
Abstract
Introduction:
Attention-Deficit Hyperactivity Disorder (ADHD) is a prevalent neurodevelopmental condition characterized by enduring patterns of inattention, impulsivity, and hyperactivity, with considerable variability in cognitive and developmental outcomes across individuals1. This study compared the cognitive profiles of children with ADHD and typically developing children (TDC) using the Wechsler Intelligence Scale for Children–Fourth Edition (WISC-IV).
Materials and Methods:
Fifty-one children (26 with ADHD, 25 TDC; age range 7–13 years 11 months) were assessed on domains such as Verbal Comprehension, Perceptual Reasoning, Working Memory and Processing Speed. Non-parametric Mann–Whitney U tests were conducted to examine differences in WISC-IV subtest scores and Full-Scale Intelligence Quotient (FSIQ) between the groups. Demographic variables (sex, family type, and socio-economic status) were also examined.
Results:
Children with ADHD showed significantly lower FSIQ (Mdn = 92.5) than TDC (Mdn = 103; U = 128.50, p < .001, r = .60). Pronounced deficits were evident in Working Memory subtests (Digit Span: r = .90; Letter-Number Sequencing: r = .99). Significant differences also emerged on Picture Concepts (p = .03), Matrix Reasoning (p = .002), and unexpectedly Symbol Search, on which the ADHD group scored higher (Mdn = 11.5 vs. 9, p = .002, r = .49). No significant differences were found for sex, family type, or socio-economic status on FSIQ.
Discussion:
The findings reveal a distinct cognitive profile in Indian children with ADHD characterized by severe working-memory deficits and relative preservation of verbal comprehension, alongside novel observations on perceptual reasoning and processing-speed subtests. These domain-specific impairments have important implications for designing targeted, culturally responsive interventions.
Keywords
Background
Attention-Deficit Hyperactivity Disorder (ADHD) is a prevalent neurodevelopmental condition that is characterized by enduring patterns of inattention, impulsivity, and hyperactivity, with considerable variability in cognitive and developmental outcomes across individuals. 1 Beyond its hallmark behavioral symptoms, ADHD is increasingly recognized for its complex cognitive profile, notably encompassing deficits in executive functioning, Working Memory (WMI), and Processing Speed (PSI). 2
The International Classification of Diseases, 10th Revision, emphasizes the importance of characterizing functional impairments and developmental profiles in neurodevelopmental disorders, comprehensive cognitive assessment has become central to both diagnostic formulation and intervention planning. Among available tools, the Wechsler Intelligence Scale for Children-IV (WISC-IV) remains the most widely utilized instrument for assessing cognitive functioning in school-aged children. By restructuring intelligence assessment into four distinct indexes: Verbal Comprehension (VCI), Perceptual Reasoning (PRI), WMI, and PSI, the WISC-IV provides a more nuanced and clinically informative portrait of cognitive strengths and vulnerabilities. 3
Prior research suggests that children with ADHD often demonstrate a distinct cognitive signature on the WISC-IV, marked by relative weaknesses in WMI and PSI when compared to their verbal and PRI abilities.4,5 Nonetheless, findings across studies have been mixed, underscoring the need for further research that carefully accounts for sample characteristics, cultural contexts, and comorbid conditions.
Mapping the cognitive profiles of children with ADHD, particularly in comparison to those of typically developing children (TDC), is critical for advancing our understanding of ADHD’s neurocognitive underpinnings and for informing individualized educational and clinical interventions. Previous work on autism spectrum disorders, for instance, has demonstrated that WISC-IV profiles can meaningfully capture neurodevelopmental cognitive differences when analyzed with attention to test structure and subgroup characteristics. 6 These findings highlight the potential value of extending a similarly detailed, contextually informed exploration to the domain of ADHD.
In the present study, we aim to explore and characterize the WISC-IV cognitive profiles of children diagnosed with ADHD compared to age-matched typically developing peers. Rather than testing specific hypotheses, our objective is to investigate emergent patterns of cognitive strengths and weaknesses, offering fresh insights into the neurocognitive profiles of children with ADHD. Notably, this study is conducted in India, a setting distinguished by its vast cultural, linguistic, and religious diversity. Given the relative scarcity of cognitive profiling research in ADHD within Indian populations, this work addresses a significant gap in the literature and seeks to contribute novel, culturally informed perspectives to the global understanding of ADHD-related cognitive functioning. Traditional studies have employed the use of a composite score of IQ to understand the cognitive functioning of children with ADHD. While they also utilize WISC-IV to understand atypical cognitive function, there is a lack of comparison-based studies giving specific subtest-based sensitivities that differentiate ADHD from typical development. The current study seeks to compare cognitive function as per the different subtests of WISC-IV representing different dimensions of intelligence quotient. Most ADHD research is conducted in Western and individualistic societies that fail to address demographic and sociocultural factors such as sex, family type, and socio-economic status. Therefore, understanding domain-specific deficits is essential for developing culturally valid and targeted interventions.
Method
Research Design
This study used a cross-sectional, between-groups comparative design, using WISC-IV to assess the cognitive profile of children with ADHD and TDC.
Hypotheses
We hypothesized that:
Group differences in IQ would vary by sex, socio-economic status, and family type. Children with ADHD would significantly score lower on the subtests of the WMI and speed domains.
Participants
A purposive sampling approach was used to recruit 51 participants (26 ADHD, 25 typically developing children), matched by age, gender, and education. Participants were recruited from schools in India. School types included government and private institutions; the medium of instruction recorded was English from semi-urban and urban demography.
Inclusion and Exclusion Criteria
ADHD Group
Ages 7–13 years 11 months, screened via ADHD Symptom Checklist-4 (ASCL-4). Excluded if psychiatric comorbid conditions, and children with prior stimulant/psychotherapy exposure, or neurological disorders were present.
Typically Developing Group
Same age range, enrolled in school, screened for comorbidities using the Child Behavior Checklist. Excluded if any neurological/psychiatric conditions or prior stimulant/therapy exposure existed.
Tools
BG Prasad’s Scale of Socio-economic Status: This is a widely used socio-economic status scale in India, encompassing economic features of both the urban and rural sectors. It is widely used in research because of its convenience and simplicity in classifying participants in SES living in India.
Psychometric Assessments
The psychometric tools administered were the ASCL-4 and WISC-IV.
ASCL-4 was used mainly as a screening tool to evaluate on the basis of inattention, hyperactivity, and impulsivity. It was used due to its high diagnostic sensitivity and how appropriately it captures symptoms from settings such as school and home environments, as mentioned in DSM-IV-TR. The 50-item checklist has a high inter-rater reliability with a Cronbach’s alpha of 0.86–0.947 7 in varied global contexts, and has shown repeated appropriateness in ADHD screening in Indian as well as Western children.
WISC-IV was used to evaluate the cognitive abilities of the participants. It evaluates cognitive performance through 10 subtests that are Similarities, Vocabulary, and Comprehension (VCI); Block Design, Picture Concepts, and Matrix Reasoning (PRI); Digit Span (DS) and Letter Number Sequencing (LNS) (WMI); and Coding and Symbol Search (PSI). WISC-IV was chosen intentionally due to its standardization and norms based specifically on the Indian pediatric population. Using an Indian adaptation ensures that IQ scores of participants are compared to normative scores of the Indian population in an attempt to avoid cultural bias. It is a highly reliable measure, including WMI with internal consistency >0.90. 8
Standardized administration was ensured so that high internal validity can be gained for our study, as all assessments were administered in an environment characterized by minimal auditory and visual distractions. Testing was conducted during morning hours (9:00 AM to 12:00 PM) to control for the effects of fatigue. Then the same protocol of testing was used for all participants.
Data Analysis
Analysis was carried out using IBM SPSS Statistics (version 25). Normality testing showed violation of normality assumptions of WISC-IV subtest scores (Shapiro-Wilk P < .05), hence distribution-free non-parametric inferential tests (Mann-Whitney U and Kruskal-Wallis H) were employed in the study. The Mann-Whitney U test was used for two-group comparisons of sex, whereas the Kruskal-Wallis H test was used for group comparisons of SES and family types. Effect size was calculated using the rank biserial correlation method based on the U statistic and epsilon-squared based on the H statistic, with interpretations following Field (2018). 9 Median values are reported as central tendency for the participants, and the significance level is set at .05.
Results
Analysis of demographic variables indicated that Full-Scale Intelligence Quotient (FSIQ) was stable across the sample, independent of sociodemographic factors.
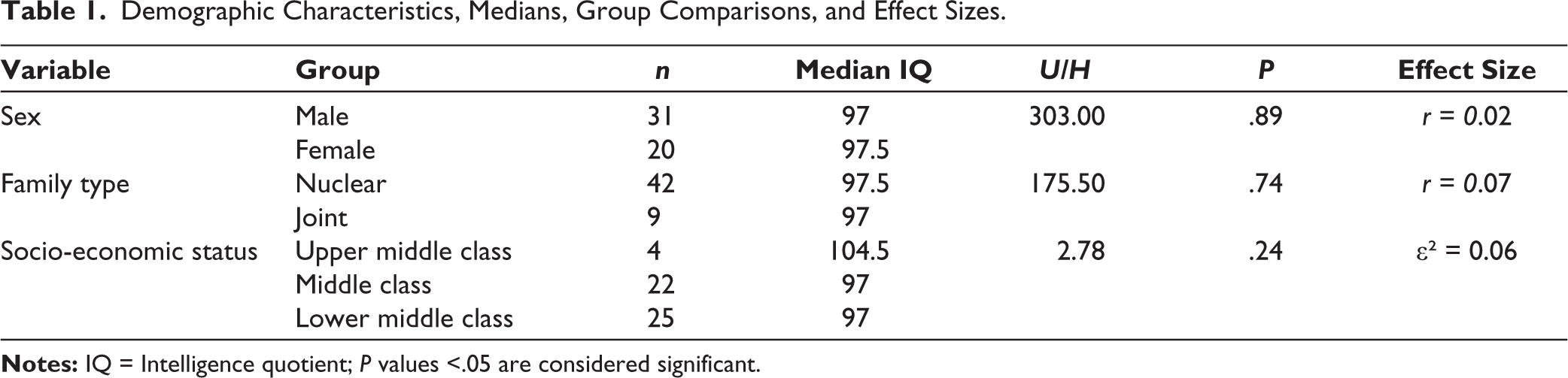
No significant difference was observed in the median IQ scores of males (Mdn = 97) and females (Mdn = 97.5) participants, U = 303.00, P = .89. The negligible effect size (r = .02) suggests that in this pediatric group, the neuro-cognitive manifestation of ADHD is not dependent on the sex of the participant. This aligns with contemporary literature suggesting that while behavioral symptoms of ADHD may differ by sex, the cognitive functions often remain similar across sexes. Comparison between children from nuclear (Mdn = 97.5) and joint (Mdn = 97) family systems revealed no significant differences, U = 175.50, p = .74, and a negligible effect size (r = .07). This implies that having an extended family support system does not significantly influence the IQ scores of the children living in small or large family member systems. A Kruskal-Wallis H test demonstrated that SES did not significantly impact cognitive scores, H(2) = 2.78, p = .24. The negligible effect size (ε 2 = .06) explains that the observed cognitive profiles are not differentiated by the economic advantage or disadvantage. Therefore, this indicates that there would be other factors that may explain cognitive differences.
The complete information is provided in Table 1.
Demographic Characteristics, Medians, Group Comparisons, and Effect Sizes.
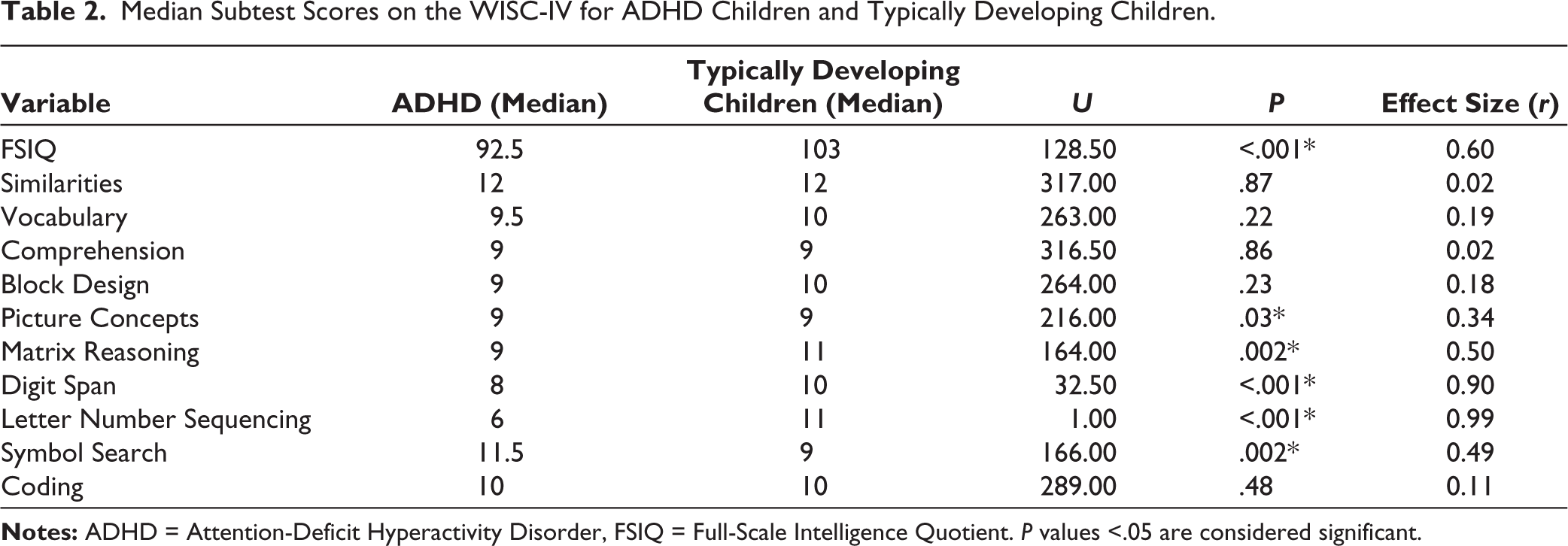
A Mann-Whitney U test was conducted to evaluate cognitive discrepancies between children with ADHD and TDC, where TDC (Mdn = 103) showed higher FSIQ scores than children with ADHD (Mdn = 92.5), U = 128.50, p < .001. The effect size was large (r = .60), indicating a large overall cognitive gap between the two groups. In similarities, there was no significant difference (U = 317.00, p = .87, r = .02). Vocabulary scores were also not significantly different (U = 263.00, p = .22, r = .19). Comprehension (U = 316.50, p = .86, r = .02) and Block Design (U = 264.00, p = .23, r = .18) showed no significant differences. No significant difference was observed in Coding scores (U = 289.00, p = .48, r = 0.11).
The most profound cognitive impairments were found in the localized domains of WMI and Fluid Reasoning. Large Deficits were noted in DS (U = 32.50, p < .001, r = 0.90) and LNS (U = 1.00, p < .001, r = .99). These near-perfect effect sizes indicate that the ADHD cognitive profile in this sample shows severe impairments in the ability to simultaneously hold and manipulate information.
As for Fluid Reasoning, Picture Concepts demonstrated a significant difference despite identical medians (Mdn = 9), U = 216.00, p = .03, r = 0.34, indicating differences in score distribution of the two groups. Last, Matrix Reasoning scores were significantly higher in TDC (Mdn = 11) compared to ADHD children (Mdn = 9), U = 164.00, p = .002, r = 0.50.
Interestingly, a significant difference was observed in Symbol Search (U = 166.00, p = .002), but with the ADHD group (Mdn = 11.5) scoring significantly higher than the TDC group (Mdn = 9) with a medium-to-large effect size (r = 0.49). The complete information is represented in Table 2.
Median Subtest Scores on the WISC-IV for ADHD Children and Typically Developing Children.
Discussion
This study aimed to conduct cognitive profiling of children with ADHD and TDC. There were several important findings that represent the cultural context of such studies in the area of neurodevelopmental disorders.
The present study focused on presenting a comprehensive cognitive profile of children with ADHD as compared to TDC using the WISC-IV. A distinct cognitive profile emerged for the ADHD group, characterized by severe deficits in WMI despite relatively intact VCI and visuospatial functions. The global FSIQ was found to be significantly lower in the ADHD group with a large effect size, where scores remained largely within the normative range, implying that cognitive impairments in ADHD are domain-specific rather than generalized. Thus, our finding supports previous research suggesting that ADHD is not associated with intellectual disability per se, but often presents with global cognitive inefficiencies that impact overall IQ scores.10,11
The lack of significant influence of sex, family type, or socio-economic status on intelligence quotient was evidenced by our study. This is consistent with the findings of a meta-analytical study by Deary et al. 12 Participants from nuclear and joint families scored similar IQ scores on WISC, as there was no significant difference in the IQ scores with respect to the family type of the participants. This is consistent with the findings of a study by Kalhotra (2014). 13 There was no significant relation between IQ scores and the socio-economic status of the participants. This was similar to the findings of the study by Hackman et al. 10 This aligns with the neurobiological model of ADHD, suggesting that the core cognition of the disorder remains consistent across different domestic and economic environments in this sample.
Domain-specific Findings
Performance on Similarities, Vocabulary, Comprehension, and Block Design did not differ significantly between groups, with negligible effect sizes. Literature further suggests that when tasks are structured and verbally mediated, children with ADHD can engage in higher-order categorical reasoning comparable to their peers. While earlier studies occasionally reported slight reductions in vocabulary among ADHD populations, 14 the current findings imply that basic lexical development remains largely intact. This also supports a differentiated conceptualization of ADHD, where difficulties arise not from a lack of social knowledge but from challenges in implementing this knowledge effectively due to deficits in attention and executive control. 11 Moreover, as Block Design assesses visual-motor coordination and spatial organization, the findings suggest that basic visual-perceptual organization may be relatively spared in ADHD. 15
The most profound impairments were localized in the WMI. The extremely large effect sizes for DS and LNS highlight the study’s most critical findings. While DS measures simple recall, LNS demands active mental manipulation of information. This highlights that complex verbal WMI is the primary cognitive deficit in this ADHD sample. This substantial effect underscores the centrality of verbal WMI deficits in ADHD, affecting not just academic achievement but broader daily functioning. 2 Unlike DS, this subtest demands active manipulation and reorganization of information, thereby placing higher demands on executive control. The findings corroborate previous research, reinforcing that complex WMI impairments are profound and central to ADHD cognitive profiles. 16
An interesting finding was reported in the PSI. The ADHD group significantly outperformed the TDC group on Symbol Search, yet no difference was found in Coding. This challenges traditional theories of universal PSI deficits. 17 It suggests that when tasks are simple and emphasize speed over accuracy, some ADHD individuals may leverage their impulsivity to perform competitively. Last, the lack of a significant difference in Coding indicates that basic visual-motor PSI may be relatively intact in ADHD, contrary to broader assumptions of pervasive PSI impairments. 18
Behavioral Observations
During the course of data collection, distinct behavioral patterns differentiated the ADHD group from their typically developing peers. Children with ADHD often exhibited noticeable difficulties in sustaining attention during test instructions, frequent off-task behaviors, and impulsivity, such as answering prematurely or shifting focus mid-task. They required more frequent prompts and redirections to maintain engagement, whereas TDC demonstrated better self-regulation, sustained focus, and organized task approaches. These behavioral observations align closely with clinical descriptions of ADHD, where deficits in behavioral inhibition, attention regulation, and WMI control are hallmark features.19,20 Notably, such behavioral variability became more pronounced during tasks demanding sustained cognitive effort, particularly during DS and LNS. These real-time observations strengthen the ecological validity of the cognitive findings and reinforce the importance of integrating behavioral assessment into comprehensive ADHD evaluations. 21
Cultural Implications
Examining ADHD within the Indian demographic context highlights the importance of cultural, social, and educational diversity. Indian children often face unique academic and familial pressures that can both amplify and mask ADHD symptoms. 22 Moreover, lower awareness levels, stigma, and the tendency to attribute behavioral difficulties to parenting or discipline issues can delay identification and intervention. 23 Unlike Western contexts that often emphasize individualized care, Indian interventions must adapt to collectivist family structures, multilingual environments, and systemic resource limitations. Thus, there is an urgent need for culturally sensitive diagnostic tools and intervention frameworks that address India’s unique sociocultural fabric rather than uncritically applying Western models. 24
Conclusion
In conclusion, this study reveals a distinctive neurocognitive profile among Indian children with ADHD, characterized by pronounced deficits in working memory and select fluid reasoning abilities (supporting Hypothesis 2), relative preservation of verbal comprehension, and an unexpected advantage on Symbol Search. Cognitive vulnerabilities were domain-specific rather than global and largely independent of sex, family type, or socio-economic status (contrary to Hypothesis 1). These findings underscore the limitations of relying solely on composite IQ scores and highlight the clinical value of fine-grained WISC-IV subtest analysis for identifying targeted strengths and weaknesses. The results carry important implications for the design of culturally responsive interventions that address core executive-function impairments while capitalizing on preserved abilities. Such contextually grounded approaches are essential for optimizing academic and functional outcomes for children with ADHD in India and similar low- and middle-resource settings.
Limitations
Several limitations are to be noted here. The sample size included 51 participants. The cross-sectional comparative design precludes causal and correlational relationships in the cognitive profiles of children with ADHD. Usage of WISC-IV might have ignored nuanced and specific executive dysfunctions seen in ADHD. Despite these constraints, the study provides insight into the stark cognitive differences in children with ADHD and TDC. The study did not account for the screen usage of the participants, pertaining to the emerging literature on the bidirectional relationship of the symptomatology of ADHD and digital media usage; the lack of a confounding variable presents as a limitation.
Future Directions
To summarize, the study provides important insights into the domain-specific cognitive profiles of children with ADHD, highlighting pronounced deficits in WMI and nonverbal reasoning, alongside relative strengths in VCI. These findings underscore the need for neuropsychological assessments to move beyond global IQ scores and focus on specific cognitive domains that critically affect daily functioning. Future research should aim to longitudinally track these cognitive patterns to examine their developmental trajectories and their predictive value for academic, social, and emotional outcomes. 15 Moreover, given the sociocultural complexities observed in the Indian context, there is a pressing need to develop culturally adapted, ecologically valid assessment tools and intervention programs that reflect the realities of Indian educational and familial environments. 25 Integrating cross-cultural validation studies and community-based interventions will be pivotal in enhancing early identification, tailoring therapeutic approaches, and improving quality of life for children with ADHD across diverse Indian settings. Future prospects can test whether ASCL-4 symptom severity (total and domain scores) correlates with WMI and PSI indices and key subtests (DS, LNS, Coding, and SS), using rank-based methods with FDR control.
Footnotes
Acknowledgements
The authors thank all participating children, their families, and the school authorities who facilitated data collection. Gratitude is also extended to the Department of Clinical Psychology, Amity University, Madhya Pradesh, for their support during the thesis phase of this study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Ethical approval was obtained from the Institutional Ethics Committee. Written informed consent was obtained from the parents/ guardians of all participants, and assent was obtained from the children before participation. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki. The study was accorded Ethical Committee Approval vide Ethics Committee AIBAS/AUMP/MPhil CP/SRC/792, dated May 1, 2025.