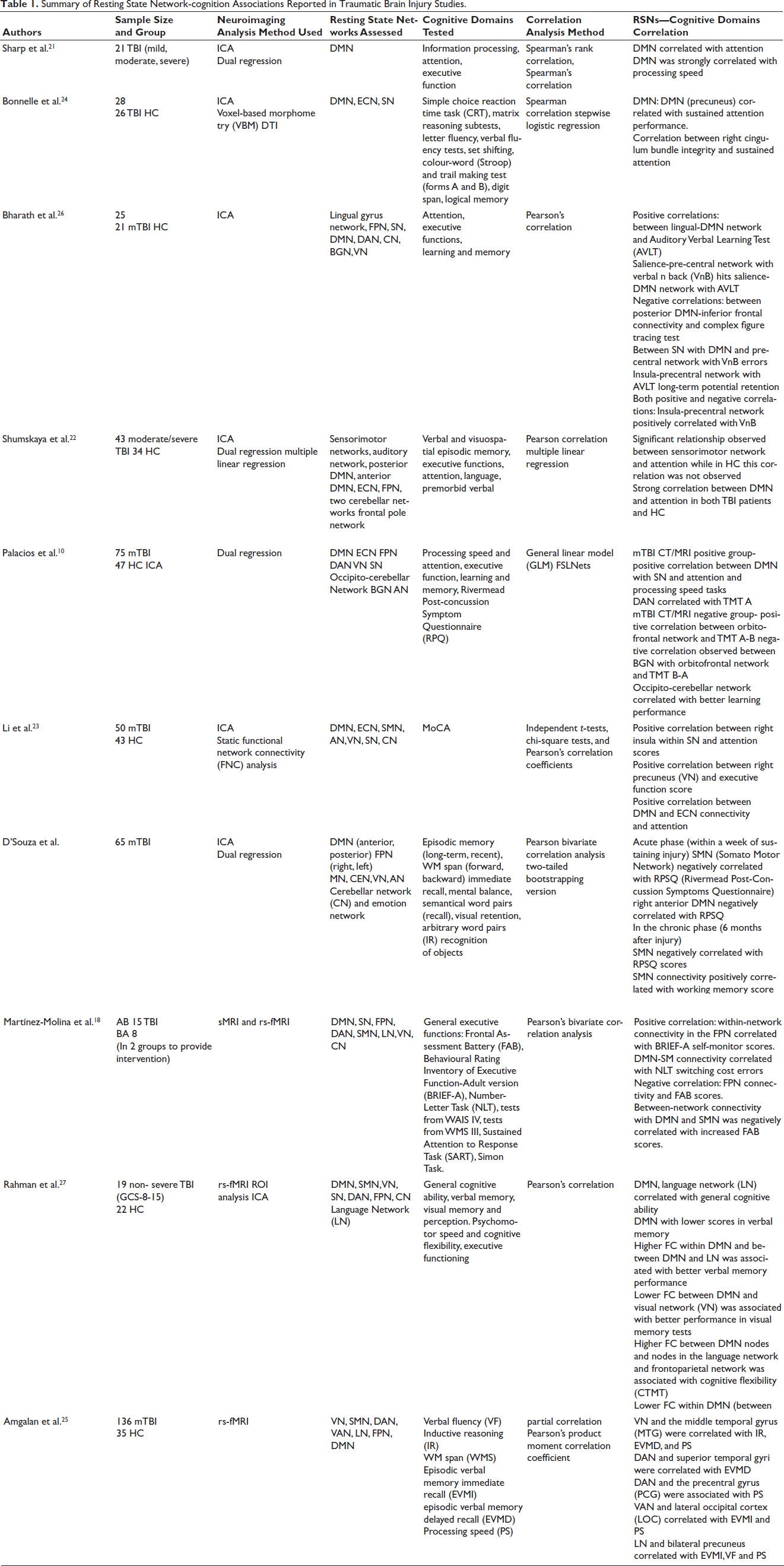
Table 1 summarises the findings on indicating the RSNs associated with each cognitive domain.
Summary of Resting State Network-cognition Associations Reported in Traumatic Brain Injury Studies.
Resting State Networks Associated with Attention
Default Mode Network
Existing literature suggests that alterations in DMN connectivity are associated with attention-related measures in TBI.10, 21–24 Several studies have demonstrated an inverse relationship between DMN connectivity and processing speed, specifically in the posterior cingulate cortex, indicating higher DMN connectivity is associated with better performance. 21 There was an association between precuneus (DMN), and sustained attention. 24 A trend was noted towards a significant effect of DMN connectivity on attention, with abnormally high connectivity correlating with more efficient response speed in TBI patients. 24 DMN and trail-making test scores were linked in mTBI patients with positive computed tomography/magnetic resonance imaging (CT/MRI) scans. 10 A link was noted between DMN and ECN connection and attention scores, which suggests a strong relationship between DMN and attention in TBI patients. 23
Sensorimotor Network
A significant SMN FC on attention was reported. 24 Healthy controls showed an inverse relationship, while TBI patients showed a correspondence between FC and attention, which varied between groups.
Dorsal Attention Network
Precentral gyrus-DAN connectivity and processing speed, precentral gyrus and DAN were linked, which suggests faster processing speed related to attention. 25 A positive relationship between DAN and TMT-A, measuring attention and processing speed, was observed in mTBI with CT/MRI positive scans also. 10
Salience Network
An increase in SN connectivity was linked with better task performance, 10 and the right insula was linked with attention scores. 23
Visual Network
A functional connectivity exists between the VN and the middle temporal gyrus, which is correlated with processing speed. 25
Resting State Networks Associated with Executive Functions
Frontoparietal Network
A significant relationship between frontoparietal network (FPN) connectivity and executive functions and BRIEF-A self-monitor scores was noted, whereas frontal assessment battery (FAB) scores showed an inverse relationship. 18
Default Mode Network
Significant relationships were reported between DMN connectivity and executive function, DMN and frontal assessment battery scores with number-letter task switching cost errors. 18 A relationship between DMN and executive function was observed. 21 Particularly, the FC was seen in relation to sustained attention and inhibition, as measured by the Stroop task. The reported results suggest that alterations in DMN connectivity may cause changes in overall executive functions.
Orbitofrontal Network
For mTBI patients with CT/MRI negative scans, an increase in connectivity in the orbitofrontal network, which was associated with better executive function performance, was observed. 10
Basal Ganglia Network
A reduced connectivity between the basal ganglia and orbitofrontal networks was correlated with executive function in patients with mTBI. 10
Visual Network
Right precuneus (within the VN) and executive scores positively correlated. 23
Resting State Networks Associated with Memory
Verbal learning and memory.
Default Mode Network. A positive association between lingual-DMN network connections and Auditory Verbal Learning Test (AVLT) scores. 26 SN-DMN network connection corresponds with AVLT scores, particularly AVLT4 scores. These findings suggest that enhanced connectivity within and between these networks is associated with improved verbal learning and memory performance. 27
Other Networks
A positive relationship between increased semi-acute connectivity within the occipito-cerebellar network and learning memory scores at 6 months after injury in the CT/MRI negative subgroup of mTBI patients. 10 A link between LN and visual memory was also noted. 27
Visuospatial Memory
Default Mode Network
An inverse relationship between posterior DMN-inferior frontal connectivity and complex figure tracing test performance. This finding suggests that enhanced connectivity between these networks is associated with poor visuospatial memory performance. 26
Working Memory
Salience Network
Salience-pre central network connectivity was positively linked with verbal n back (VnB) hits. Connections of the SN with DMN and precentral network were negatively correlated with VnB errors. The increased connectivity between SN and other regions is suggestive of better working memory performance. 26
Somatomotor Network
There is a positive connection between intrinsic functional connectivity in SMN and working memory scores. 28
Negative associations were reported between alterations in functional connectivity in DMN, DAN, VN, SMN, VAN and the working memory span. The finding suggests that the changes in functional connectivity are correlated with working memory performance in TBI patients. 25
Episodic Memory
Inverse relationships were also observed between alterations in functional connectivity in DAN and superior temporal gyri (STG) with episodic verbal memory. Limbic network and bilateral precuneus correlated with episodic verbal memory immediate recall (EVMI). DMN and precuneus associated with episodic verbal memory delayed recall (EVMD). Functional connectivity changes were observed between VAN and lateral occipital cortex (LOC) associated with episodic memory immediate recall (EVMI). 25
Discussion
This review explains the intricate association between the brain’s FC and cognitive domains from multiple studies on RSNs in TBI patients. DMN is the most widely explored RSN. The inverse relationship between DMN and FPN, as related to DMN and processing speed measures, indicates that task-positive network functions are interfered with by higher DMN connectivity. These varying relations are suggestive of compensatory mechanisms due to injury, influencing the DMN’s activity in both task-negative and task-positive performance. A positive pattern of association between FPN and executive functions was observed.
The contradictory patterns of links with different executive function tests, such as the Brief A and FAB, explain the complexity of executive functions and the need to assess cognitive functions from multiple aspects following TBI. The positive association between SMN and attention in TBI patients, and the negative association in healthy controls, indicates that alterations in FC are due to the injury. 24 The results suggest that FC, as a result of compensatory mechanisms, requires further research on maladaptive responses to injury. 24
The multiple network interactions emphasise the distributed nature of cognitive processing. The observed associations between RSN connectivity and cognitive performance suggest meaningful, though complex, brain behaviour relationships in TBI. 25 The consistent negative direction of these links is noteworthy and may indicate that reduced connectivity between certain regions correlates with better cognitive performance in TBI patients. The structural connectivity findings, particularly the negative links between right cingulum bundle integrity and sustained attention, present an intriguing and counterintuitive relationship. 24 This may suggest compensatory mechanisms where reduced white matter integrity leads to functional reorganisation, potentially improving cognitive performance. These findings collectively highlight the complexity of brain–behaviour relationships in TBI patients. The varying directions and strengths of associations across different networks and cognitive domains underscore the need for a nuanced understanding of post-TBI brain function. This integrative review synthesises conceptual and empirical patterns across neuroimaging studies rather than providing an exhaustive or systematic evaluation of the literature.
Implications for Future Research
Upcoming studies can focus on investigating the adaptive versus maladaptive nature of altered network connectivity in TBI patients, exploring the temporal dynamics of these relationships, considering both acute and chronic stages of TBI and examining how these network changes shift from group-level to individual-level analysis. Development of an individual connectome profile can be used to create an individualised rehabilitation module by identifying the disrupted network and target. The use of machine learning techniques for individualised data helps in predicting clinical outcomes. Additionally, multilayer and multiplex network models can be explored to simultaneously analyse the functional and structural connectivity.
Limitations
The available literature remains limited, which may affect the generalisability of the synthesised findings. Most available studies employed cross-sectional designs, limiting conclusions regarding longitudinal network changes and recovery trajectories. The heterogeneity of TBI severity across studies may have introduced variability in results, complicating the derivation of consistent conclusions. While cognitive domains like attention, working memory, verbal learning and executive functions were examined, the review may not have comprehensively addressed all cognitive functions affected by TBI. Despite all studies utilising rs-fMRI, variations in acquisition parameters, pre-processing and analysis methods could have affected the comparability of results. The review may not have explored the effects of age and sex on the disruptions of functional connectivity and its effects on cognitive impairment post-TBI. The neuropsychological tools used to assess cognitive functions may vary across research studies, which may affect the consistency of the findings reported. Furthermore, the absence of meta-analytic pooling means that confidence intervals and precise effect sizes cannot be reported. The certainty of findings varies across cognitive domains: DMN-attention and DMN-memory associations are supported by multiple independent studies and are therefore more reliable, while findings for networks such as the Basal Ganglia Network or Orbitofrontal Network rest on single studies and should be interpreted with caution. A significant limitation across included studies is the variability in the timing of neuroimaging assessments relative to injury onset. Acute, sub-acute and chronic TBI are each characterised by distinct neurobiological processes: early post-injury phases reflect oedema and diaschisis, while chronic phases reflect neuroplasticity and reorganisation. 16 The absence of a formal bias assessment tool is an additional limitation of this review; future systematic reviews in this area should employ standardised instruments such as the JBI critical appraisal checklist to appraise study quality. 20 The heterogeneity in imaging time points across studies makes it difficult to draw conclusions about stage-specific RSN alterations and their differential impact on cognitive outcomes. 10
Conclusion
In this review, the RSNs associated with attention, executive functions, visuospatial cognition and memory in TBI patients were explored. It is noteworthy that functional connectivity within and between DMN is a sensitive biomarker for early prognosis of TBI, as there are a notable number of studies available focusing on DMN. Further research is required to clarify the mechanisms underlying other RSN alterations, as well as their role in cognitive recovery following TBI. The evidence for neuroplasticity and recovery can be observed through the dynamic changes in the affected networks, but the exact reasons for hyperintensities of activation are unknown. Although additional analysis of studies is required to completely understand the alterations in these networks and their significance for cognitive performance to frame a rehabilitation strategy for recovery and reorganisation of disrupted connectivity, this review provides a foundational overview of the existing literature.
Footnotes
Acknowledgement
The authors gratefully acknowledge the support provided by Sri Ramachandra Institute of Higher Education and Research for facilitating this research.
Author’s Contribution
Ms Madhumathi P C: Conceptualisation, methodology, literature search, study selection, data extraction, formal analysis, writing; Dr Visvanathan K: Supervision, methodology, critical review of manuscript, review & editing; Dr Rajeswaran R: validation (fMRI—resting state networks aspect), critical review of manuscript, assistance in writing; Dr Rimjhim Agrawal: review of manuscript draft, validation (fMRI—RSNs aspects); Dr Vijayalakshmi: inputs on methodology, review & editing, inputs on cognitive functions aspects; Mr Varadharajan: guidance on methodology, assistance in study selection, review, validation (cognitive functions aspect).
Data Availability Statement
This study is a review of previously published literature. All data analysed in this review are available in the cited articles, which are included in the reference list.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Patient consent was not required as this study is an integrative review of previously published literature and did not involve human participants or collection of primary data.
Statement of Ethics
Not applicable.