
Abstract
Background
Autonomic regulation of the heart is commonly assessed using heart rate variability (HRV), which reflects beat-to-beat fluctuations in heart rate. Time- and frequency-domain HRV indices are known to vary with age, sex and environmental influences. However, existing reference values are largely derived from Western populations, underscoring the need for region-specific normative HRV data.
Purpose
This study aimed to develop comprehensive, region-specific reference values for HRV and to examine age- and gender-related differences in HRV indices in a predominantly South Indian population.
Methods
This cross-sectional observational study recruited 272 healthy adults aged 18–80 years, predominantly from South India. Five-minute resting ECG recordings were obtained for HRV analysis. Standard time- and frequency-domain HRV parameters were calculated. Data normality was assessed prior to analysis. Baseline comparisons were performed across gender and across three predefined age groups, followed by appropriate post hoc analysis. A prior power analysis was also conducted.
Results
Data from 249 healthy individuals were included in the final analysis. Normative reference values for time- and frequency-domain HRV parameters were established. Males exhibited lower resting heart rate and higher LF/HF ratio, whereas females demonstrated significantly higher root mean square of successive difference and percentage of successive RR intervals differing from the previous interval by more than 50 ms. Age-wise analysis revealed a more pronounced decline in mean RR interval beyond 30 years of age. Compared with individuals younger than 30 years, those older than 30 years showed significant reductions in HRV—particularly in time-domain parameters and frequency-domain indices.
Conclusion
This study provides 5-min HRV reference data for healthy adults from a predominantly South Indian population. Both age and gender independently influenced HRV indices, with an age-related decline in overall HRV and higher vagal tone observed in women compared to men. The observed deviations from international Task Force reference values suggest population-specific influences, potentially related to ethnicity, lifestyle and environmental factors. We advocate the generation of region-specific HRV data sets by different centres to get a holistic picture of region- and population-specific variations in HRV.
Keywords
Introduction
The autonomic nervous system (ANS) plays a key role in homeostasis. 1 The assessment of this limb of the nervous system is critical, since the ANS has been implicated in the pathophysiology of multiple disorders.2–6 Therefore, timely evaluation of this system can provide crucial insights for the diagnosis and management of clinical disorders. 7
Laboratory assessment of the ANS has been traditionally performed using an evaluation of autonomic tone and reactivity. The activity of the cardiac limb of the ANS at rest is evaluated using heart rate variability (HRV). HRV quantifies the perturbations in heart rate (or RR intervals) on a beat-to-beat basis using established mathematical indices.8–10 Autonomic reactivity is evaluated using a standardised group of tests proposed by Ewing et al.11, 12 Together, these tests provide a comprehensive picture of the ANS, and the robustness of these parameters has been evaluated in multiple works. 13
While Ewing battery has standardised cut-offs for various tests, 14 HRV parameters have demonstrated considerable variations across different populations and age groups. It has been shown that gender influences HRV, with females demonstrating post-pubertal parasympathetic predominance, which diminishes after menopause. 15 While some studies report higher time and frequency domain indices in males, while stronger nonlinear measures in females, others have found no significant sex-related differences in HRV among healthy adults. 16 Therefore, the available evidence on the influence of gender on HRV indices is evolving. Age is another important factor wherein progression of this variable has demonstrated sympathetic dominance accompanied by reduced baroreflex sensitivity and decreased HRV.17, 18 HRV indices, such as SDRR, root mean square of successive difference (RMSSD), and pRR50% (percentage of successive RR intervals differing from the previous interval by more than 50 ms) have been proposed as biomarkers of premature aging.
In view of the effect of physiological variables on HRV indices, it is recommended that large data sets should be generated for different centres to account for differences in populations and geographies. While large-scale data sets are available for Western populations,19–23 similar data sets from our country are lacking. This gap is critical because previous studies increasingly highlight the need for large-scale regionally inclusive reference standards, considering demographic, lifestyle, diet, climate, physical activity and regional differences. 24 In the Indian context, Abhishekh et al. provided one of the earliest data sets for short-term, age-related HRV references. 25 Thereafter, data sets have been generated to observe the effect of physical activity on HRV, 26 gender and adiposity. 27 Also, some studies have documented HRV parameters in large healthy subjects in different populations across India.15, 28 We also observed studies that have described age-specific ranges for autonomic reactivity parameters, 29 but did not address HRV indices. We observed a lack of comprehensive, region-specific HRV reference data, particularly in South India. Therefore, we conducted the present study to describe the range of HRV parameters in the South Indian population. In addition, we also attempted to explore the effect of age and gender on HRV indices.
Methodology
Study Design
Our study was cross-sectional and observational in nature, conducted in accordance with the STROBE 30 guidelines established by the EQUATOR network. The study was performed as per the guidelines of the Declaration of Helsinki. The research was approved by the institutional ethics committee of our institute. Written informed consent was given by all the participants before recruitment in the study.
Recruitment of the Participants
Apparently healthy adults (18–80 years), of either gender, were included in our study. Before inclusion in the study, a medical history was taken to rule out any co-existing illness, such as neurological/psychiatric disorders, diabetes mellitus, cardiovascular disorders and other chronic illnesses, that could have affected autonomic parameters. Also, subjects addicted to tobacco/alcohol or any other narcotic substance were excluded from the study. Documentation was made regarding the absence of co-morbidities. We took a history to rule out the presence of autonomic symptoms affecting the study subjects on a regular basis. These included, but were not limited to, excessive or reduced sweating, diarrhoea and/or constipation, postural dizziness or blackouts, dyspnoea at rest/exertion and excessive runny or dry nose. While one or more of these symptoms may happen occasionally across population, these symptoms are debilitating in patients with diseases involving ANS. After supine rest, vitals such as heart rate, blood pressure and respiratory rate were recorded. These components ensured that the study was apparently healthy at the time of inclusion in the study.
Data acquisition for all female subjects was performed between days 2 and 7 of the menstrual cycle. We excluded pregnant females and subjects taking oral contraceptive pills from the study, since these are known to affect autonomic tone.
On the day of the data acquisition, subjects were advised to abstain from tea/coffee/tobacco. Also, subjects were advised to avoid any heavy physical activity within 24 h of testing.
Data Acquisition
Upon arrival to the AFT lab, the subject was requested to empty their bladder. Before data acquisition, subjects were explained about the study protocol and a supine rest of 10 min was provided. All recordings were done in spontaneous (free) respiration. We chose spontaneous breathing as there is a large corpus of literature that recommends its use over metronomic breathing.13, 31 Lead II ECG was recorded using single-use disposable adhesive Ag-AgCl electrodes. Data were acquired using digital data acquisition system (Power Lab C™ system, AD Instruments, Australia). Low- and high-pass filters (0.5 and 35 Hz) were applied to the raw ECG signal to reduce noise and ensure good signal quality.
Heart Rate Variability Analysis
HRV analysis was performed with Lab Chart™ software version 8 (AD Instruments, Australia). Then the data were visually inspected to exclude any artefacts. A 5-min clean segment of ECG signal was utilised for HRV analysis. All analyses were done by an observer to prevent inter-observer bias. Time domain and frequency domain HRV measures were derived according to Task Force guidelines. 8 From the RR intervals, the following time domain measures were calculated, that is, average heart rate (average HR), average RR interval based on RR intervals (average RR) and RMSSD as the square root of the mean squares of successive intervals between adjacent RR intervals and pRR50%. Fast Fourier Transformation spectral analysis was used to derive frequency domain parameters like Powers in VLF (0–0.04 Hz), LF (0.04–0.15 Hz) and HF (0.15–0.4 Hz) bands; total power; normalised powers in LF and HF bands (LF nu and HF nu, respectively) and LF/HF ratio. These indices are extensively reported in the scientific literature.32–35
Statistical Analysis
Data were analysed using R software 36 (R4.5.2) and JASP™ software. 37 The normality of the data was determined by applying the Kolmogorov–Smirnov goodness-of-fit test. Based on distribution, parameters are expressed as mean ± SD or median (IQR). Baseline comparisons between the groups were performed using Welch two-sample t-test or one-way analysis of means (not assuming equal variances), ANOVA. A p value of .05 was taken for statistical significance. Post hoc analysis using Tukey’s honestly significant difference test was performed. Power was calculated using the power.f.regression() function from the ‘pwrss’ R package. 38
Results
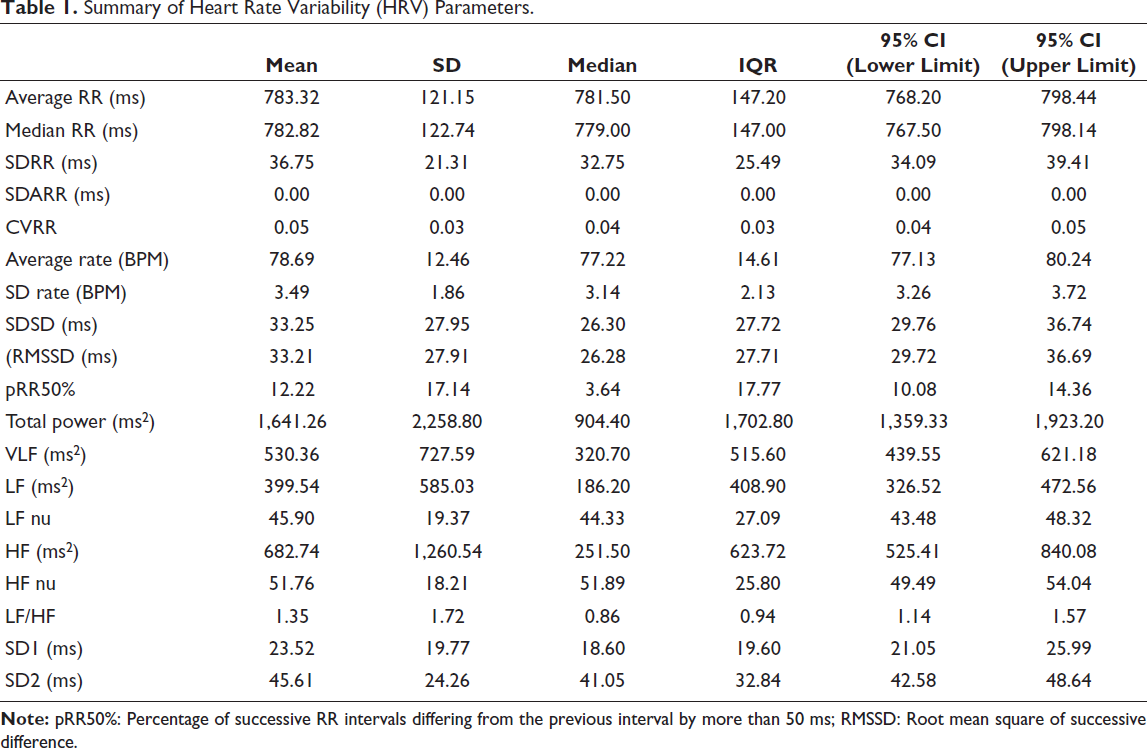
We acquired data from 272 healthy subjects. Data of 23 subjects were rejected due to artefacts, noise or poor signal quality. Consequently, 249 healthy adults in the age group of 18–80 years (mean age = 42 ± 15 years) are presented in the current work. Participants were in the majority from Telangana and Andhra Pradesh (n = 194), followed by Kerala (n = 23), Tamil Nadu (n = 11), Karnataka (n = 1) and other states (n = 20), who were residents of Telangana for the past 2 years. Since age was significant at baseline, participants were categorised into three groups based on age, that is, <30 years (n = 67), 30–59 years (n = 136) and 60 plus years (n = 46) to assess its interaction with HRV (Supplementary Table 1). Summary of HRV parameters is shown in Table 1.
Summary of Heart Rate Variability (HRV) Parameters.
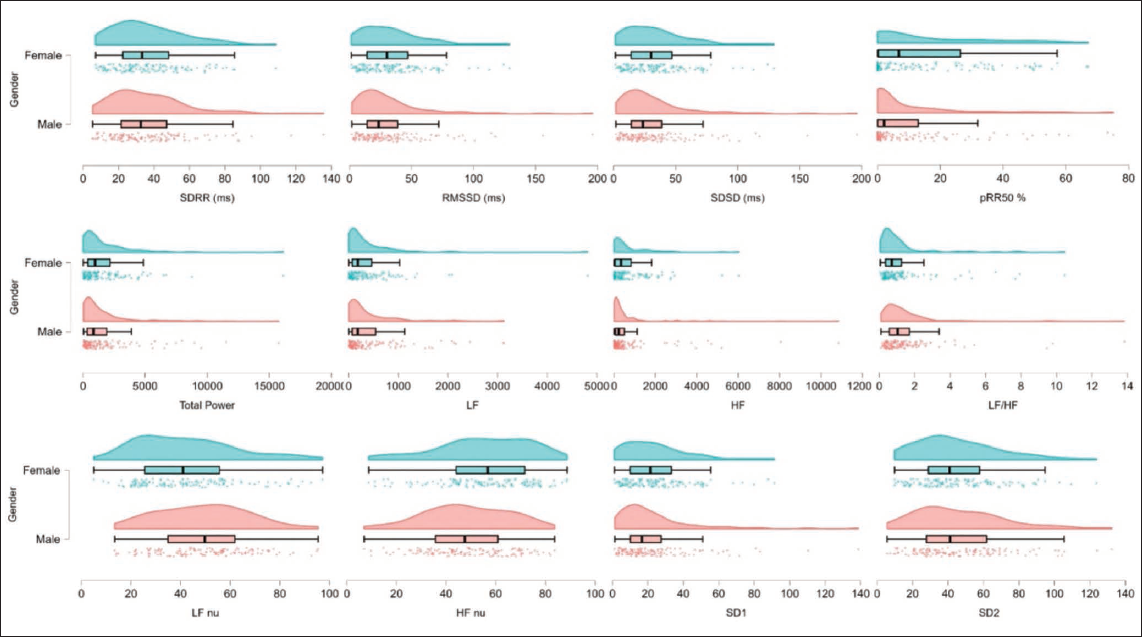
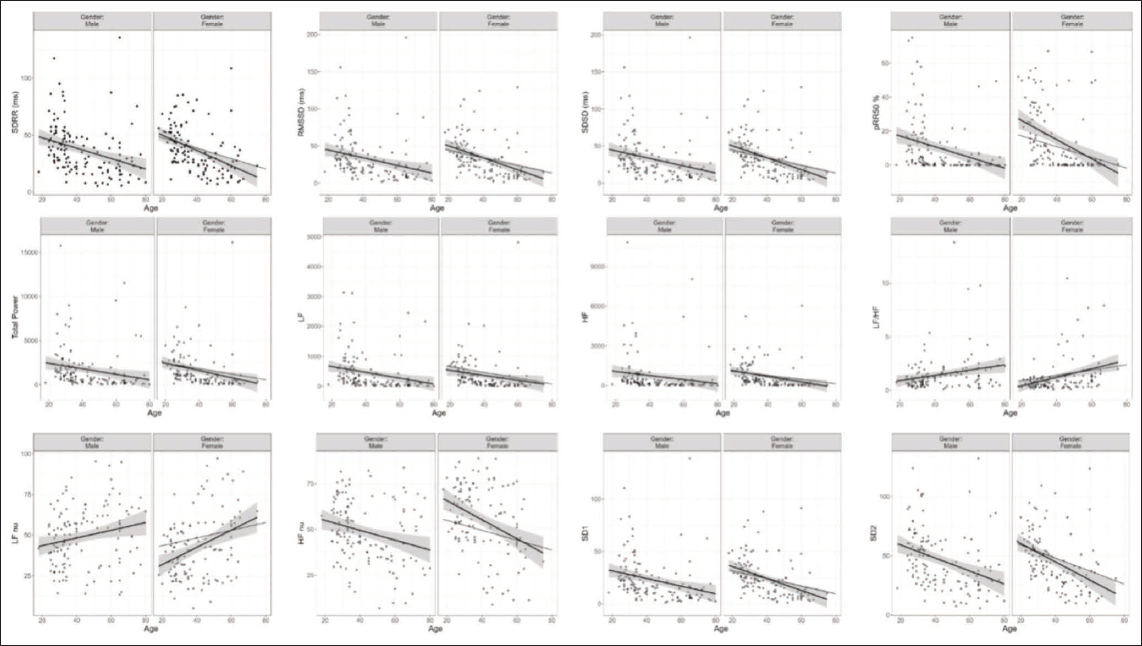
In addition, we segregated study participants according to gender, that is, 130 males and 119 females. Distribution of HRV parameters according to gender is shown in Figure 1. Gender wise differences of all the HRV parameters are summarised in Table 2, and linear regression plots between age and HRV parameters clubbed according to gender is shown in Figure 2. Significant gender differences in several HRV measures were seen. Males had a higher average RR interval (804 ± 127 ms) compared to females (761 ± 110 ms). This is corroborated by the mean heart rate, which was lower in males (77 ± 12 bpm) than in females (81 ± 11 bpm). RMSSD showed a marginally higher value in females (34 ± 26 ms) compared to males (32 ± 30 ms). Similar trends were seen in pRR50%, with females having higher values compared to males. In the frequency domain, the total power, LF and HF components were higher in males, though with considerable variability. Notably, LF normalised units (LF-nu) were higher in males (49 ± 18), while HF-nu in females were higher (55 ± 19). The LF/HF ratio showed a slightly upward trend in males (1.48 ± 1.78) compared to females (1.21 ± 1.64). Significant interaction with gender was observed with average RR, average HR, pRR50% frequency domain parameters, such as absolute and log converted values of LF and HF.
Effect of Age and Gender on Heart Rate Variability (HRV) Indices.
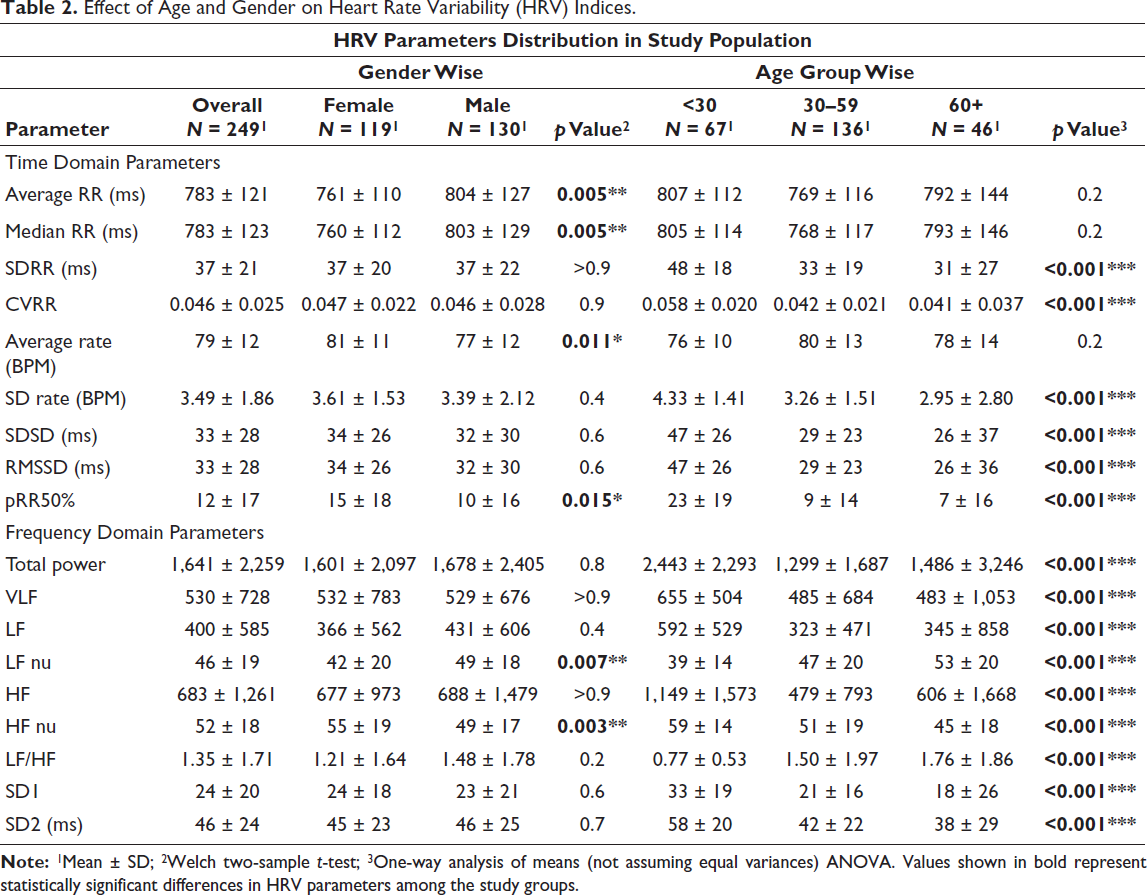
We compared HRV indices between three age groups, that is, age <30 years (n = 67), age between 30 and 59 years (n = 136) and age >60 years (n = 46) (Table 2). The average RR interval was relatively stable in younger subjects, showed a decline after the third decade and later with a slight increase in the oldest group. The average heart rate increased gradually with age, peaking in the 30–59 age group before declining in the oldest age group. Time-domain indices, including SDRR, RMSSD and pRR50%, showed a gradual decline with increase in age. Total power also decreased notably with age, with a minor rebound in the oldest group. While considering frequency domain, LF nu showed a gradual rise, HF nu declined consistently and the LF/HF ratio depicted an increasing trend with age, reflecting a shift towards sympathetic predominance. ANOVA revealed significant impact of age on SDRR, RMSSD, pRR50%, LF nu, HF nu, LF/HF and total power (Supplementary Table 2). Given the significant one-way ANOVA, post hoc analysis using the Games–Howell test (Supplementary Table 3) was conducted to identify which specific age groups differ significantly. It was found that there was a significant change in HRV parameters after 30 years compared to the less than 30 years group, especially in parameters like RMSSD, pRR50%, LF nu, HF nu, LF/HF and total power.
We evaluated power to detect R² (and R² change) for the normative analysis with an alpha of 0.05. Expected R² values for the HRV parameters were taken from literature/pilot estimates (SDNN 0.15, RMSSD 0.18, pNN50 0.12; additional parameters: LF, HF, LF/HF with expected R² 0.20, 0.16, 0.14). With n = 249, the study is well powered (>0.90) to detect main effects of age and to fit full age + sex models for moderate-to-large R² values (≈0.12–0.20) (Supplementary Table 4). The sample size and power analysis were done using the ‘pwr’ package in R. The details are provided in the Supplementary Appendix, Supplementary Table 4 and Supplementary Figures 1 and 2.
Discussion
This study provides reference values for resting HRV in a healthy South Indian population aged 18–80 years, highlighting the influence of both age and gender. Advancing age was found to be associated with a gradual reduction in overall HRV and parasympathetic activity, most evident after the 30s, accompanied by a relative increase in sympathetic drive. Gender differences were clear, with males depicting a higher sympathetic tone and females depicting greater parasympathetic activity. Overall, these findings suggest that age and gender significantly influence HRV patterns.
Establishing population-specific reference values for resting HRV is essential, as autonomic function can differ across regions and ethnic groups.15, 24 Our results are largely in agreement with normative resting values reported in the Indian population.15, 25, 39 There were slight differences in HRV parameters when compared with data from non-Indian populations, possibly reflecting variation in age distribution, lifestyle 40 and regional factors.41, 42 When compared with Task Force normative data showed a markedly lower SDRR (37 ± 21 vs 141 ± 39 ms).24, 43 Both RMSSD (33 ± 28 vs 27 ± 12 ms) and HF nu (52 ± 18 vs 29 ± 3) were higher in our cohort. These findings support earlier findings from studies conducted in India on HRV and may point towards relatively preserved or even enhanced parasympathetic activity, particularly among younger and more physically active individuals.15, 26, 44 On the other hand, LF nu (46 ± 19 vs 54 ± 4), total power (1,641 ± 2,259 vs 3,466 ± 1,018 ms2), and LF/HF ratio (1.35 ± 1.71 vs 1.5–2.0) were lower compared to task force normative values. Taken together, these findings highlight the value of region-specific reference data sets for precise interpretation of HRV indices. This finding also highlights the need for a globally accepted standard recording duration for HRV assessment, along with validation of comparability across different recording durations.10, 45
In terms of gender differences in HRV metrics, our study found that females depicted a higher resting heart rate compared to males. This variation cannot be attributed solely to sympathetic activity as difference in heart size between genders may also play a role. However, since heart size is closely associated with body mass index, this relationship requires further investigation. 23 Interestingly, heart rate differences between men and women appear to vary as a function of HRV, underscoring the complex interplay between autonomic regulation and neural mechanisms in shaping gender-specific cardiac function. 46 Despite the higher resting heart rate, females demonstrated greater vagal activity, reflected in higher RMSSD, pRR50% and HF nu values, along with lower LF nu and LF/HF ratios in comparison to males. These observations are similar to earlier reports from both Indian and international cohorts.15, 18, 47–49 Hormones, particularly estrogen and oxytocin, play an important role in modulating sinus node function and autonomic regulation, contributing to the higher vagal activity seen in premenopausal women. 18 This also may be attributed to greater acetylcholine sensitivity, slower breakdown of acetylcholine, and enhanced cortical thickness in regions regulating vagal outflow.46, 50
The findings from our study point towards a gradual weakening of parasympathetic function over time, reflecting a progressive decline in autonomic control of the heart with advancing age. The trend can be seen in Figure 2, wherein all HRV parameters show a decline with age with the exception of LF, a marker of sympathetic activity. At rest, the healthy heart is largely under parasympathetic regulation, mediated by fast-conducting, myelinated vagal fibres that modulate heart rate in under a second.51, 52 Therefore, time-domain measures such as RMSSD and pNN50, along with the high-frequency (HF) component in frequency-domain analysis, are considered strong indicators of vagal tone. In our study, parasympathetic indices including SDRR, RMSSD, pRR50% and HF nu showed a significant decline with age, consistent with earlier reports of age-related vagal withdrawal.52, 53 We found that the progressive decline in these markers was most pronounced after the third decade of life, indicating reduced overall variability and vagal modulation. Such changes may have been due to factors affecting myelination of vagal fibres, structural alterations in the sinoatrial node, reduced receptor responsiveness and neurotrophic support.18, 23, 54 Parallel to the decline in parasympathetic activity, our study supports earlier evidence of sympathetic predominance with ageing. 17 Both LF power and the LF/HF ratio showed a significant increase with age, reflecting a relatively dominant sympathetic drive. This sympathetic override was especially evident after the 30s, coinciding with the decline in vagal indices and overall HRV. While we did not explore the causal mechanisms behind these changes, multiple mechanisms have been reported in the literature.23, 55, 56 These intrinsic changes might be further shaped by external influences such as post-COVID autonomic changes. 57 The relatively small subgroup sizes in the present study offer preliminary insights into autonomic variations58, 59 and require confirmation in larger, adequately powered cohorts. Our data set includes participants with ages up to 80 years, which has not been explored in previous studies.18, 25
Conclusion
This study focused on short-term HRV metrics for adults in the South Indian population, spanning from early adulthood to the elderly age group. The strength of our study is in its broader age coverage, which allowed a clear assessment of the impact of age and gender separately on HRV. Our study distinctly shows an age-related decline in overall HRV parameters, particularly those influenced by parasympathetic activity. In addition, our data further support the notion of gender differences in HRV parameters, with women showing higher vagal tone than men. Based on findings in the present work, we are able to provide a normative data set of HRV indices for a large population from South India at our centre. We hope that this data set will help in providing a reference range for future studies exploring HRV in both basic science and clinical domains.
Limitations
Although the overall sample size was reasonably large, the number of participants within individual age groups was relatively small. Studies with larger, well-powered cohorts are, therefore, needed to better understand the interaction between age and sex on HRV. The cross-sectional nature of the study also limits causal interpretation of age-related changes in autonomic function. In addition, body composition parameters, such as body mass index, were not assessed, restricting adjustment for potential physiological confounders when interpreting age- and sex-related differences. Future longitudinal studies with larger samples and detailed anthropometric profiling would allow more robust normative data and enhance the clinical relevance of HRV reference values.
Footnotes
Acknowledgements
The authors sincerely thank Mr Arun, Mrs Pranali, and Mrs Abhirami (Nursing Officers), and Mr Vinay Technician, for their invaluable assistance and active involvement in completing this project. They also extend their gratitude to Mr Sumanth, Mr Harish, and Mr Pravesh from ADI Instruments for their technical support.
Author’s Contribution
Anish Singhal: Conceived and designed the study, prepared the ethics documents, developed protocol, coordinated the study, participant recruitment and data collection, quality checks, statistical analysis and writing, data interpretation, initial draft of the manuscript.
Athira M. Das: Prepared the ethics documents, developed protocol, coordinated the study, participant recruitment and data collection, quality checks, statistical analysis and writing, data interpretation, initial draft of the manuscript.
Vishnu Akhil Raj Kumar Y: Designed the study, prepared the ethics documents, developed protocol, coordinated the study, participant recruitment and data collection, quality checks, statistical analysis and writing, data interpretation, initial draft of the manuscript.
Arun Mitra: Developed protocol, coordinated the study, participant recruitment and data collection, quality checks, statistical analysis and writing, data interpretation, initial draft of the manuscript.
Shival Srivastav: Quality checks, statistical analysis and writing, data interpretation, initial draft of the manuscript.
Billa Anala, Arijit Sarkar, Kalpana M, Taranikanti Madhuri, Nitin Ashok John: participant recruitment and data collection, quality checks, statistical analysis and writing, data interpretation, initial draft of the manuscript.
All authors reviewed and commented upon the initial draft and approved the final manuscript.
Consent Statement
Written informed consent was obtained from all participants after explaining the nature and purpose of the study.
Data Availability Statement
The data sets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written informed consent was obtained from all participants for participation in the study and publication of the findings. All data were anonymized, and participants were informed that the published article would be freely accessible online.
Statement of Ethics
The research was conducted as per the Declaration of Helsinki guidelines. The study protocol was approved by the institutional ethics committee on human research and ethical review board of our institute (IEC Ref.No: AIIMS/BBN/IEC/July/2025/789-R).
Supplementary Material
Supplementary material for this article is available online.