
Abstract
Background
Hypertension is a major global health concern associated with substantial morbidity and mortality. Lifestyle interventions, including yoga-based stress management, are increasingly recognized as complementary approaches for blood pressure control..
Purpose
To evaluate the effectiveness of a 12-week structured yogic breathing and relaxation programme compared with standard non-pharmacological care in adults with hypertension.
Methods
In this randomized controlled trial at AIIMS Rishikesh, 66 adults with Stage 1 hypertension or elevated blood pressure were randomized to either a yoga intervention or standard care. The intervention group practised a validated 40-minute daily yoga module comprising pranayama and relaxation techniques. Primary outcomes were changes in systolic and diastolic blood pressure, while secondary outcomes included BMI, waist-to-hip ratio, sleep quality, perceived stress, and alcohol use.
Results
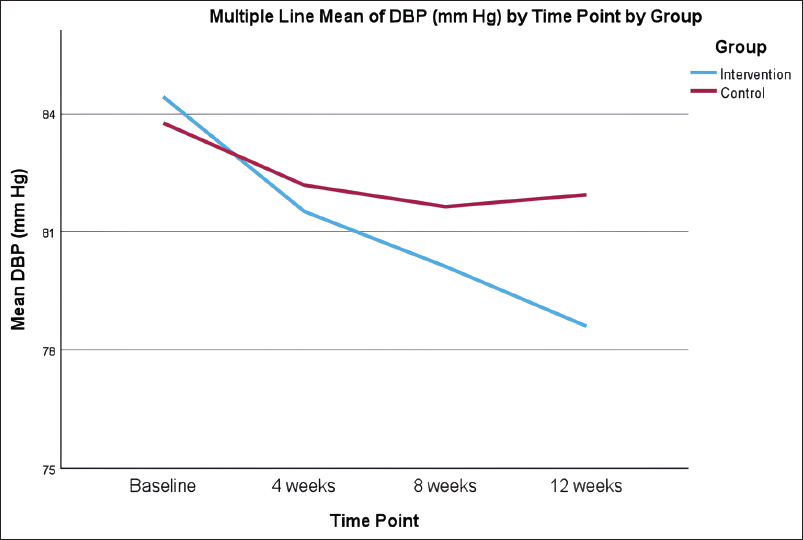
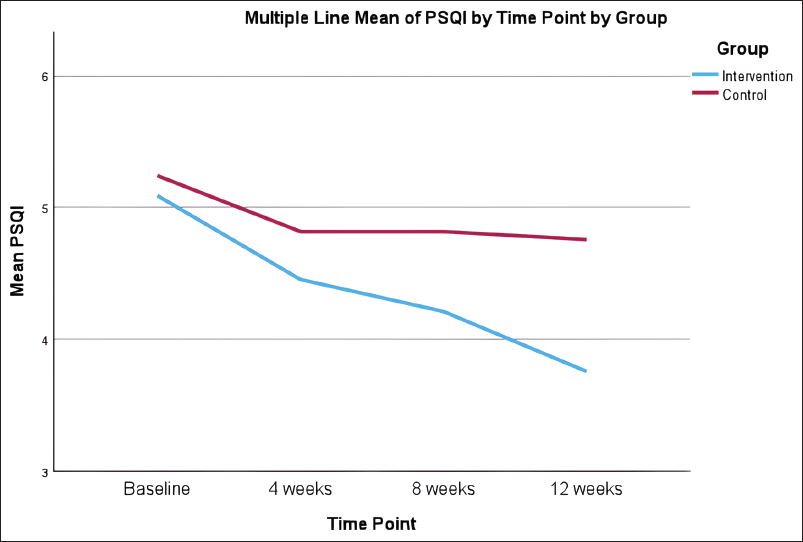
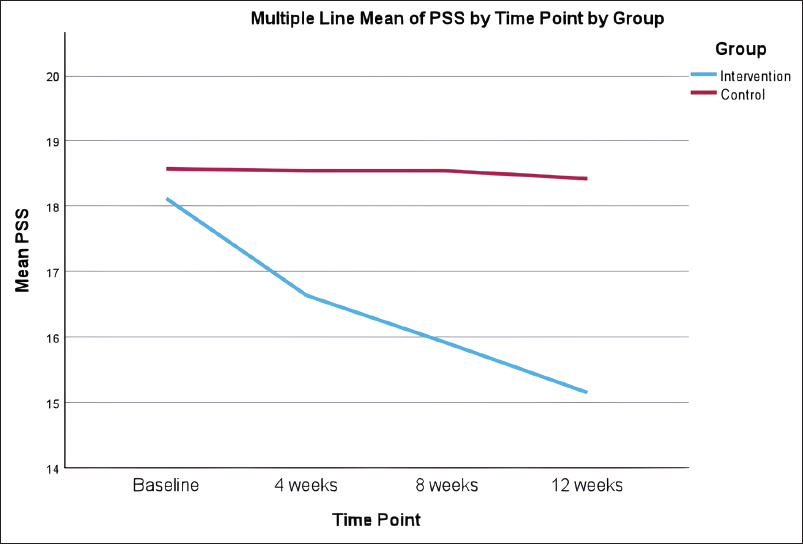
After 12 weeks, the yoga group showed significant reductions in systolic (132.42 ± 3.96 to 124.06 ±4.11 mmHg; p <0.001) and diastolic blood pressure (84.42± 2.82 to 78.61 ± 3.89 mmHg; p <0.01), with significant improvements in perceived stress (p=0.001) and sleep quality (p = 0.019). BMI and waist-to-hip ratio showed clinically relevant but non-significant improvements.
Conclusion
A 12-week yogic breathing and relaxation programme effectively reduced blood pressure and improved lifestyle parameters, supporting its integration into hypertension management. Further long-term studies are warranted.
Keywords
Introduction
Hypertension is a significant global public health issue, contributing significantly to premature mortality and increased risk of cardiovascular diseases (CVD), stroke and kidney disorders.1, 2 The prevalence of hypertension has doubled over the past three decades.3, 4 India faces a substantial hypertension disease burden with a prevalence of 22.6%, affecting 24.1% of men and 21.2% of women. 2 The condition also significantly contributes to India’s share of the global burden, with 18% of hypertension-related Disability-Adjusted Life Years occurring in India.5, 6
While medications are widely used to manage hypertension, lifestyle modifications are now being recommended as an equal first-line approach to counter the effects of some of the modifiable risk factors for hypertension and help to better control disease progression. 7 Use of alternative stress-reduction techniques such as yoga, tai-chi, mindfulness, music and progressive muscle relaxation has also increased lately to counter stress and its effects regarding hypertension. 8 Yoga, an ancient mind-body practice, integrates controlled breathing (pranayama) and relaxation techniques that influence autonomic function and stress responses. 9 Several studies suggest that yoga positively impacts blood pressure by enhancing parasympathetic activity, improving vascular compliance and reducing cortisol levels. 9
Despite growing evidence, yogic breathing and relaxation techniques have not been fully integrated into routine hypertension management. 8 The present study was designed to evaluate the effects of a structured pranayama and relaxation-based intervention in participants with hypertension in comparison with standard non-pharmacological management for blood pressure reduction. We hypothesised that a structured 12-week yogic breathing and relaxation programme would demonstrate beneficial effects on blood pressure and associated lifestyle parameters, including perceived stress and sleep quality, among hypertensive adults when compared with standard non-pharmacological interventions.
Methods
Study Design and Participants
A randomised controlled trial (RCT) was conducted at AIIMS Rishikesh’s General Medicine outpatient department (OPD) and Lifestyle Disease Clinic between February 2024 and October 2024, after getting approval from the Institutional Ethics Committee, AIIMS, Rishikesh (Reference number: AIIMS/IEC/23/387; Dated: 06/10/2023), and after registration in Clinical Trial Registry India (CTRI number—CTRI/2024/02/063355). The study recruited 66 participants aged 18–55 years with Stage 1 hypertension or elevated blood pressure, as classified by AHA guidelines. 7
Participant recruitment was done using a simple consecutive sampling method at the General Medicine OPD, AIIMS, Rishikesh. Inclusion criteria were: participants aged 18–55 years, diagnosed with elevated BP and Stage 1 hypertension (as per AHA/ACC guidelines), 7 and participants willing to participate in the study procedures, comply with intervention protocols and adhere to follow-up assessments after randomisation.
The exclusion criteria for this study include individuals who have been practising yoga or meditation for more than 1 month in the previous 6 months. Additionally, individuals with comorbidities such as diabetes mellitus, chronic kidney disease (CKD), established cardiovascular disease, stroke, epilepsy, migraine or any psychiatric disorder were excluded. Participants unwilling to provide written informed consent were excluded. Pregnant women were not eligible to participate, and those with less than 75% compliance with the study protocol were also excluded.
Eligible participants were allocated to two arms (ratio 1:1) with the help of a computer-generated randomised sequence. The random allocation sequence was generated by a third person with no clinical involvement, ensuring an unpredictable allocation sequence. Treatment allocation was concealed using sequentially numbered opaque sealed envelopes to prevent selection bias. Envelopes were opened sequentially and only after writing the participant’s name and other details in order to remove any chances of selection bias. The patient’s history was taken, a physical examination was conducted, and findings were recorded on standardised case record forms. Blood pressure and anthropometric measures were taken. Alcohol consumption was assessed using the Alcohol Use Disorders Identification Test (AUDIT). 10 Sleep quality was evaluated using the Pittsburgh Sleep Quality Index (PSQI). 11 Perceived stress levels were assessed using the Perceived Stress Scale (PSS). 12
At the time of recruitment, participants were informed that they could be allocated to either the yoga intervention arm or the control arm following randomisation, and informed consent was obtained for participation in the trial irrespective of group allocation. Participant willingness to participate did not influence group allocation, which was performed independently using a computer-generated random sequence. As recommended for behavioural and non-pharmacological intervention trials, 13 participant willingness to comply with assigned interventions was considered necessary to facilitate adherence and reduce attrition; however, allocation remained fully randomised throughout the study.
Intervention
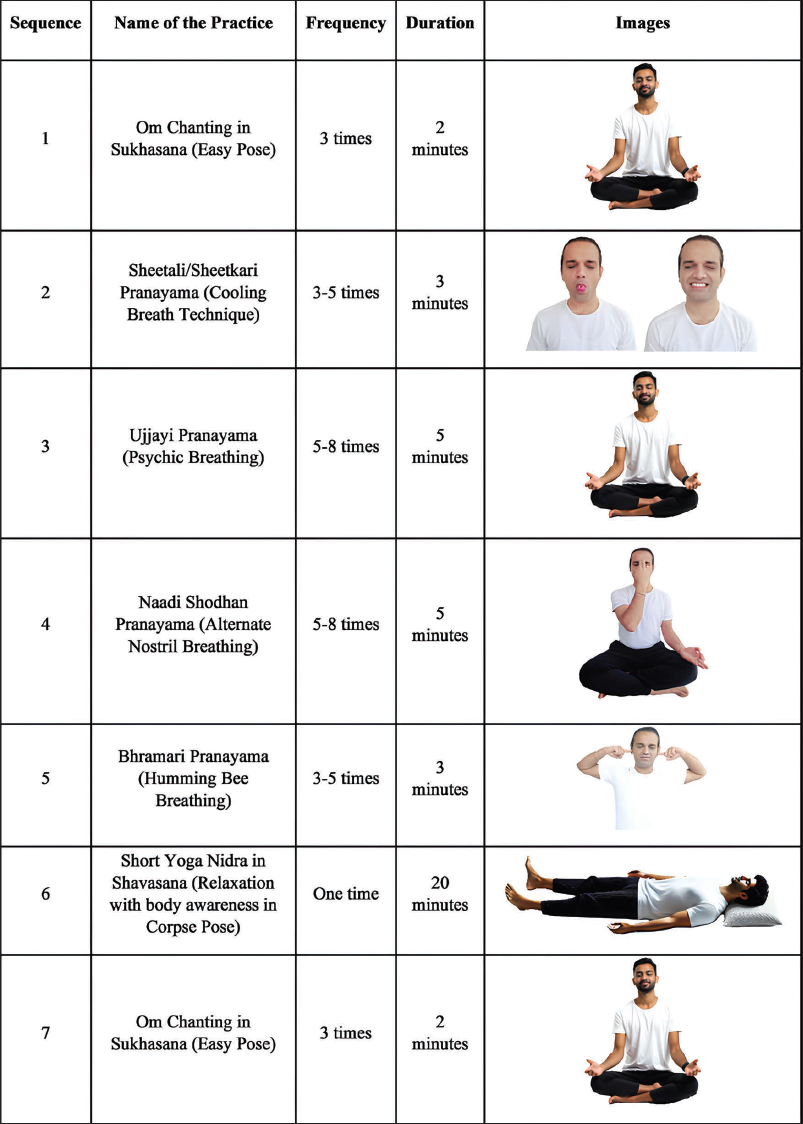
The intervention group practised a validated 40-min daily yoga module incorporating pranayama and relaxation techniques. Participants were initially trained in person during their first clinical visit by a qualified yoga therapist and were provided with handouts containing the sequence of practices along with supportive images for home reference (Figure 1). Since the intervention primarily involved simple breath-based practices and relaxation techniques without any complex physical postures (asana), audio-guided instructions were considered adequate following supervised training. Compliance and intervention fidelity were monitored using a dedicated mobile application developed in collaboration with the Indian Institute of Technology Jodhpur, which provided standardised audio instructions for daily home practice. Additionally, the audio-based format was considered more feasible for participants from remote areas with limited internet accessibility. The control group received standard non-pharmacological recommendations, including brisk walking, the DASH diet and lifestyle modifications.
Yoga Intervention Module for Hypertension (Participant Handout).
Validation of Yoga Intervention Module for Hypertension.
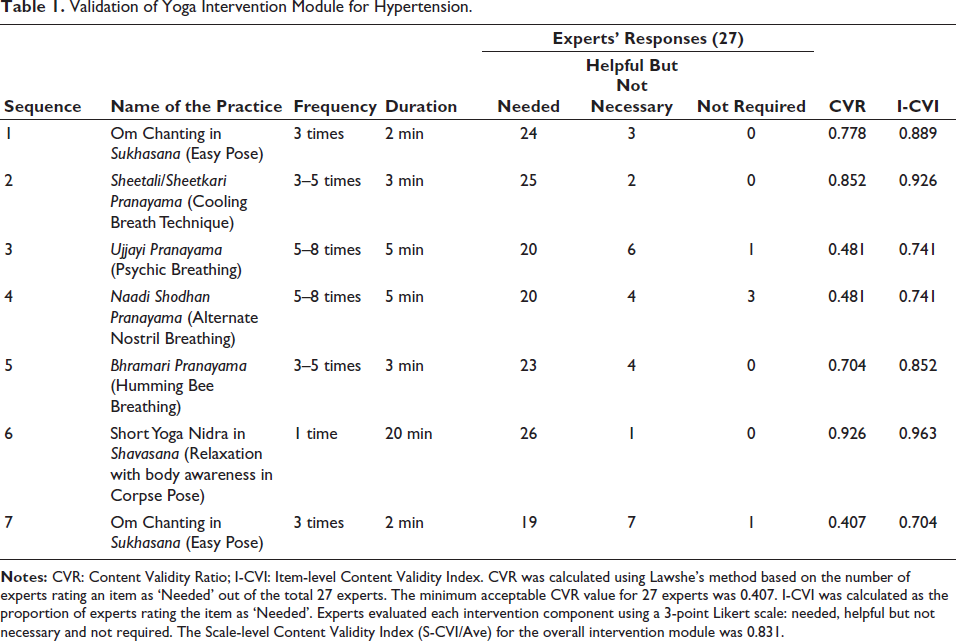
The yoga intervention module for hypertensive patients utilised in the current study underwent a systematic content validation process to establish its therapeutic relevance and scientific appropriateness. A total of 27 experts with professional experience of 5–13 years in yoga therapy participated in the validation process. Experts belonging to various schools and traditions of yoga were approached to ensure balanced expert consensus. The selected yogic practices were included in the intervention based on their safety, feasibility and ease of practice for hypertensive patients, in accordance with contemporary yoga therapy textbooks and protocols developed by reputed yoga institutions such as the Bihar School of Yoga, Kaivalyadhama, S-VYASA, Morarji Desai National Institute of Yoga and the Central Council for Research in Yoga and Naturopathy.
The experts evaluated each intervention component using a 3-point Likert scale consisting of ‘Needed’, ‘Helpful but not Necessary’ and ‘Not Required’. Content Validity Ratio (CVR) was calculated using Lawshe’s method, 14 with the minimum acceptable CVR for 27 experts considered as 0.407. 15 The obtained CVR values ranged from 0.407 to 0.926, indicating acceptable to excellent expert agreement regarding the necessity of the selected Yogic practices. Guided yoga nidra demonstrated the highest CVR (0.926), followed by Naadi Shodhan Pranayama (0.852). The Item-level Content Validity Index (I-CVI) values ranged from 0.704 to 0.963, while the Scale-level Content Validity Index based on the averaging method (S-CVI/Ave) was 0.831, indicating good overall content validity of the intervention module (Table 1). Furthermore, this intervention has also been previously utilised in a published RCT, 16 thereby further supporting its feasibility, clinical applicability and therapeutic relevance in hypertensive populations.
Outcome Measures and Assessment Procedures
Primary outcomes included changes in systolic blood pressure (SBP) and diastolic blood pressure (DBP). Secondary outcomes assessed body mass index (BMI), waist-to-hip ratio (WHR), sleep quality (PSQI), stress levels (PSS), alcohol consumption (AUDIT) and 24-h dietary intake.
All baseline assessments were conducted at the General Medicine OPD and Lifestyle Disease Clinic, AIIMS Rishikesh, before randomisation. Follow-up assessments were subsequently performed at 4 weeks, 8 weeks and 12 weeks after enrolment during scheduled participant visits to the same clinical setting.
Blood pressure measurements were recorded using standardised clinical procedures after adequate seated rest in a calm environment. Anthropometric measurements, including height, weight, waist circumference and hip circumference, were obtained using standard measuring instruments following institutional protocols. Questionnaire-based assessments, including AUDIT, PSQI and PSS, were administered in a structured manner through direct participant interaction.
All clinical and questionnaire-based assessments were conducted by the Principal Investigator after protocol-specific training under faculty supervision. Anthropometric measurements, blood pressure recordings and questionnaire administration were performed during scheduled study visits using standardised procedures and instruments, with periodic monitoring by faculty supervisors to ensure protocol adherence and data quality. The OPD/clinic-based yoga intervention sessions were conducted separately by a qualified yoga therapist who was not involved in outcome assessments.
Statistical Analysis
It was determined that a sample size of 52 participants would provide enough power (0.80) to detect a significant difference in the primary outcome measures with a two-tailed α of 0.05. Adding a 20% attrition rate makes the total number of participants required for the study to be 66. Hence, the total sample size was N = 66, with 33 participants in each arm (control and experimental). Sample size calculations are based on the effect size estimated from a previous study done by Murugesan et al. 17
Data were collected in MS Excel 2024. SPSS 30.0 version for Windows was used for data analysis. All data were readily accessible to the principal investigator, the guide and the co-guides of the research study. Categorical variables were presented as numbers and percentages (%). Continuous variables were presented as mean ± standard deviation (SD). For descriptive statistics: the normality of data was assessed by the Shapiro–Wilk test. The data were then represented as mean and SD, followed by the application of parametric and non-parametric tests based on the normality results of the data. For inferential statistics of data with normal distribution: independent t-test was used to compare the two groups at each time point during follow-up. Repeated measures of analysis of variance (ANOVA) were used to explore the changes over time within the same group. The two-way repeated measures of ANOVA method were used to explore differences between the two groups over time. A p value < .05 was considered statistically significant. Intention-to-treat analysis was followed for data analysis. Missing data were managed as the Last Observation Carried Forward. The information gathered from the patient was kept confidential, and the patient’s identity remained undisclosed.
Results
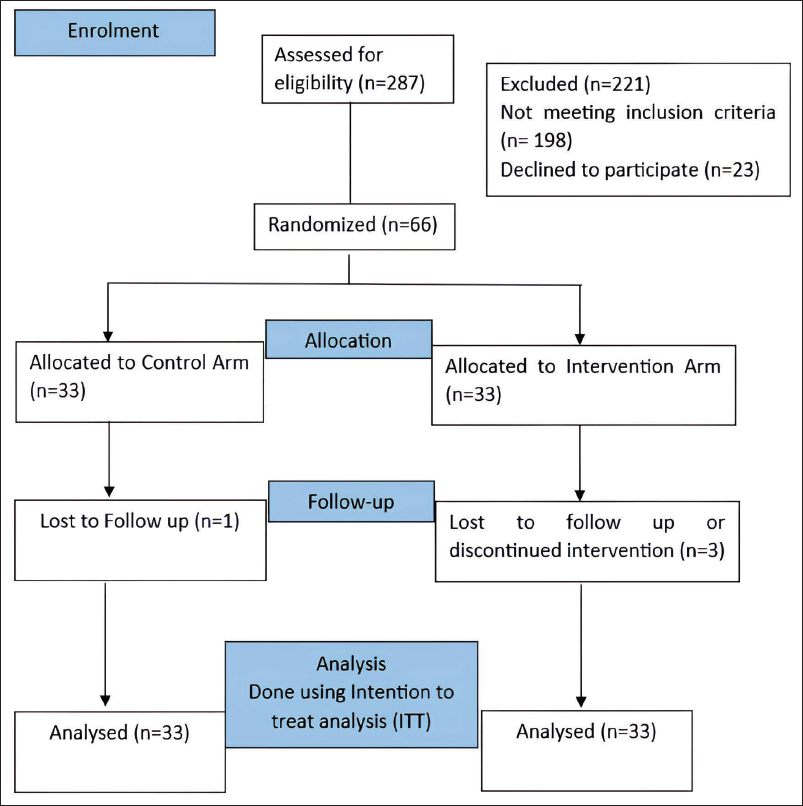
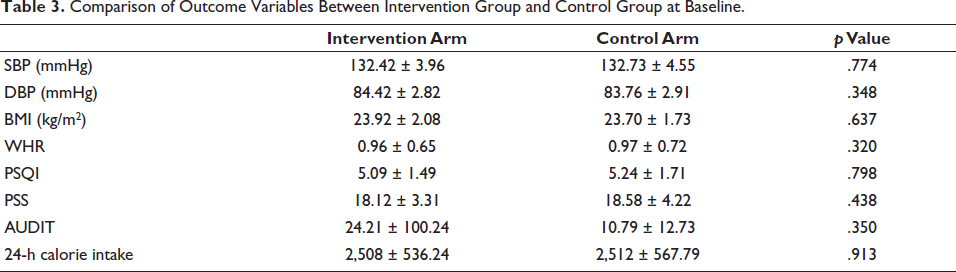
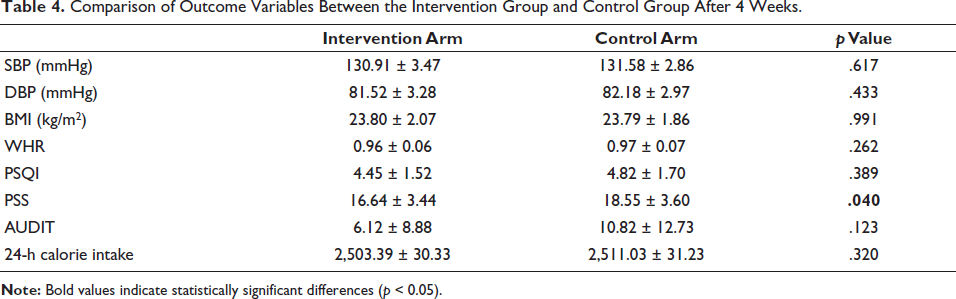
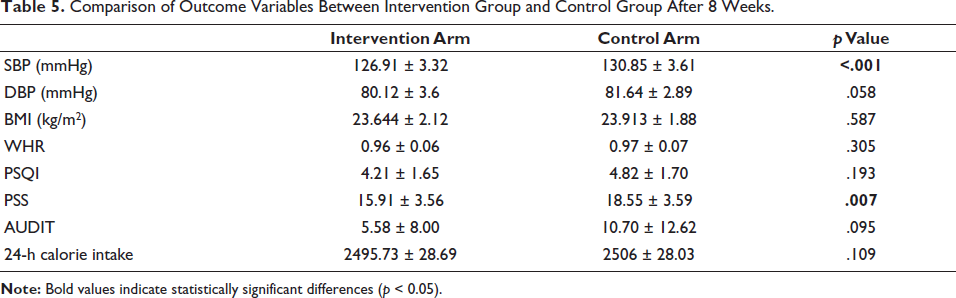
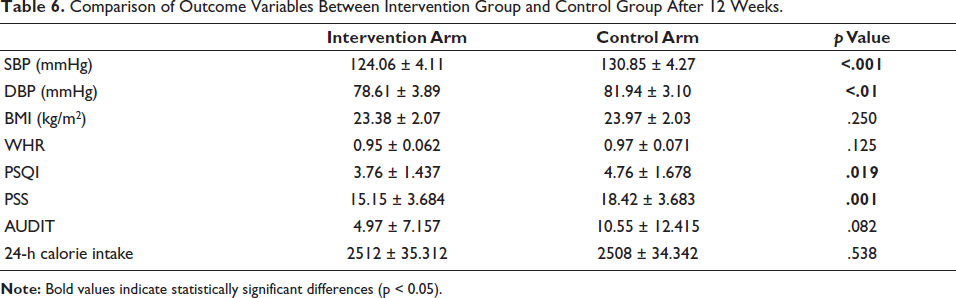
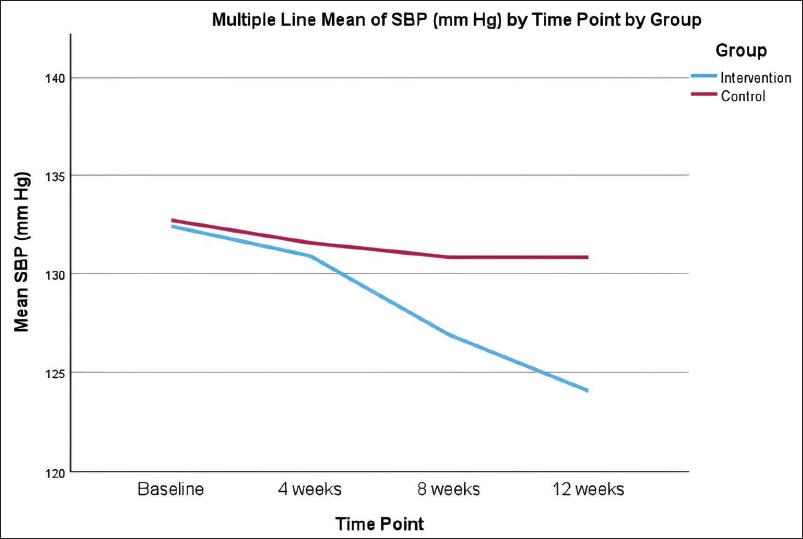
Of the 287 assessed for eligibility, 66 participants were randomised into two arms (control and intervention arm) (Figure 2). The mean age of the study population in both groups was quite similar, and sex distribution was also quite similar in both of the study populations (Table 2). Outcome variables were similar at baseline (Table 3). Comparison of outcome Variables between intervention and control groups after 4, 8 and 12 weeks is summarised in Tables 4–6, respectively. Changes in SBP, DBP, PSQI and PSS over time are shown in line diagrams depicted in Figures 3–6, respectively. The intervention group showed a significant reduction in SBP (p < .001) and DBP (p < .01) over 12 weeks compared to the control group. Stress levels (PSS) significantly decreased in the intervention group (p = .001). Sleep quality (PSQI) improved significantly (p = .019). No statistically significant changes were observed in BMI and WHR, though a downward trend was noted.
Study Flow Chart.
Comparison of Age and Sex Between Intervention and Control Arm.

Comparison of Outcome Variables Between Intervention Group and Control Group at Baseline.
Comparison of Outcome Variables Between the Intervention Group and Control Group After 4 Weeks.
Comparison of Outcome Variables Between Intervention Group and Control Group After 8 Weeks.
Comparison of Outcome Variables Between Intervention Group and Control Group After 12 Weeks.
Change in Systolic Blood Pressure Over Time.
Change in Diastolic Blood Pressure Over Time.
Change in Pittsburgh Sleep Quality Index Over Time.
Change in Perceived Stress Scale Over Time.
Discussion
Hypertension, one of the most widespread health challenges globally, stands as a leading risk factor for a host of serious conditions, including CVD, CKD and stroke.3, 7 These associated complications contribute substantially to morbidity and mortality worldwide, emphasising the need for effective management strategies. This RCT was conducted to evaluate the effectiveness of yogic breathing and relaxation techniques in managing hypertension and associated lifestyle factors. These practices, rooted in Indian traditional holistic health paradigms, have been suggested to offer a cost-effective and accessible means of improving health outcomes, particularly in resource-limited settings.
The study revealed a significant reduction in both systolic and diastolic blood pressure among participants in the intervention group over 12 weeks. Specifically, mean SBP decreased from 132.42 ± 3.96 mmHg to 124.06 ± 4.11 mmHg (p < .001), showing a 6.31% reduction in SBP after 12 weeks. Mean DBP dropped from 84.42 ± 2.82 mmHg to 78.61 ± 3.89 mmHg (p < .01), showing a 6.88% reduction in DBP after 12 weeks. For instance, earlier studies have highlighted yoga’s role in managing hypertension, and a meta-analysis conducted by Cramer et al. corroborates these results, reporting an average reduction of approximately 10 mmHg in SBP and 5 mmHg in DBP among individuals practising yoga. 18 However, our study had a different set of easily doable exercises for the Indian context.
Various physiologic mechanisms are hypothesised for this reduction of BP. Pranayama and relaxation techniques enhance parasympathetic activity, reducing heart rate, vascular resistance and improving cardiac output, thereby lowering blood pressure. This modulation is well-documented in previous studies.18–20
Controlled breathing and pranayama stimulate nitric oxide production, promoting vasodilation, reducing arterial stiffness and enhancing vascular compliance. These effects improve blood flow and lower blood pressure. Research also links regular yoga practice to decreased arterial stiffness, benefiting overall cardiovascular health.21–23 The findings are particularly relevant in India, where hypertension control rates remain low and medication use carries social stigma. Only about 33.2% of hypertensive patients achieve adequate blood pressure control, leaving many at risk of complications such as cardiovascular disease, stroke and CKD. 24
Stress is a key modifiable risk factor for hypertension, influencing its onset and progression. This study showed a significant reduction in PSS scores in the intervention group, dropping from 18.12 ± 3.31 to 15.15 ± 3.684 (p < .01), after 12 weeks. These findings align with existing research on the stress-relieving benefits of yoga-based practices.21, 25
Chronic stress activates the HPA axis, raising cortisol levels and blood pressure. Yoga practices such as pranayama and yoga nidra stimulate the vagus nerve, enhance parasympathetic activity and reduce cortisol, restoring balance and lowering blood pressure, reducing hypertension-related risks.26, 27 These findings echo those of Chiesa and Serretti, who reported ‘significant stress reduction through mindfulness-based stress reduction BSR) practices, including yoga’. 28
The significant drop in PSS scores underscores yoga’s role as a holistic, non-pharmacological approach to stress-induced hypertension. By addressing both physiological and psychological health, yoga enhances emotional stability, complements traditional therapies and improves hypertension outcomes. Integrating it into public health initiatives could boost control rates, reduce disease burden and enhance quality of life.
Sleep disturbances, closely linked to hypertension, were significantly improved in the intervention group, as reflected in reduced PSQI scores (5.09–3.76). Poor sleep quality increases sympathetic activity, blood pressure variability and cardiovascular risks. Yoga, particularly yoga nidra and pranayama, enhances restorative sleep by regulating circadian rhythms, reducing nocturnal sympathetic activity and lowering cortisol levels.29, 30
By addressing sleep disturbances, yoga supports blood pressure control and overall well-being. Its integration into hypertension care offers a cost-effective, holistic solution for improving sleep, reducing stress and stabilising blood pressure.
Although BMI and WHR ratio reductions were modest, the data were not statistically significant, but these changes are clinically relevant. Stress-induced alterations in appetite regulation and metabolic function often exacerbate obesity-related hypertension.31, 32 The observed reduction in WHR (from 0.96 to 0.95) indicates decreased central obesity, a critical predictor of cardiovascular risk. Additionally, yoga enhances metabolic health by improving insulin sensitivity and lipid profiles. 33 Future studies with longer time periods are required for these parameters.
The intervention group outperformed the control group, which followed standard non-pharmacological recommendations such as the DASH diet and brisk walking. 7 While lifestyle modifications are effective, yoga offers unique advantages by addressing both physiological and psychological determinants of hypertension. A comparative study by Tyagi and Cohen highlighted yoga’s superiority over conventional exercise in reducing stress and improving cardiovascular parameters. 34
India’s hypertension burden, marked by early onset and poor control rates, calls for culturally relevant solutions. Rooted in tradition, yoga offers a feasible, low-cost intervention aligned with healthcare priorities. This study found significant reductions in systolic (6.31%, p < .001) and diastolic blood pressure (6.88%, p < .01) in the intervention group, along with lower stress and improved sleep quality, enhancing mental and emotional well-being. While BMI and WHR changes were modest, they reinforced the role of lifestyle interventions in holistic health management.
Limitations
Although participants received supervised in-person training and supportive demonstration materials, the intervention utilised audio-guided instructions rather than audiovisual guidance during home practice, which may have further enhanced standardisation and participant engagement.
Conclusion
This study demonstrated the effectiveness of a 12-week yogic breathing and relaxation programme in improving blood pressure, stress and sleep quality in hypertensive adults. The intervention group showed significant improvements compared to controls, highlighting yoga’s multidimensional benefits in managing both physical and mental health aspects of hypertension.
The findings support integrating yoga into hypertension care, particularly in resource-limited settings. However, further research with larger, more diverse populations and extended follow-up is needed to confirm long-term sustainability.
Footnotes
Acknowledgements
The authors sincerely thank all participants and contributors for their time and commitment to this 12-week randomized trial. We also acknowledge the app developers from the Indian Institute of Technology Jodhpur for developing the mobile application used to deliver standardized audio instructions and monitor home practice compliance. We are especially grateful to Gurudev Sri Sri Ravi Shankar Ji and the Sri Sri Publications Trust for permitting the use of the Yoga Nidra Hindi Audio as part of the intervention.
Authors’ Contributions
Conceptualization / Design: Rajat Sharma, Monika Pathania, Ravi Kant Data Curation / Investigation: Rajat Sharma, Praag Bhardwaj, Sumit Kalra Data Analysis: Rajat Sharma, Monika Pathania, Drupad Das Original Draft Preparation: Rajat Sharma Review & Editing: Monika Pathania, Ravi Kant, Praag Bhardwaj, Sumit Kalra, Drupad Das Supervision: Ravi Kant, Monika Pathania
Declaration of Competing Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written informed consent was obtained from all participants prior to enrolment in the study in accordance with the Declaration of Helsinki. Participants were informed about the objectives, procedures, potential benefits, and risks of the study, and confidentiality of their data was maintained throughout the research.
Statement of Ethics
The study was conducted after approval from the Institutional Ethics Committee, AIIMS, Rishikesh (Reference number: AIIMS/IEC/23/387; Dated: 06/10/2023), and after registration in Clinical Trial Registry India (CTRI number—CTRI/2024/02/063355).