
Abstract
Background
Eating attitude can be defined as beliefs, thoughts, feelings, behaviour and relationship with food. It can impact a person’s food choices and health status. A deviant eating attitude is a maladaptive pattern of thoughts and behaviours related to food consumption, which can include periods of inconsistent eating, ranging from overeating to undereating, dietary restriction, emotional eating and preoccupation with food and body weight. These concerns may be visible in the form of emotional dysregulation, anxiety, depression, low self-esteem and interpersonal difficulties. The deviant eating attitude can lead to psychological distress, as individuals may use restrictive eating patterns to cope with overwhelming emotions and life stresses, further deteriorating their overall mental health. Dialectical behaviour therapy (DBT) plays a key role in addressing this vicious cycle by targeting the core emotional and behavioural patterns which maintain disturbed eating disorder. DBT reduces the shame and self-stigma that affect the eating cycle and fosters genuine engagement with the therapeutic process. Through DBT, an individual can learn about mindfulness, distress tolerance, emotion regulation and interpersonal effectiveness. It facilitates individuals to recognise and manage uncomfortable emotions without resorting to dysfunctional eating patterns.
Purpose
The study aimed to explore the therapeutic effect of DBT on deviant eating attitude, along with mental health in adolescents.
Methods
A single case report method was used in the current study. The tools used in the study were case history, Mental Status Examination, Eating Attitudes Test-26, developed by David M. Garner, and Mental Health Inventory, developed by A. K. Srivastava. A total number of 14 sessions of DBT were given, and the pre- and post-therapy assessments were conducted. A case of a 15-year-old female presented with the chief complaints of concerns with her weight and physical looks, high consumption of junk food, disturbed sleep routine, disturbed interpersonal relationship, anger outburst, low self-esteem, irritability and reduced academic performance since the last 2 years, which increased significantly in the last 6 months.
Results
The pre- and post-assessments were conducted, and they indicated relief in the symptoms reported by the client. She reported improved focus and increased motivation for academic goals. She also reported improved social relationships with improved mood and regulated sleep than before. She reported a reduction in the consumption of junk food. Her interpersonal skills improved significantly, allowing her to express her thoughts and feelings more effectively.
Conclusion
Findings support DBT as an effective mode of intervention that targets deviant eating attitudes and improves mental health by strengthening emotion regulation, increasing distress tolerance, and improves interpersonal skills.
Introduction
The food we consume provides us with nutrition and fuels our organs, regulates our moods and sustains the capacity to think, feel and influence our behaviour. The brain and body maintain an intricate system of hunger and satiety signals precisely because adequate nutrition is non-negotiable for survival. 1 Psychologically, food influences our emotions, reward and self-regulation, and mood significantly influences food choices. It is found that people often use eating as a coping mechanism for stress and negative life situations. 2
Eating attitude refers to an individual’s beliefs, thoughts, emotions, behaviours and overall relationship with food. Eating attitudes are described as deeply personal cognitive and affective orientations towards food that directly shape dietary behaviour and, over time, determine nutritional outcomes and overall health status. 3 These attitudes influence food choices, eating patterns and ultimately health status. Eating attitude can also be conceptualised as a regular, selective and repetitive pattern of food consumption, encompassing the quantity and type of food consumed, the context in which eating occurs, and the social setting or companionship during meals.
A deviant eating attitude is a maladaptive pattern of thoughts and behaviours related to food consumption, which can include limited to episodes of overeating or undereating, dietary restriction, emotional eating and preoccupation with food and body weight. 4 They are health-compromising eating patterns which impact the health and well-being of a person. It may include eating behaviours such as overeating, unbalanced diet, skipping meals, restricted or specific diet consumption, consumption of sugar-sweetened beverages and excessive consumption of processed food. It can result in obesity and increased body fat, decreased energy level, poor attention and concentration, risk of cardiac conditions, diabetes, hypertension and so on. 5 During adolescence, there is an urge to have a higher sense of independence, which might result in the development of unhealthy eating habits that can continue throughout adulthood. 6
Mental health plays a vital role in shaping eating attitudes, with psychological factors like emotional dysregulation, depression, anxiety, low self-esteem and impulsivity, 7 strongly predicting unhealthy patterns such as restrained eating, emotional eating and binge tendencies. 4 Individuals with serious mental illness often experience disrupted hunger cues and use food as a coping mechanism for stress, leading to mindless or excessive eating that accentuates weight gain and leads to psychological distress. 8
Dialectical behaviour therapy (DBT) is an evidence-based intervention widely used for eating disorder problems, particularly those involving emotional dysregulation, binge eating, purging or restrictive patterns and treatment of borderline personality disorder.9, 10 DBT perceives disturbed eating not from a moral or cognitive failure but as a skills deficit in the context of emotional dysregulation. DBT perceives these behaviours as predictable consequences of unhealthy coping skills and reduced capacity to tolerate and regulate overwhelming emotional experiences. 11
DBT targets the core mechanisms driving these issues, such as intense emotions, impulsivity and poor distress tolerance, through four skill modules: mindfulness (observing urges without acting), distress tolerance (surviving cravings without bingeing/restricting), emotion regulation (managing triggers like shame or anxiety) and interpersonal effectiveness (navigating relationships that exacerbate symptoms).10, 11
Methods
In the current article, a single case report method is adopted. A detailed case history, mental status examination and baseline assessment were conducted with the client. A total of 14 therapy sessions of DBT were conducted. After completion of sessions, post-assessments were conducted.
The Case
The case presented was of Ms R, a 15-year-old female, studying in class XI in a private school in Lucknow, belonging to a middle socio-economic status. She lives in a nuclear family setup with her father, mother and younger brother. She was presented with chief complaints of concern about her weight and physical looks, high consumption of junk food, disturbed sleep routine, disturbed interpersonal relationship, anger outburst, low self-esteem, irritability and reduced academic performance since the last 2 years, which increased significantly in the last 6 months.
The client reported that she had a breakup in the year 2023, which significantly impacted her mental health. She has been trying to cope with it, but has been having difficulties dealing with it. Her partner was critical, and he would often comment on her physical appearance and would compare her with his other peers. She would feel insecure about her physical appearance due to it. She could not confront him and would feel stuck in the relationship, due to which she would often get angry during conversations. He broke the relationship abruptly, which made her feel that she was inadequate. She has been feeling that she is not enough, due to which she is single, and her boyfriend broke the relationship. The breakup affected her self-esteem and confidence drastically. She started feeling insecure about herself after the breakup, and her sleep and appetite were disturbed post the breakup.
She would eat her food at irregular timings and most of the time she ordered food from outside and did not prefer eating the food cooked at home. She reported eating at midnight while studying and consuming caffeine to stay awake. She reported that she feels bloated and has constipation whenever she eats junk food constantly. She prefers to eat in the canteen at school and does not eat her tiffin; she often shares this with her peers. This makes her mother upset and leads to arguments with her mother very often. This makes her upset and irritated most of the time, due to which she avoids having any conversation with her parents. Whenever she is at home, she prefers to stay in her room and watch movie reels or is on OTT.
She reported having frequent misunderstandings and fights with her peers. She has been having difficulty adjusting to her classroom. Most of her friends have stopped talking to her after the breakup due to miscommunication. She further added feeling lonely at school, due to which on most of the days she does not feel like going to school. She pushes herself to be regular to maintain her attendance. She has not been able to score as per her potential; in the recent half-yearly exam, she just managed to score the passing marks.
The client appeared well-kempt and tidy, an adequate level of self-hygiene was maintained, eye contact was maintained with the examiner and rapport was established with ease. The attitude towards the examiner was cooperative, no abnormality in the motor behaviour was found, speech was relevant, coherent and goal-directed with no abnormality. No abnormality in the cognitive functions was reported. Affect was irritable, communicable and appropriate. In thought content, ideas of guilt were present; no abnormality was detected in perception. Judgement was intact, with Grade Level 2 insight.
Test Administered
Eating Attitudes Test
This test was conducted to assess eating disorder risk.
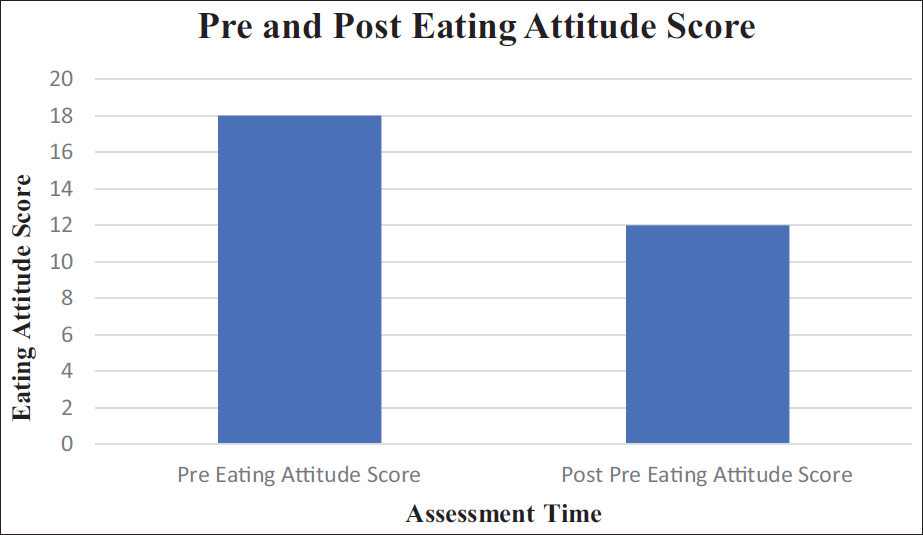
Total Eating Attitudes Test-26 (EAT-26) score: 18.
The scores obtained indicated that there is a high risk of development of an eating disorder.
Mental Health Inventory
This test was conducted to assess mental health.
Total score on Mental Health Inventory (MHI): 144.
The scores obtained on the scale indicated poor mental health.
Target Areas for Therapy
Reduce quality-of-life interfering behaviour.
Build skills for emotional and behavioural regulation.
Create acceptance by validating the client’s experience.
Aim to change unhealthy behaviours.
Help the client build healthy coping skills.
Rationale of the Therapy
The client reported a deviant eating attitude, along with difficulties in interpersonal functioning and a gradual decline in academic performance. She experiences challenges in social situations, including difficulty expressing her needs, heightened sensitivity to other opinions, struggles in establishing and sustaining relationships, and limits in her ability to handle conflicts efficiently. These difficulties not only impact her everyday functioning but also largely impact her unhealthy eating behaviours. DBT is used to address both the disturbed eating attitude and the underlying mental health concerns.
Structure of the Intervention
Each DBT session lasted around 45–50 min and followed a planned structure to ensure effective therapeutic work. The session usually began with a discussion about the client’s recent experiences, emotional state and any concerns faced since the previous session. After this, the client and therapist jointly decided the agenda and focus areas for the session. Pre- and post-assessments were done to assess the effectiveness of the DBT techniques. At the end of the session, the important points were reviewed, progress was discussed and suitable practice tasks or coping strategies and homework were planned for the week.
Initial Phase (Sessions 1–4)
In this phase of therapy, the focus was on building the therapeutic alliance, informed consent was taken and pre-assessment was conducted. Psychoeducation was given to the client about the symptoms and mode of therapy. Based on the case history and symptoms, a case formulation was made by using the biosocial model. Commitment strategies, diary card introduction and core mindfulness skills (Wise Mind, What/How skills) were introduced in this phase.
The initial phase of therapy focused on establishing the therapeutic alliance, informed consent was taken and pre-assessment was conducted. The therapist emphasised building a strong therapeutic alliance, as a collaborative and trusting relationship between the therapist and client is considered essential to the success of DBT-based interventions. 9 Informed consent was obtained prior to the commencement of any therapeutic procedures, ensuring the client’s autonomy and ethical participation throughout the treatment process.
Middle Phase (Sessions 5–12)
The second phase of therapy focused on the treatment component, which focused on systematic skill learning and behavioural intervention. The focus was on learning core DBT skills: mindfulness, distress tolerance, emotion regulation and interpersonal effectiveness. This phase was focused on facilitating the client’s coping strategy to improve the deviant eating attitude and emotional regulation skills. The skills taught to the client during this phase were TIPP, ACCEPTS, Radical Acceptance, IMPROVE, PLEASE, DEAR MAN, GIVE and FAST.
Termination Phase (Sessions 13–14)
The primary focus of this phase involved developing a relapse prevention plan, formulating a crisis management strategy and preparing coping cards for continued self-regulation. A post-assessment was subsequently administered, and the pre- and post-intervention scores were reviewed and compared. The process concluded with a formal discussion regarding the termination of therapy, marking the planned closure of the intervention.
Results
The post-assessment was conducted after the completion of all 14 DBT sessions.
In EAT-26, her score was 12, which suggests a low risk of developing an eating disorder (Figure 1).
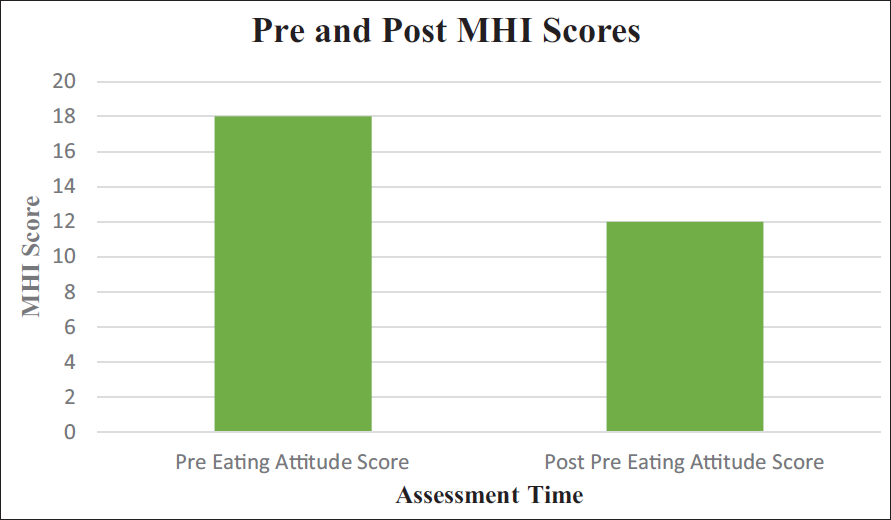
In the MHI, the score was 115, suggesting improved mental health (Figure 2).
The post-assessment scores changed on both tests after application of DBT. The change in the scores indicates DBT is an efficient therapy for the management of mental health and deviant eating attitude.
Ms R showed significant changes in different areas of her everyday functioning. She reported that her focus towards her studies has improved, and her motivation to go to school has also increased. There has been improved motivation towards her academic goals. This has helped in improving her academic performance and has contributed positively to her self-confidence.
She reported about her better engagement in school and active participation in extracurricular activities, which reflects improved well-being and engagement in life. This would eventually help in increasing her sense of achievement and a balanced routine, all of which would contribute to her personal development.
She reported a change in her interpersonal communication and has started having healthier connections with her peers and parents. This has reduced past misunderstandings and internal emotional build-up. Her eating habits have improved, as she has been eating all her meals, and her junk food consumption has reduced significantly. This has helped in improving her communication with her parents and has reduced conflicts significantly. Alongside this, her tolerance towards stress has improved significantly, which is indicative of better emotional regulation and coping skills, helping her navigate challenges more efficiently without feeling overwhelmed.
Overall, these improvements are indicative of positive development in her eating attitude, psychological health and improved social functioning.
Graph Showing the Pre-intervention and Post-intervention Scores on the Eating Attitudes Test-26.
Graph Showing the Pre-intervention and Post-intervention Scores on the Mental Health Inventory (MHI).
Discussion
Eating attitudes mostly indicate a comprehensive pattern of distress about food and its related behaviour. In the current case, DBT facilitated reframing eating attitude as a stress-related behaviour. Through skills building in DBT, the client learned different techniques to manage emotions and learned positive coping skills, which further contributed to improved mental health.12, 13 The client learned ways to manage distress tolerance, which further helped her improve her interpersonal skills. The frequency of consumption of junk food and irregular timing improved, which eventually helped her manage health-related symptoms. DBT intervention also focused on validation and Wise Mind techniques, which eased feelings of not liking food specifically.9, 14
The present case report presents an efficient application of DBT in the management of deviant eating attitudes and mental health. The findings support the efficiency of DBT as an effective intervention. The visible improvements in interpersonal skills, sleep patterns, coping skills and changed eating patterns provide evidence to support that maladaptive eating patterns are caused and maintained not only by cognitive distortions but can also be influenced by ineffective skills. The skills learned from DBT can be helpful in creating effective and long-term changes in behaviour. 15
The findings also suggest that emotional dysregulation, in combination with environmental factors, can play a significant role in fostering eating attitudes; they can also affect mental health.2, 16 The short and specific structure of DBT increases its clinical benefit, and research implies that DBT-based interventions can lead to enhancement in emotional health and behavioural management. 17
In the current case, a remarkable change in eating attitudes and coping skills led to improvement in the overall emotional health. In the termination session, she reflected on her sleep, saying, ‘I tried breathing and grounding… It actually helped. I am now able to fall asleep faster now’.
When discussing appetite, she shared, ‘I’m eating more regularly now, I carry tiffin regularly and even finish that. It feels normal again’.
It has also helped the client to enhance her interpersonal communication, which has eventually led to marked improvement in overall mental health. Mindfulness skills learned through DBT help in enhancing emotional regulation and further help in improving overall well-being. 18 DBT helps in significantly reducing binge eating patterns by enhancing distress tolerance and emotional awareness, which helps individuals to rely less on food and its related behaviour as a significant coping skill.11, 16, 19
Conclusion
The present case contributes to the evolving clinical literature, which suggests that DBT is an effective mode of intervention for the treatment of deviant eating attitude and further fosters positive improvement in mental health. DBT is a skills-based intervention that helps in the management of emotion dysregulation and interpersonal difficulties.9, 10 Emotional dysregulation is identified as one of the common coping skills in eating disorders. Difficulty in processing emotions can reinforce individuals to develop unhealthy coping skills such as limited eating, overeating or undereating as a form of effective regulation. 20
In conclusion, DBT core skills, mindfulness, distress tolerance, emotion regulation and interpersonal effectiveness precisely address emotional complexities, which further lead to emotional unpredictability and dysfunctional coping skills. With time, DBT has been used as an effective mode of treatment for eating disorders, particularly for binge eating disorder, bulimia nervosa. 14
Footnotes
Authors’ Contribution
All authors contributed to the study’s conception and design. Research conceptualisation, data sorting, analysis and duplication checks were performed by DR. NS assisted in the final reading of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written informed consent was obtained from the client to participate in the study. The client was briefed about their voluntary participation and confidentiality of her responses.
Statement of Ethics
Ethical approval was obtained from the Ethics Committee of Amity University, Lucknow, Uttar Pradesh, India.