
Abstract
Background
The menstrual cycle involves cyclical fluctuations in ovarian hormones that produce phase-dependent changes in neurocognitive function, emotional regulation, pain sensitivity and physical performance. Yet most therapeutic interventions, including yoga, apply uniform practices across the cycle, overlooking these physiological transitions. A phase-specific yoga approach may better accommodate these hormonal changes.
Purpose
This study aimed to develop, content-validate and assess the feasibility of a four-phase, menstrual cycle-specific yoga module to support menstrual health.
Methods
The study had three phases. (a) The development phase involved a systematic review of classical and contemporary yoga texts alongside relevant scientific literature. (b) In the validation phase, 11 experts validated the module using a three-point Likert scale; content validity was established using Lawshe’s Content Validity Ratio (CVR). (c) Feasibility was tested in a pre-post pilot study among female university students with premenstrual syndrome (PMS). 15 participants completed an 8-week intervention comprising five sessions per week. Outcomes included intervention fidelity, face validity, PMS symptom severity and PMS-related quality of life (PMS-QoL).
Results
The validated module retained 12/21 practices for the menstrual phase, 30/31 for the follicular phase, 25/33 for the ovulatory phase, and 19/28 for the luteal phase (all CVR > 0.59). The feasibility study demonstrated 100% acceptance and retention with no adverse events. Practices were rated easy to learn, with minor modifications required for some postures. High satisfaction and perceived benefits were reported for managing phase-related difficulties, emotional regulation, mood, strength, flexibility and balance. After 8 weeks, PMS symptoms decreased significantly, and PMS-QoL improved across physical, emotional and social domains.
Conclusion
The four-phase, menstrual cycle-specific yoga module was feasible, acceptable and associated with preliminary improvements in PMS symptoms and PMS-QoL. Aligning yoga practices with phase-dependent psychophysiological changes may offer a physiology-informed strategy for promoting menstrual health. Further controlled trials in broader eumenorrheic populations are warranted.
Introduction
Menstrual health is an integral component of overall female health and well-being across the reproductive lifespan, from menarche to menopause. In relation to the menstrual cycle, it can be defined as a state of complete physical, mental and social well-being, rather than merely the absence of disease or infirmity, and encompasses the ability to manage menstruation safely and comfortably while participating fully in everyday activities. 1 Menstruation is a fundamental physiological process regulated by highly coordinated interactions of the hypothalamic–pituitary–ovarian (HPO) axis and associated hormonal feedback mechanisms. 2 Fluctuations in ovarian hormones across the menstrual cycle have been associated with phase-dependent changes in mood, subjective symptoms, and select cognitive domains, including attentional and spatial–anticipatory processes.3–5
Each phase of the menstrual cycle is associated with distinct hormonal profiles and psychophysiological demands. The menstrual phase is commonly marked by reduced energy, heightened pain sensitivity and increased need for rest and recovery. 6 The follicular and ovulatory phases are characterised by rising oestrogen levels, improved mood, enhanced neuromuscular coordination and greater physical capacity, supporting engagement in more dynamic and strength-oriented activities. 7 In contrast, the luteal phase involves an initial rise followed by a decline in progesterone levels, which is often associated with heightened emotional sensitivity, fatigue and somatic discomfort in some individuals. 3 These phase-dependent changes suggest that interventions synchronised with menstrual phase-specific physiology may offer greater clinical effectiveness, safety and acceptability than approaches applied uniformly across the month. Such interventions are relevant primarily for eumenorrheic women aiming to maintain optimal menstrual health, and may also benefit those experiencing common conditions such as primary dysmenorrhea (prevalence: 46%–76%) and premenstrual syndrome (PMS; prevalence: 40%–71%). 8 These conditions can substantially impair QoL, academic and occupational performance and day-to-day functioning, highlighting the need for accessible, physiology-informed strategies to support menstrual well-being.
Yoga, as a holistic mind-body discipline 9 and widely practised complementary and alternative medicine (CAM) modality, 10 is particularly amenable to being structured around cyclical physiological patterns. By integrating physical postures, regulated breathing, relaxation techniques and meditative practices, yoga has been shown to influence autonomic balance, stress regulation, emotional processing, musculoskeletal function, mindfulness and subjective well-being—mechanisms directly relevant to menstrual health. 11 Existing yoga intervention protocols for menstrual complications, including polycystic ovarian syndrome (PCOS) 12 and dysfunctional uterine bleeding, 13 have consistently adopted a uniform set of practices across the entire menstrual cycle. Even validated yoga modules for specific female populations, such as postpartum NICU mothers, 14 primary dysmenorrhea, 15 premenstrual syndrome (PMS) 16 and hypothyroidism, 17 have similarly adopted a uniform structure without differentiating content or intensity by menstrual phase. Consequently, the potential added benefit of systematically tailoring yoga practices to the distinct hormonal and symptom profiles of each menstrual phase remains largely unexplored.
Despite the theoretical and clinical relevance of menstrual phase–specific approaches, no rigorously developed and validated yoga module currently exists that systematically aligns yogic practices with the four phases of the menstrual cycle. Structuring such a module across follicular, ovulatory, luteal and menstrual phases more closely reflects underlying hormonal trajectories and transition points. This allows precise adjustment of posture selection, intensity, breath work and relaxation practices to align with phase-specific symptomatology and functional capacity. Accordingly, the present study aimed to systematically develop and content-validate a four-phase, menstrual cycle-specific yoga module designed to support female menstrual health. Further, feasibility, safety and preliminary effects were assessed among female university students with moderate to severe PMS. By establishing feasibility within a cyclic, hormone-sensitive condition, this work seeks to provide a foundation for future research exploring the applicability of this module in healthy female populations and across other menstrual disorders characterised by regular ovulatory cycles.
Methods
This study was conducted in three phases following a standardised methodology for development, validation and efficacy assessment of a novel yoga module. The module was specifically designed to align with menstrual phase-related physiological variations. It aimed to address the psychophysiological challenges experienced by women with PMS and alleviate symptoms that predominantly occur during the luteal phase.
Phase I: Development of the Yoga Module
To identify appropriate yoga practices capable of addressing the challenges of each phase of the menstrual cycle, and to promote overall well-being, two authors meticulously reviewed four seminal yoga texts. The classical sources included Hatha Yoga Pradipika, 18 Gheranda Samhita, 19 Hatharatnavali 20 and Hatha Tattva Kaumudi, 21 and one contemporary yoga text—Asana Pranayama Mudra Bandha. 22 Additionally, a comprehensive literature search identified yoga-based studies addressing female-specific conditions, including PMS and primary dysmenorrhea. Studies addressing comorbid conditions affecting menstrual health, such as anxiety, depression, migraine, hypothyroidism and obesity, were also reviewed. The search was conducted across PubMed, Scopus, Web of Science and Google Scholar.
Based on evidence from classical texts and contemporary research, a curated set of yoga practices was developed to address the psychophysiological challenges of each phase, reduce stress and improve quality of life (QoL). Each phase included a specific set of practices. Core components across phases included: (a) Sukshma vyayamas (Loosening practices); (b) Suryanamaskara (sun-salutation), excluding the menstrual phase; (c) Swasha-kriya (breathing practices); (d) Asanas (physical postures) encompassing standing, balancing, sitting, twisting, forward and backward bending, prone and supine postures; (e) Vishratmak abhyasa (relaxation practices); (f) Mudras (gestures); (g) Pranayamas (voluntary regulated breathing); and (h) Om chanting. In addition, Gatiyatmak Sukshma vyayama (Dynamic loosening practices) were incorporated specifically during the follicular and ovulatory phases.
Phase-specific Practice Design
The practices aimed to foster natural harmony across the menstrual cycle. Yoga interventions were aligned with phase-specific hormonal and psychophysiological changes. Each phase included practices tailored to its characteristic physical, mental and energetic state of the body. The design also considered phase-related variations in energy and functional capacity.
Menstrual Phase
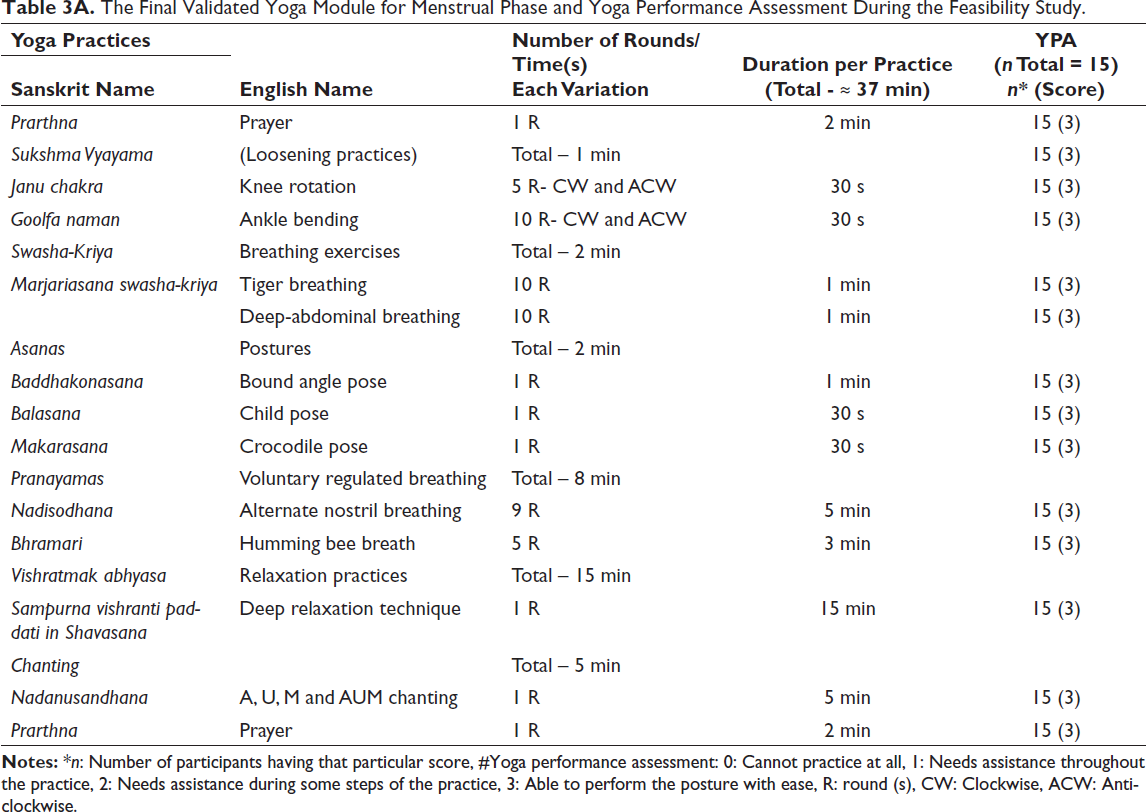
The menstrual phase is commonly associated with lethargy, low energy and heightened pain sensitivity. It is often accompanied by fatigue, abdominal discomfort and generalised body aches.23, 24 To address these characteristics, the practices chosen were slow, gentle and restorative, with emphasis placed on the pelvic region, lower abdomen and lower back. Greater focus was given to relaxation and chanting practices to promote comfort and ease, such as Tiger breathing, Deep abdominal breathing, Baddhakonasana, Deep relaxation technique and Nadanushandhan.
Follicular Phase
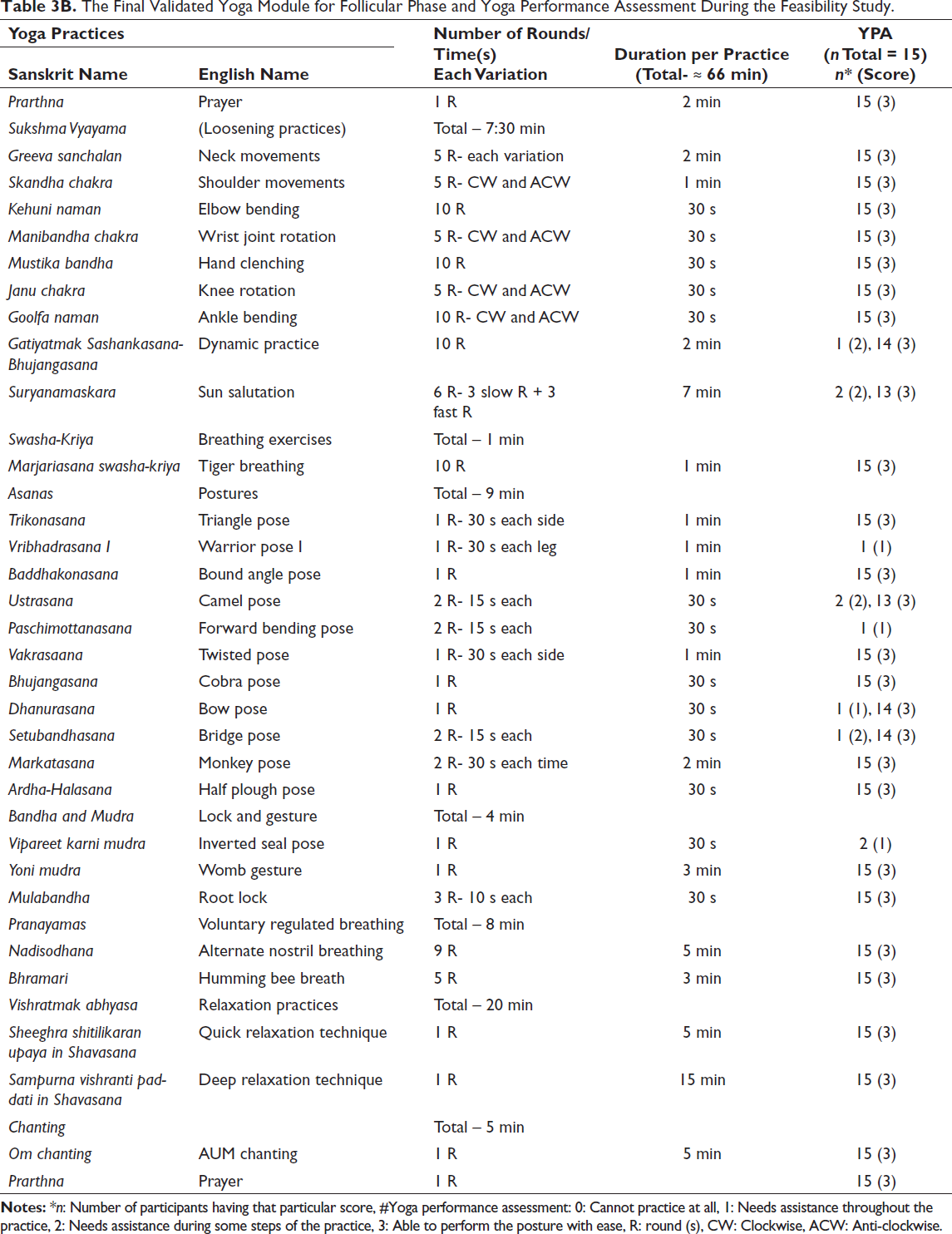
The follicular phase marks a preparatory stage characterised by endometrial proliferation and rising oestrogen levels.7, 24 This hormonal shift is associated with increased energy, improved neuromuscular capacity and reduced negative emotional reactivity.7, 24 It supports improved motivation, focus, and a positive mental state.24, 25 Practices were designed to enhance vitality, concentration and flexibility. Dynamic movements were incorporated to match improved physical capacity. These included Gatiyatmak Shasankasana-Bhujangasana, Suryanamaskara and balancing and twisting postures. Selected pranayama techniques and meditation supported mental clarity.
Ovulatory Phase
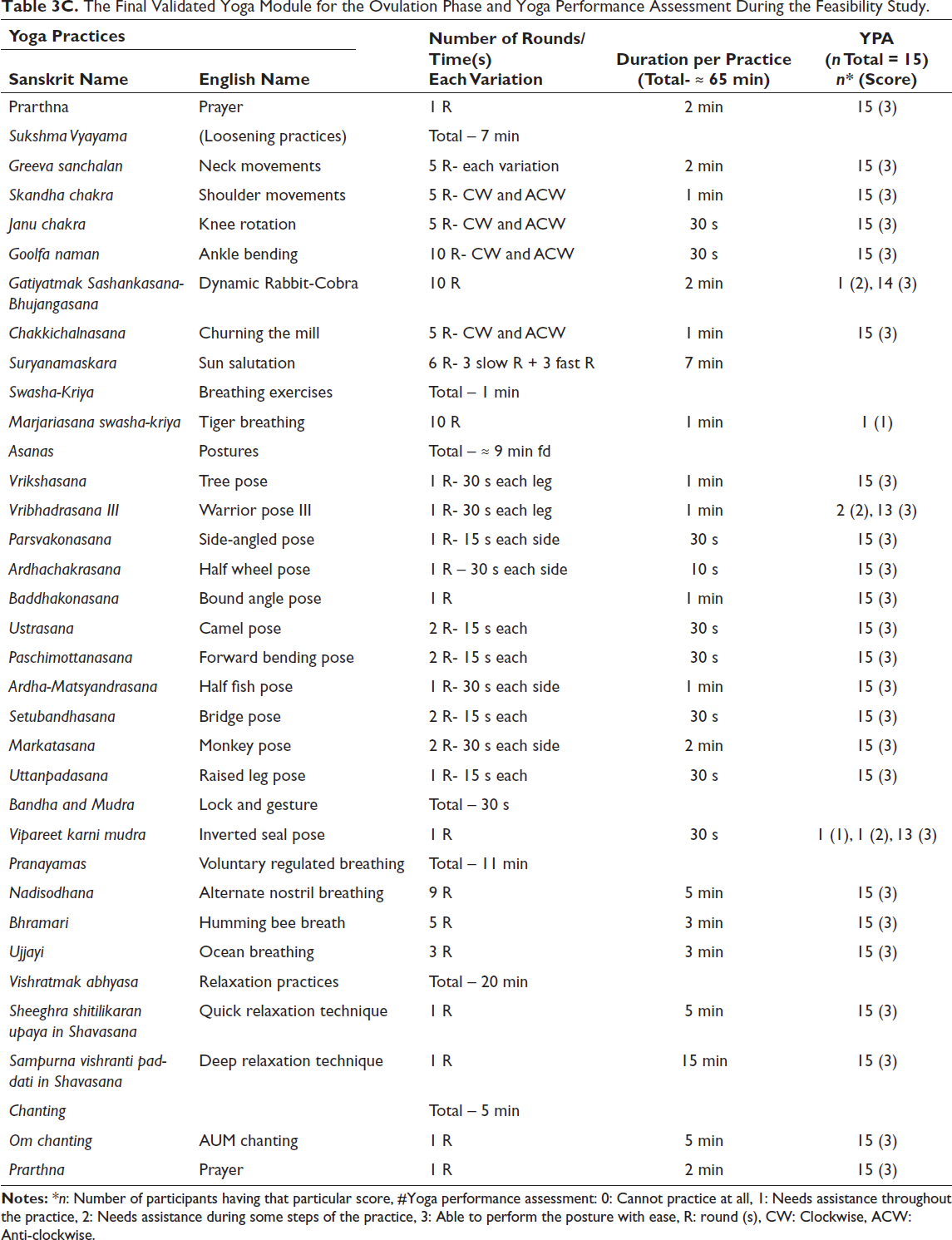
The ovulatory phase typically occurs between days 9 and 14 of the cycle. It is characterised by enhanced flexibility, 26 peak external physical load capacity 27 and perceived peak energy and strength readiness, 28 elevated mood, motivation and cognitive sharpness. 24 To support these attributes, practices chosen for this phase were comparatively more dynamic and physically demanding. The practices included were Chakki Chalanasana, Suryanamaskara, Paschimottanasana, Virbha-drasana II and III and Ardha Matsyendrasana.
Luteal Phase
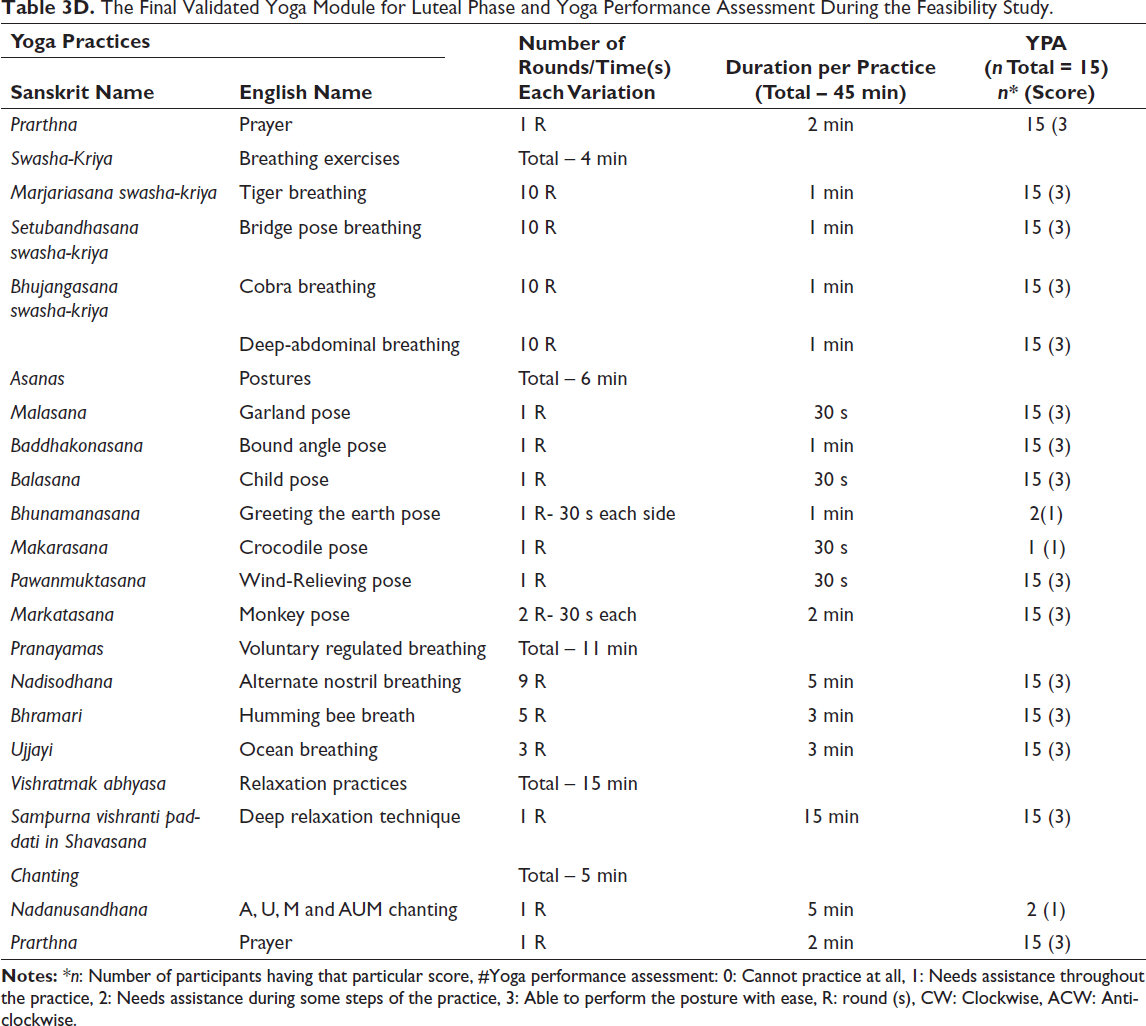
The luteal phase is characterised by elevated progesterone levels and is often associated with premenstrual symptoms such as emotional sensitivity, reduced energy, decreased libido, pain and psychological distress.24, 29 Practices during this phase were therefore designed to mitigate stress, regulate emotions, stabilise internal physiological processes, support and enhance cognitive function. Moderate-intensity practices were used to avoid overexertion, including slow Sukshma vyayama, gentle rounds of Suryanamaskara, increased emphasis on breathing techniques, simple asanas such as Baddhakonasana and Bhunmanasana and relaxation.
Phase II: Content Validation of the Module
A total of 15 experts were requested to participate in validating the developed yoga module. Eligibility criteria included: (a) possession of a postgraduate degree in yoga or BNYS certification, (b) gynaecologist with knowledge of yoga (c) a minimum of 5 years of professional experience in yoga research, teaching or therapeutic practice.
Experts received a structured validation form via email. The form included study objectives and a detailed list of proposed practices along with their underlying rationale. Experts rated each item using a three-point Likert scale (0: not necessary, 1: useful but not essential, 2: essential). Additionally, a section for optional comments and suggestions was provided for qualitative feedback (Supplementary File A).
Content validity for each practice was assessed using Lawshe’s Content Validity Ratio (CVR) method:30, 31
where Ne is the total number of experts rating a practice as ‘essential’, and N is the total number of experts.
Phase III: Feasibility Testing of the Validated Yoga Module
Although the four-phase yoga module was developed for the general eumenorrheic population, the pilot study was conducted among 15 participants with PMS using a pre-post study design. PMS occurs in females with regular menstrual cycles and intact ovulatory function. This makes it a suitable model condition for testing an intervention explicitly structured around menstrual phase physiology. The feasibility of such a module in a menstrual disorder such as PMS can be directly translated to healthy eumenorrheic populations.
Study Participants and Setting
This study was conducted among female university students at the Central University of Rajasthan between May and August 2025. A preliminary PMS screening survey was conducted in the girls’ hostels during January and February 2025. In total, 550 students were screened for eligibility, of whom 130 met the inclusion and diagnostic criteria for PMS. Finally, 15 consenting participants with PMS were enrolled in this pilot feasibility study.
Inclusion and Exclusion Criteria
The following are the inclusion criteria: (a) consenting female university students residing in campus hostels, aged 18–30 years; (b) females who fulfil Premenstrual Syndrome Screening Tool (PSST) criteria for moderate to severe PMS; and (c) unmarried status. Exclusion criteria for the study participants are as follows: (a) females with diagnosed gynaecological disorders, irregular or infrequent menstruation or existing psychiatric or psychological conditions; (b) overweight or obesity; (c) long term medication use or history of major surgery within the previous year; (d) history of substance abuse or addiction (e.g., smoking or alcohol); and (e) prior exposure to yoga practices within the past 6 months.
Intervention
The final validated yoga module was implemented through a structured intervention comprising 40 supervised sessions delivered over 8 weeks (five sessions per week). Each participant received approximately 7 sessions in the menstrual phase, 11–12 sessions in the follicular phase, 8–9 sessions in the ovulatory phase and around 13 sessions in the luteal phase. Sessions were offered at two times: one in the morning and two in the evening, to accommodate the participants’ academic schedules. All sessions were conducted by four certified yoga instructors. Sessions were held in designated classrooms within the Department of Yoga. The setting ensured adequate lighting and a distraction-free environment. Phase-specific sessions were conducted simultaneously across menstrual cycle phases.
Session Management and Instructor Training
At any given time, phase-specific sessions—menstrual, follicular, ovulatory and luteal—were conducted simultaneously, each led by a different instructor. To ensure consistency and minimise instructional variability, instructors underwent structured training before the intervention. Training focused on phase-specific practice rationale, appropriate pacing and intensity, voice modulation, participant observation and safe execution of practices, understanding the selection of dynamic practices during the follicular and ovulatory phases and restorative practices during the menstrual and luteal phases.
Participant Tracking and Adherence
Individual menstrual cycles were monitored using a detailed electronic tracking system to ensure accurate phase-specific allocation of participants. Attendance registers were maintained throughout the intervention to monitor adherence and confirm participation across all four menstrual phases, which was essential for evaluating feasibility and intervention fidelity.
Assessments and Tools
Participants were screened for PMS using the PSST to identify moderate-to-severe PMS. Feasibility and face validity were assessed following Bowen et al.’s framework, covering the following domains: (a) Acceptability, (b) Demand, (c) Implementation, (d) Practicality, (e) Adaptation, (f) Integration, (g) Expansion and (h) Limited efficacy. 32 Participants rated their experiences and perceived usefulness of the practices using a three-point Likert scale. Intervention fidelity was evaluated based on acceptance, attrition, retention rate and adverse events. Outcome measures included the Premenstrual Syndrome Scale (PMSS) and the premenstrual syndrome-related quality of life (PMS-QoL), assessed at baseline and after 8 weeks. Assessments were conducted during the luteal phase, confirmed using self-administered ovulation predictor kits (Easy@Home), which detect the luteinising hormone surge 24–48 h before ovulation. 33
Statistical Tools
Content validity for each yoga practice was assessed using Lawshe’s CVR. Socio-demographic characteristics were summarised using descriptive statistics. Data normality was evaluated using the Shapiro–Wilk test. Pre- and post-intervention changes were analysed using paired t-tests. Missing data were managed using the ‘mean of the nearby points’ method. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA).
Results
Phase I: Development of Yoga Module
Following a comprehensive review of the seminal and contemporary texts, relevant scientific literature and expert consultations, a set of yoga practices was identified for inclusion and further validation across the four menstrual phases—menstrual, follicular, ovulatory and luteal.
Phase II: Validation of Yoga Module
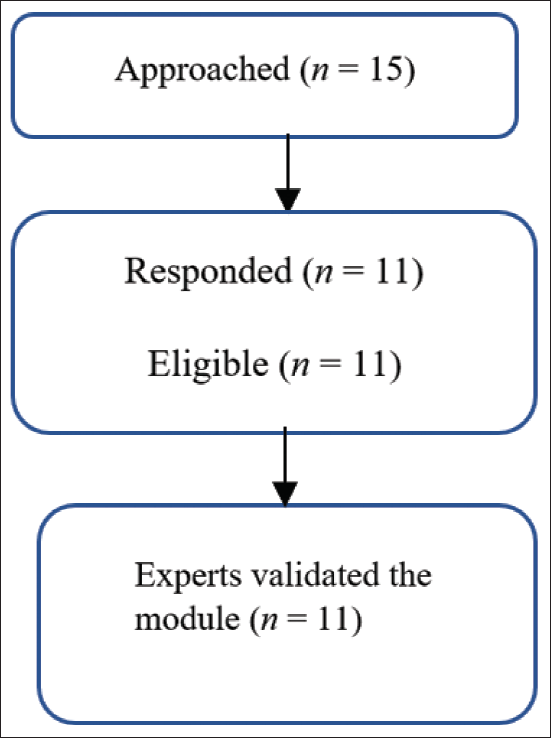
A total of 15 experts were invited to participate in the content validation process. Of these, 11 experts responded, while 4 did not; therefore, content validation was conducted based on responses from 11 experts (Figure 1).
Recruitment of Experts for Validation.
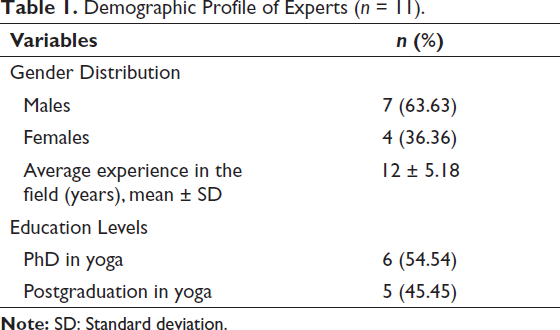
The demographic and professional characteristics of the experts are summarised in Table 1. The panel comprised professionals affiliated with reputed institutions, including Swami Vivekananda Yoga Anusandhana Samsthana (SVYASA), National Institute of Mental Health and Neuro Sciences (NIMHANS), National Institute of Nutrition (NIN), National Institute of Complementary Medicine (NICM) Health Research, Ipcowala Naturopathy and Yoga Center and the Central University of Rajasthan.
Demographic Profile of Experts (n = 11).
For retention of a practice in the final module of each phase, a CVR ≥ 0.59 was applied based on Lawshe’s CVR formula (p < .05, one-tailed for 11 experts). 30 Consequently, 9 of 21 practices in the menstrual phase, 1 of 31 in the follicular phase, 8 of 33 in the ovulatory phase and 9 of 28 in the luteal phase were excluded due to CVR values below the threshold.
Phase III: Feasibility Testing of the Modules
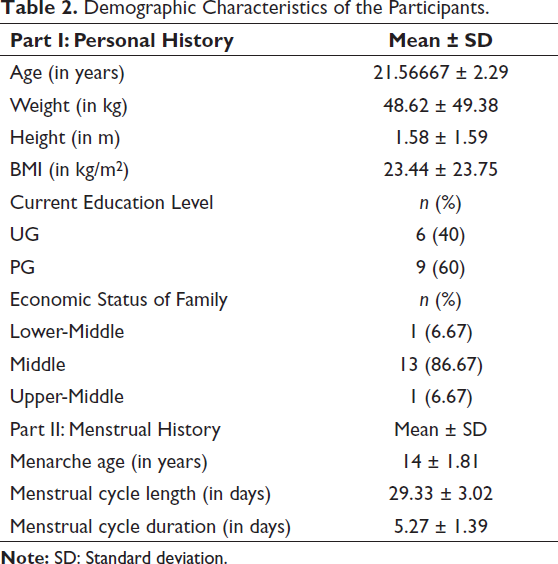
Socio-demographic information was collected in two parts. Part 1 included their personal details, and part 2 comprised their menstrual cycle-related details, including relevant medical history. The overall demographic profile of the participants is presented in Table 2.
Demographic Characteristics of the Participants.
Measurement of Intervention Fidelity
All 15 eligible participants consented to participate, yielding a recruitment rate of 100%. Participants who attended at least 28 sessions were eligible for post-intervention assessments. All participants completed the intervention, resulting in a 100% retention rate and 0% attrition. No adverse events were reported throughout the intervention period.
Measurement of Face Validity
Feedback of Participants on a 3-point Likert Scale
Satisfaction with the intervention – 100%
Intention to continue the intervention in the future – 73.33%
Helpful in managing problems related to each phase of the menstrual cycle – 100%
Helpful in managing PMS symptoms – 93.33%
Helpful in regulating emotions during the luteal phase – 86.67%
Helpful in improving overall mood – 86.67%
Helpful in improving physical strength –86.67%
Helpful in improving flexibility – 93.33%
Helpful in improving balance – 86.67%
Appropriateness of phase-specific adaptation – 80%
In the checklist assessing the perceived usefulness of individual practices in each phase, most practices were rated ‘extremely useful’ or ‘moderately useful’. During the menstrual phase, one participant each rated Swash-kriya and prone postures as ‘not useful,’ and one rated Nadanusandhana as ‘moderately useful’. In the follicular phase, one participant each rated Sukshma Vyayamas and balancing, standing, sitting and prone postures as ‘moderately useful’, while two participants rated supine postures as ‘moderately useful’. During the ovulation phase, one participant each rated the Sukshma Vyayama, Swash-kriya, prone and supine postures as ‘moderately useful’. In the luteal phase, two participants each rated twisting postures and Nadanusandhana as ‘moderately useful’, and one rated supine postures as ‘moderately useful’. All remaining practices were rated as ‘extremely useful’ across phases.
Instructor Evaluation
Instructor-rated Yoga Performance Assessment (YPA) ratings indicated that participants were generally able to perform the practices effectively during the menstrual and luteal phases, except for two to three participants who experienced difficulty with prone and supine postures during these phases. During the follicular and ovulation phases, some participants initially required assistance with Vipareet Karni Mudra and Virbhadrasana III; however, by the end of 8 weeks, they were able to perform these practices independently. Additionally, a small number of participants required additional time to complete each round of Suryanamaskara.
The finally validated yoga module for each phase, along with the YPA scale, has been presented in Tables 3A–3D.
The Final Validated Yoga Module for Menstrual Phase and Yoga Performance Assessment During the Feasibility Study.
The Final Validated Yoga Module for Follicular Phase and Yoga Performance Assessment During the Feasibility Study.
The Final Validated Yoga Module for the Ovulation Phase and Yoga Performance Assessment During the Feasibility Study.
The Final Validated Yoga Module for Luteal Phase and Yoga Performance Assessment During the Feasibility Study.
Outcome Measures
Normality Test
Data for both PMSS and PMS-QoL, including all subscales, followed a normal distribution. Accordingly, pre–post comparisons were conducted using parametric Student’s t-tests.
Changes in Premenstrual Syndrome Scale
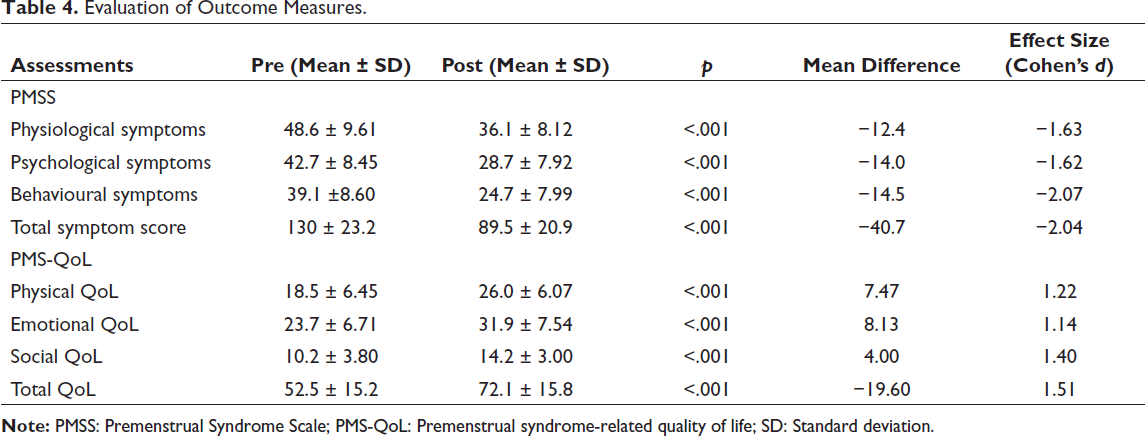
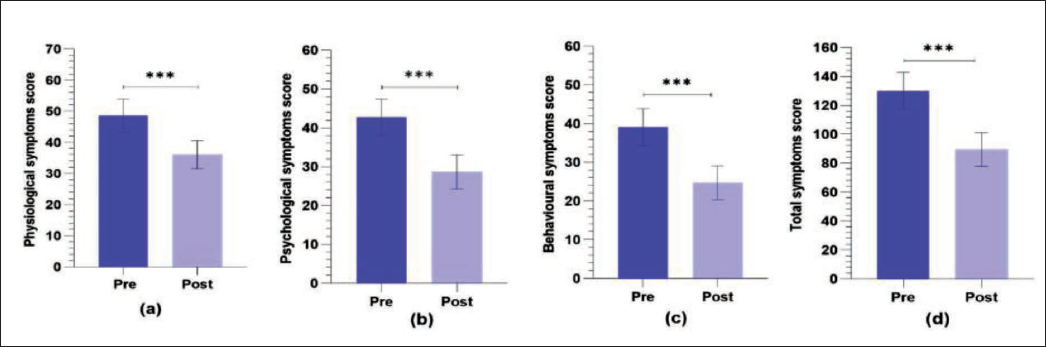
After 8 weeks, significant reductions were observed across all PMSS domains: physiological (p < .001, ∇ = −12.4, d = −1.63), psychological (p < .001, ∇ = −14.0, d = −1.62), behavioural symptoms (p < .001, ∇ = −14.5, d = −2.07) and total scores (p < .001, ∇ = −40.7, d = −2.04). Detailed results are presented in Table 4 and Figure 2.
Evaluation of Outcome Measures.
Changes in Subscales of the Premenstrual Syndrome Scale (PMSS): (a) Physiological Symptoms, (b) Psychological Symptoms, (c) Behavioural Symptoms and (d) Total Symptoms.
Changes in Premenstrual Syndrome-related Quality of Life
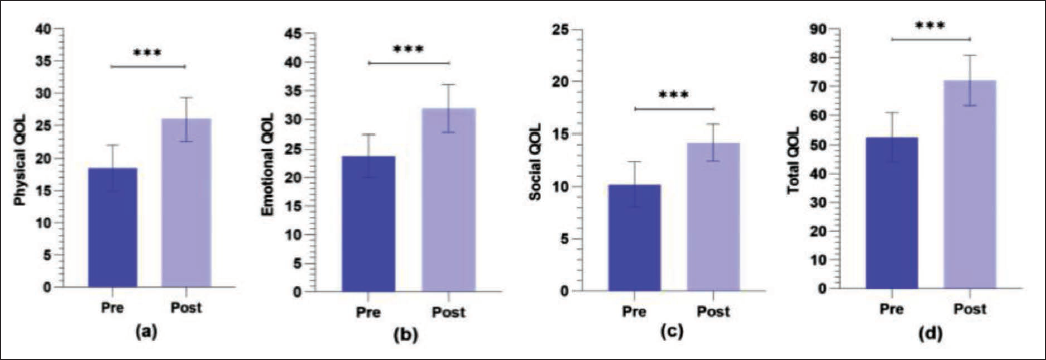
There was significant improvement across all domains of PMS-QoL, including physical (p < .001, ∇ = −7.47, d = −1.22), emotional (p < .001, ∇ = −8.13, d = −1.14), social QoL (p < .001, ∇ = −4.00, d = −1.40) and in overall QoL (p < .001, ∇ = −19.60, d = −1.51). Results are summarised in Table 4 and Figure 3.
Changes in Subscales of the Premenstrual Syndrome-related Quality of Life (PMS-QoL): (a) Physiological QoL, (b) Emotional QoL, (c) Social QoL and (d) Total QoL.
The findings of this study suggest that the module is feasible, safe and with no adverse events for females with PMS. A comprehensive summary of the feasibility outcomes is provided in Supplementary Table 1, following the guidelines adapted from Bowen et al. 32
Discussion
This study presents a comprehensive, menstrual cycle-specific yoga module designed to enhance menstrual health in women. The module is structured into four phases of the menstrual cycle, each comprising practices tailored to address its distinct psychophysiological demands. Eleven qualified experts validated the module, and feasibility was assessed in 15 female university students with PMS. The findings indicate that the module was feasible, safe and associated with no adverse events. It reduced PMS symptoms and improved PMS-QoL. Practice duration varied across phases, requiring approximately 37 min during the menstrual phase, 66 min during the follicular phase, 65 min during the ovulatory phase and 45 min during the luteal phase.
Previously validated yoga modules or protocols for conditions with higher prevalence among females, such as primary dysmenorrhea, hypothyroidism, rheumatoid arthritis and migraine, have largely overlooked the need for modification or customisation of practices for each menstrual cycle. This limitation also applies to yoga protocols designed for healthy female populations. In contrast, the present study introduces a four-phase yoga module that incorporates practices focusing on energy levels, body mobility, functionality, emotional state and hormonal fluctuations across the menstrual cycle. As such, the module may be suitable not only for women with PMS, but also for women with other cycle-related conditions, eumenorrheic females with clinical conditions (with modifications specific to that condition), as well as the healthy female population.
Different menstrual phases are associated with distinct psychophysiological changes.34, 35 During menstruation, the female body adapts to decreasing ovarian steroid hormones, 6 resulting in several perimenstrual symptoms such as fatigue, mood swings and other physical or emotional challenges. 23 Accordingly, the menstrual-phase module emphasised restorative practices, relaxation, chanting and pranayama, with these components accounting for the majority of the 37-min session. During the follicular and peri-ovulatory phases, rising ovarian oestradiol is associated with modulation of central neurotransmitter systems—notably serotonergic and GABAergic pathways and related monoaminergic signalling—which has been linked to increased subjective energy and positive affect.24, 36 In some studies, phase-dependent differences in maximal strength have also been observed, with meta-analytic evidence indicating modest advantages during the late follicular and ovulatory phases for certain strength outcomes. 37 Consequently, the modules for these phases were longer (approximately 65 min) and incorporated a greater proportion of dynamic and strengthening practices, balanced with relaxation. During the ovulatory phase, slightly longer relaxation components were included to facilitate physiological and psychological preparedness for the subsequent luteal phase. The late luteal phase is characterised by regression of the corpus luteum and a consequent decline in oestradiol and progesterone levels, 38 and this hormonal withdrawal is frequently associated with increased sensitivity to hormonal fluctuations, with many women reporting fatigue, reduced perceived energy and motivation and other premenstrual symptoms during this period.24, 28 Therefore, the luteal-phase module was relatively shorter (45 min) and emphasised gentle movements, regulated breathing and relaxation.
This study has several strengths. First, the module was specifically developed for females to accommodate the psychophysiological changes that occur across the menstrual cycle. Second, this module applies to both healthy women and those with regular menstrual cycles who experience menstrual-related disorders. Third, feasibility testing in women with PMS supports its applicability to menstrual disorders. The module’s effectiveness is further demonstrated by the observed improvement in PMS symptoms and QoL, corroborated by participants’ subjective feedback. Additionally, the use of an established YPA scale and the application of Bowen’s feasibility framework further strengthen the methodological rigour of this study.
However, several limitations of this study should be acknowledged. The case vignette method was not employed during content validation. The number of experts involved was relatively limited. The sample size of the pilot feasibility study was small. Future research should aim to replicate and extend this module in larger and more diverse populations, including women with dysmenorrhea, menorrhagia and other menstrual disorders.
Conclusion
This study reports the development, content validation and preliminary feasibility testing of a four-phase, menstrual cycle-specific yoga module that explicitly aligns the type and intensity of practice with phase-related psychophysiological changes. In a pilot sample of female university students with moderate to severe PMS, the module was acceptable and feasible to implement. It was associated with reductions in PMS symptom severity and improvements in PMS-QoL. The demonstrated feasibility of this module in a menstrual disorder, such as PMS, supports its direct application to healthy eumenorrheic populations to promote menstrual health across the cycle. Further feasibility and efficacy studies across other menstrual disorders characterised by regular ovulatory cycles are warranted.
Footnotes
Acknowledgements
The authors gratefully acknowledge Saptaparna Pradhan and Upanita Biswas for their valuable assistance during the data collection period. The authors also extend their sincere appreciation to all the study participants for their enthusiastic involvement, which contributed significantly to the success of this trial. The authors further thank the Department of Yoga for providing the necessary infrastructure and resources essential for the successful execution of this research.
Author’s Contribution
DH: Writing—review and editing, writing—original draft, methodology, software, formal analysis, data curation, visualisation, validation, conceptualisation; AB: Writing—review and editing, writing—original draft, software, formal analysis, visualisation; KM: Writing—review and editing, validation, supervision, methodology, conceptualisation; RB: Writing—review and editing, validation, methodology; SK: Writing—review and editing, software, formal analysis; SSC: Writing—review and editing, formal analysis, visualisation; MM: Writing—review and editing, data curation, methodology, visualisation; PBN: Writing—review and editing, methodology, software; RHM: Writing—review and editing, methodology.
Data Availability
The data set generated during and/or analysed during the current study is available from the corresponding author on request.
Declaration of Competing Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written informed consent was obtained from the participants before their enrolment in the study after providing a detailed explanation of the study procedures
Statement of Ethics
The study was approved by the Institutional Ethical Committee of Central University of Rajasthan (CURAJ/H-IEC/25/03/0012). It was further registered in the Clinical Trial Registry of India (CTRI/2025/04/085497).
Supplementary Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.