
Abstract
Background
Parkinson’s disease (PD) is a neurological degenerative condition affecting motor and non-motor functions of everyday life. While early management focuses on functional mobility and rehabilitation, evidence supports that yogic interventions as adjuvant therapy are applied yet limited in clinical practice. This study developed a customised yoga therapy module (CYTM) for motor and non-motor conditions, particularly for people with mild to moderate PD.
Purpose
To develop a patient-friendly, symptom-specific, 24-week CYTM for people living with early Parkinsonism of Hoehn and Yahr staging scale I–III.
Methods
The study follows a five-phased methodological development, which comprises a literature search, conceptualisation and development of a 24-week CYTM for early PD, evaluation with validation by the subject/panel experts, and relevance, along with a phase-wise operational method. The relevance of selected practices was validated with the item-level content validity index (I-CVI) and scale-level (S)-CVI/AVR/UA.
Results
The executed five-phased methodological framework, and the newly developed CYTM comprises 29 practices to improve the functional changes of people with early PD. Experts’ ratings yielded I-CVI (>0.91), scale-level content validity index of the average (S-CVI/AVR) (>0.995) with average and scale-level content validity index based on universal agreement (S-CVI/UA) (Universal Agreement) >0.941.
Conclusion
As per the expert’s opinion, the newly developed, symptom-specific, participant-friendly CYTM could be an appropriate practice for people living with mild to moderate PD. This CYTM will be evaluated by a non-randomised controlled clinical trial to establish its effectiveness.
Introduction
Parkinson’s disease (PD) is a neurological degenerative condition most commonly defined by motor symptoms, including resting tremor, muscular rigidity, bradykinesia and postural instability. 1 It also encompasses a wide spectrum of non-motor symptoms such as quality of life, cognitive and executive dysfunction, attentional deficits, sleep disturbances and autonomic dysregulation2, 3 affecting the daily activities of older adults. 4 Recent epidemiological data from 2021 estimate that approximately 11.77 million individuals globally are affected by PD, warning a continued rise in prevalence from 2022 to 2035. 5 At this rate, India may contribute to the largest proportion of the global PD burden, with motor symptom onset, between the age group of 22 and 49 years, who are classified as early-onset Parkinson’s disease (EOPD). 6 The general burden of multiple motor and non-motor manifestations can lead to social stigma, self-withdrawal, reduced activities of daily living (ADL) and psychological distress with markedly diminished quality of life (QoL). 7 Though modern medicine has a limitation to respond, many non-pharmacological treatments play a vital role as adjuvant therapy, 8 and one among them is yoga, the ancient Indian traditional and cultural practice, known to be a lifestyle polypill. 9 Evidence suggests that structured yogic interventions, combined with lifestyle modifications, may mitigate PD-associated symptoms, thereby enhancing the overall functional well-being of the geriatric population. 10
Yoga for Early Parkinsonism in Response to Sustainable Development Goals
Sustainable Development Goals (SDGs) present an action plan structure for promoting holistic health among the PD population. 11 SDGs 3.4 and 3.8 support motor and non-motor conditions, enhancing the quality of life. 12 SDG 4.7 facilitates patient and caregiver education in sustainable self-care, while SDG 10.2 promotes low-cost, comprehensive care for elderly individuals in low- and middle-income countries (LMICs). 13 SDG 11.7 encourages the creation of community spaces for active ageing and yoga practice, and SDG 12.8 advocates sustainable health practices.9, 14 In this context, complementary and alternative therapeutic modalities, particularly yogic interventions, are increasingly recognised as valuable adjuncts in PD management. 12 Early integration of asana, pranayama, meditation and other mind-body practices has been shown to mitigate symptom progression and enhance functional outcomes. 15
Need for a Customised Yoga Therapy Module
Existing research demonstrates that yoga enhances postural control, the overall quality and functionality of life in individuals with PD, 16 and interrelated domains influence environmental factors, and lifestyle behaviours.17, 18 Emerging evidence further supports that yoga’s role in improving neuromuscular flexibility, mobility and global functional capacity in PD management.19, 20 However, limitations like short duration, styles and approaches, instructor competency, trial design, tele-yoga delivery and sample size 21 demand a need to develop a culturally aligned, customised practice, particularly for older adults residing in residential care homes.22, 23 The study focuses on developing a customised yoga therapy module (CYTM) to treat both motor and non-motor signs in a clinical setting for early PD, classified as mild to moderate according to the Hoehn and Yahr scale I–III. 24
Methods
The development of a yoga therapy module involves a search of existing literature with an integration of yoga-based interventions in a structured therapeutic framework, with the objective of achieving targeted clinical outcomes. 25 The research team undertook a planning process to design the module to be symptom-specific and participant-friendly. Accordingly, the CYTM was developed using classical yogic texts alongside contemporary empirical evidence, emphasising interventions in modulating PD-related dysfunctions. The development of this existing module for early PD adheres to the 21-item CLARIFY (checklist standardising the reporting of intervention of yoga) checklist 26 given in Supplementary File 1.
Various yogic practices comprising loosening techniques (warm-ups), breathing exercises (pranayama), yoga postures (asana), meditation techniques (dhyana) and yoga-based relaxation (yoga nidra) were systematically selected from classical yoga texts, including Patanjali Yoga Sutra, Hathapradipika, Gheranda Samhita and Hatha Ratnavali, along with modern literature of Yoga Dharshna and Light on Yoga. The module development was executed in a five-phased methodological framework, focusing on creating a comprehensive practical tool for early PD, as shown in Figure 1.

Phase 1: Search Strategy for the Literature Review
Eligibility Criteria
The study encompasses randomised controlled trials, clinical trials and experimental studies involving participants aged 60 years and above, diagnosed with PD Hoehn and Yahr stages I–III, from 2015 to 2025 July. Eligible studies must focus on yoga-therapy-based interventions, including mind–body therapy, mindfulness practices, relaxation techniques, breathing exercises and asanas with yoga protocol and development.
Search Strategy
The initial review prioritised older adults with early PD (Hoehn and Yahr I–III) and randomised controlled trials (RCTs)/clinical trials in PubMed and Cochrane Central to match the intended CYTM. The search strategy was developed in PubMed and Cochrane Central. The following Boolean operators are used to search the existing literature, peer-reviewed articles in the PubMed database. The search terms were (‘Yoga’[Mesh] OR ‘Mind-Body Therapies’[Mesh] OR ‘Yoga/therapeutic use’[Mesh] OR ‘Yoga/methods’[Mesh]) AND (‘Parkinson Disease’[Mesh] OR ‘Parkinsonian Disorders’[Mesh]) AND (‘Program Development’[Mesh] OR module OR protocol OR ‘program development’ OR tailored OR selective OR specific OR ‘patient-centered’ OR ‘disease-specific’ OR validation OR ‘content validity’). The same was also carried out in Cochrane Central: Line 1 (Yoga/Mind-body therapies): (‘yoga’ OR ‘mind-body’ OR ‘mind body’ OR ‘mind-body therapy’ OR ‘mind body therapy’). Line 2 (Parkinson’s Disease): (‘parkinson disease’ OR ‘parkinson’s disease’ OR parkinsonian OR parkinsonism OR ‘parkinsonian disorders’). Line 3 (Tailored/Protocol/Program development): (tailored OR protocol OR ‘program development’ OR ‘programme development’ OR ‘patient-centered’ OR ‘patient centred’ OR ‘disease-specific’) and Line 4 combined: #1 AND #2 AND #3. Data were manually reviewed and screened for both the search log and other literature that we came across. Existing work referring to key findings, methodologies, outcomes and critical analysis to identify strengths and gaps in previous research was a first step. Special focus was given to the study outcomes, stages of PD involved, type and duration of yogic methods, incorporating appropriate safety measures, careful designing and methods by which validations were carried. While it is acknowledged that yoga has the potential to alleviate various PD symptoms and boost quality of life, 28 specific therapeutic mechanisms and their extent remain underexplored in scientific literature. Contemporary yogic literature increasingly highlights the health-promoting effects of structured yogic interventions. 29
Phase 2: Conceptualisation and Development of the Proposed Yoga Practice
Conceptualisation
The research team comprised experienced yoga experts and clinical researchers, in collaboration with a qualified medical professional specialised in geriatric care and PD patients. The entire research team together discussed motor and non-motor symptoms of PD. This multidisciplinary dialogue helped in contextualising the clinical manifestation. The development process includes: review of literature, understanding the PD criteria and attention to stakeholders’ opinions specific to the conditions of PD. All medical practitioners, geriatric specialists, pathologists, yoga professors, PD patients, caregivers and alternative health specialists had given their suggestions on the signs and symptoms affecting the routine life of PD people.
Development
The characteristics and symptoms of clinical observations are studied through literature. It explains: balance depends on vestibular, proprioceptive and visual integration and dysfunction increases fall risk. 30 Muscle strength and circulation are interrelated, requiring intact neuromuscular function, sometimes resulting from slowed transit, incontinence and cognitive dysfunction. 31 For each specific case of mentioned PD, therapeutic practices were identified from classical and modern yogic texts. 32 However, the non-motor challenge practices initially demand careful adaptation and progression. Formulating a CYTM specific to the PD symptoms, the module integrated mobilisation techniques like warm-ups aimed at mitigating articular rigidity and enhancing mobility. Standing āsanas were included to promote postural balance and to strengthen hip extensors, quadriceps, hamstrings and calf muscles. 33 Relaxation techniques, pranayama practices including yogic meditation and guided yoga nidra were included to attenuate psychological manifestations commonly connected with PD, like anxiety, stress and depression. 34 These methods were intended to foster neuropsychological stability and promote a calm, integrated state of body and mind.
Phase 3: Evaluation and Validation by the Subject and Panel Experts
The evaluation of the proposed yoga module for individuals with early PD was done in a systemic, multi-stage validation.25, 35 The CYTM was formulated based on the critical parameters of mode, frequency, session duration and progressive therapeutic stages in the framework of standardised therapeutic prescriptions. In order to achieve cognitive diversity and independent judgement, we have used purposive sampling to identify a panel of five experts in the field, including the traditional yoga scholars, interdisciplinary yogic science researchers and experienced practitioners of complementary medicine with advanced academic qualifications, clinical experience (at least 2 years, usually 5+) and multidisciplinary expertise. 36 The completed module, with the justifications of each practice for the targeted PD symptoms, was sent to the experts electronically. The review of each expert was done individually, with a thorough consideration of therapeutic relevance, scientific rigour, safety and clinical applicability to early-stage PD. 25 The functional capacity of the participants, the adequacy of the number and sequence of practices and compatibility with various stages of early PD were taken care of with special attention to focus on neuromuscular facilitation, motor coordination and autonomic control. 37
Validating the Relevance of Selected Practices
The developed CYTM incorporates 29 distinct yoga practices, which were thoroughly reviewed and discussed in terms of their intended purpose and therapeutic application with face validation. The multidisciplinary panel comprising 40 experts, including PD patients, caregivers, geriatricians, doctoral advisory boards, ethical review committee specialists, scientific review board personnel, certified yoga therapists, statisticians, biomedical researchers, bioethicists, risk assessment professionals, legal experts, lay representatives and social scientists, critically appraised and assessed.
Phase 4: Relevance of the Customised Yoga Therapy Module
After the panel validation, the relevance of the practice was once again validated with a linear scale by the interdisciplinary expert team. The qualified yoga therapy specialists and researchers, along with the clinicians from integrative medicine possessing more than 5–10 years of relevant clinical and research experience, were invited via email to complete a structured survey questionnaire administered through Google Forms. The questionnaire was well explained, and we have asked them to rate the relevance of each of the selected yoga practices on a four-point linear scale ([1] as not relevant, [2] as somewhat relevant, [3] as quite relevant, and [4] as highly relevant) for the relevance level of the content validity index of Lynn. 38 The questions were based on the relevance, clarity, simplicity, comprehensibility and the overall suitability for each practice of asana, pranayama, meditation and relaxation was determined with item-level content validity index (I-CVI) and scale-level content validity index of the average (S-CVI/AVR) >0.80–0.90 which is common and scale-level content validity index based on universal agreement (S-CVI/UA), and this is the universal agreement I-CVI = 1.00. Some more questions are added to get their insightful suggestions regarding the identical methods and their application.
Phase 5: Formulation of Phase-wise Operational Practice
Creation of phase-wise operational practice was formulated to ensure dedicated safety evolution for this intervention to ensure participant-friendly and comprehensible practice with chair support, wall support and graduated introduction when necessary. The implementation of operational practice developed for the intervention delineates a methodical administration framework structured through a four-phase progression model. This model is specifically designed to enable the gradual application of therapeutic practices, allowing adequate temporal intervals for participants’ acclimatisation and physiological adaptation. A four-phase progression ensures systematic delivery while accommodating individual variability. The overall developed CYTM phase-wise operational practice is represented in Supplementary File 2. This developed module will be administered through offline mode for a better therapeutic efficacy, comprising a 1-h session–5 days a week over a 24-week intervention period. Preferably, all sessions will be conducted under the supervision of a highly qualified yoga therapist, ensuring therapeutic appropriateness and safety.
Results
Databases were searched from 2015 to 2025, such as PubMed and Cochrane Central. Among 85 identified articles screened by title and abstract, 70 articles were excluded. Fifteen articles were selected for full-text screening; seven were excluded due to incorrect study duration, incorrect study outcome and finally eight articles of Colgrove et al., 12 Ni et al., 39 Kakde et al., 40 Cheung et al., 13 Kwok et al., 41 Walter et al., 18 Adams et al. 42 and Some et al. 19 were helpful in developing the new CYTM. The search results are explained in Supplementary File 3. The design and testing of the yoga module went through the first round of evaluation with feedback and proposals given by subject experts. According to the recommendations of experts, a few changes were made, such as: starting the session with warm-ups, removing four asanas, increasing breath counts (from three to five) and increasing relaxation duration for lasting benefits. The experts gave verbal and written approval with face validation of therapeutic applicability. A panel of 40 experts carried out a rigorous discussion and evaluation of the clinical advantages. This was followed by 11 subject experts of clinical practice for relevance validation. The questions were based on the relevance, clarity, simplicity, comprehensibility and overall suitability, calculated with (I-CVI) ≥0.91 and (S-CVI/AVR) (Average) ≥0.995 and (S-CVI/UA) (Universal Agreement) ≥0.941, (16 out of 17 items had 100% expert agreement) as excellent scores to determine the relevance and applicability of the selected yoga practices in motor and non-motor functions. The executed five-phased methodological framework yielded a 29-practice CYTM for early PD; item- and scale-level content validity metrics are reported in Tables 1 and 2.
Proportion of Experts Rating Each Item as Relevant.
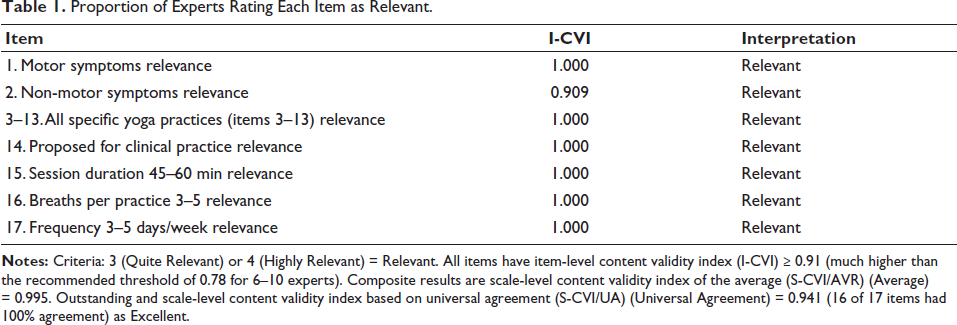
Notes: Criteria: 3 (Quite Relevant) or 4 (Highly Relevant) = Relevant. All items have item-level content validity index (I-CVI) ≥ 0.91 (much higher than the recommended threshold of 0.78 for 6–10 experts). Composite results are scale-level content validity index of the average (S-CVI/AVR) (Average) = 0.995. Outstanding and scale-level content validity index based on universal agreement (S-CVI/UA) (Universal Agreement) = 0.941 (16 of 17 items had 100% agreement) as Excellent.
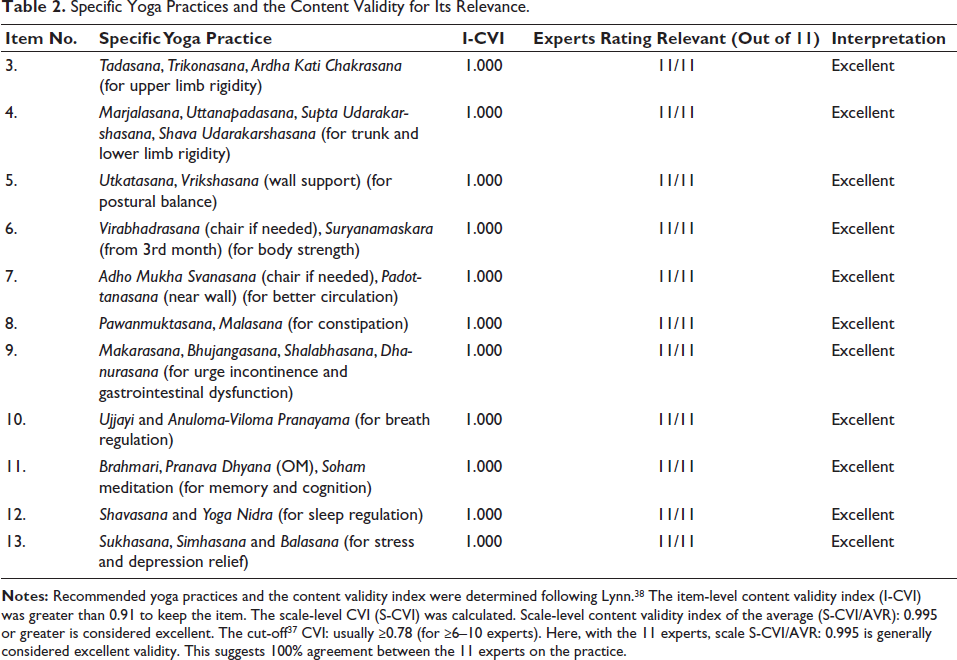
Specific Yoga Practices and the Content Validity for Its Relevance.
Discussion
The module development was executed in a five-phased methodological framework, yielding a preliminary, expert content-validated module for early PD, and a phase progression ensures systematic delivery while accommodating individual variability. Through the literature search, the research team found an existing literature gap and affirmed the necessity to create a CYTM. The validation and relevance results are in line with the previous studies 19 that demonstrated regular yogic sessions have the potential to increase motor proficiency among individuals who are affected by PD through the provision of improved joint mobility and flexibility. 42 Often, practical constraints on the frequency of activities highlight the frequent logistical issues with tele-yoga among the geriatric population and access to online practice.21, 43 In the present study, the yoga regimens for mild and moderate PD were developed based on the existing textbooks and scientific material.25, 44 They are symptom-targeted and participant-specific and were subjected to appropriate statistical tests. Like most other yoga protocols, the module also integrates asanas (poses), pranayama (breathing exercises), meditation and relaxation. 17 As experts suggested, the module will be administered through offline mode for a better therapeutic efficacy, comprising a 1-h session 5 days a week over a 24-week intervention period.
Rigour and Precision of Consensus
The number of people chosen (1–4) for each item, the percentage agreement for ‘relevant’ (3–4), a more stringent ‘4-only’ agreement and 95% binomial CIs for I-CVI are provided. The bootstrap CIs for S-CVI/AVR and S-CVI/UA, and sensitivity by subgroups (e.g., yoga therapists vs clinicians) are also given. The deidentified matrix and analysis outputs are given in the Supplementary File 4.
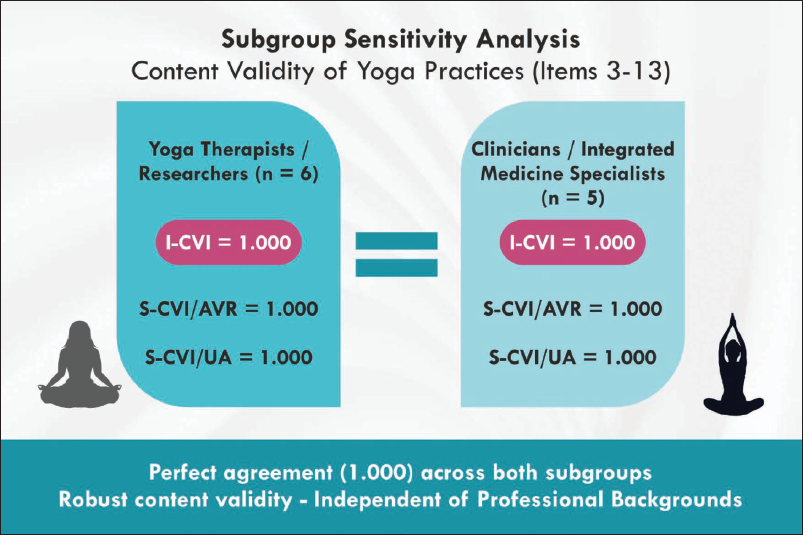
Sub-group Analysis
This showed a perfect content validity (I-CVI = 1.000, S-CVI/AVR = 1.000, S-CVI/UA = 1.000) in both yoga therapists/researchers/PD caregiver cum yoga therapist (n = 6) and clinicians/integrated-medicine specialists of BNYS/BAMS, MD (n = 5) for all 11 yoga practices portrayed in Figure 2.
Conclusion
The expert’s opinion-based CYTM is a symptom-specific and participant-friendly first step to the development of an approved daily practice for people with mild to moderate PD. The 29-practice module will be tested on its feasibility with end-users and then evaluated in a non-randomised controlled clinical trial.
Footnotes
Acknowledgements
The authors thank Yenepoya (Deemed to be University), Mangaluru, Karnataka, India. Sincere thanks to the entire department of Geriatric Medicine, Yenepoya Medical College Hospital, Mangaluru. The authors acknowledge and appreciate the support extended by all subject experts for their role in evaluating and validating the yoga module: Dr Subramanya Pailoor, Department of Yoga Studies, CUK; Dr Govardhan Reddy, Division of Yoga, Center for Integrative Medicine Research, Manipal; Dr Rashmitha, Department of Yogic Science and Spirituality, Uttarakhand; Dr Ajitesh, Department of Yoga, Mangalore University College; and Dr Guru Deo, MDNIY, New Delhi. Special thanks to subject experts of clinical practice for validating the relevance of the module. Gratitude is extended to all the panel experts and the Doctoral Advisory Committee members for their meticulous evaluation and constructive recommendations.
Authors’ Contribution
Study design, methodology and conceptualisation: LM, PA and UK. Developing the original text, collecting data and processing: LM. Interpreting data and analysing, editing and revising the paper: PA and UK.
Clinical Trial Registry of India
The Clinical Trial Registry of India (CTRI) registration: CTRI/2025/07/090595.
Data Availability
The relevance of the chosen practices and their validation are shared along with the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
The authors have not included any identifiable individual data or images in this manuscript. This will be addressed in the future.
Statement of Ethics
This study complies with ethical guidelines set by the Indian Council of Medical Research (ICMR) in 2017 and the World Medical Association Declaration of Helsinki (WMA DoH, 2024 Revision), along with the European Medicines Agency Guideline for Good Clinical Practice. The therapeutic developmental model is part of the doctoral research, approved by the Doctoral Advisory Committee (DAC). Institutional Scientific Review Board (SRB) permitted this study with protocol ID: 52112023 for the geriatric concerns, protocol ID: YNYSCH/SRB/RP/01/2023 for the yogic science concerns. The institutional ethical approval is given by (YEC-2), Protocol Number: YEC2/2024/130.
Supplementary Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.