
Abstract
Introduction:
Inadequate knowledge of sexual and reproductive health (SRH) poses many dangers for adolescents, as they often become sexually active at this stage. This study aimed to assess students’ awareness in this area and to test whether a peer training intervention in sexual health education is feasible and effective.
Materials and Methods:
Knowledge of SRH was assessed in N = 289 students in classes 9th-12th from one school using a pre-existing structured questionnaire. N = 19 girls and N = 19 boys peer leaders were selected from them and provided education on this topic. They discussed the knowledge acquired with their classmates. Post-intervention data were collected from N = 137 students after 2 weeks. The discussions and clarifications sought by the peer leaders were written down, and thematic analysis was done. Feedback was also noted for the acceptability and feasibility of the educative session.
Results:
The majority of the students gave correct or appropriate responses for questions related to reproductive systems, sexually transmitted diseases, contraception, pregnancy, and abortion quantitatively. Thematic analysis revealed myths, misconceptions, and cultural beliefs associated with menstruation and masturbation. The questionnaire total score was significantly higher at post-intervention compared to baseline. Most of the peer leaders discussed the information learnt with their classmates and gave positive feedback for the educational session.
Discussion:
Peer training intervention may be a feasible approach for improving awareness of SRH among school-going adolescents for health promotion.
Keywords
Introduction
About one-fifth of India’s total population constitutes adolescents. 1 False and inadequate information regarding sexual and reproductive health (SRH) at this age can lead to various adverse outcomes, like risk for HIV, psychosexual disorders, unintended pregnancy, and other health risk behaviors. 2
Various studies from different regions of India have explored the knowledge and attitudes toward sexual health in school-going adolescents, and most of them have reported that there is inadequate knowledge among them.3–7 This is because discussion about sexuality and reproduction is still considered taboo.
Some prior studies from India have tried to impart sexual education in school-going adolescents by conducting didactic lectures in group settings delivered by teachers, lay counselors, or health professionals. 8 One previous study conducted two decades ago employed a peer training intervention to educate students on SRH. The trained peer leaders actively communicated the messages to their classmates. It was reported that the peer training intervention was less time-consuming and equally effective. 9
Peer education involves teaching health-related information to individuals with shared characteristics. Peers of the same age can educate their classmates through formal pedagogical methods or diffusion. In the diffusion method, they discuss the information learnt during normal conversations in informal settings within their social networks, such as during free periods, lunch breaks, and while traveling to school together. Peer-led health promotion may be more acceptable to adolescents, as they tend to learn more from peers of their own age than from adults. 10 Further, this strategy may be more effective if the peer leaders are socially influential. 11 These peer-led interventional strategies have demonstrated success in preventing tobacco abuse, sexual risk behaviors, and HIV prevention in Western countries.10–12 The current study thus aimed to revisit a peer-led sexual education intervention informed by these theories, employing a quasi-experimental design to assess its acceptability and effectiveness.
Materials and Methods
Study Setting and Sample Size
The current study was conducted by the Department of Psychiatry of a tertiary care government hospital and medical college of North India. The first phase of the study involved collecting data on school-going adolescents’ awareness of SRH. The second phase was health promotional and interventional. To assess adolescent students’ baseline awareness of SRH, the sample size was estimated based on a previous Indian study by Kuberan et al., 5 which reported that two out of three school-going adolescents had inadequate knowledge of SRH. Using the formula N = Z 2 × P × Q/L 2 and the sample size was calculated to be 266. By adding a 10% inadequate response rate, the final sample size was decided as 290.
Procedure
Prior to data collection, the office of the local District Education Officer (DEO) for Secondary Schools was approached, and the purpose of this study was explained. The office granted permission to conduct the research and selected a Government Senior Secondary School in the district’s urban area, from which an adequate sample size could be obtained.
The selected school was visited in April 2025, and the school principal and coordinator were informed about the study, and they agreed to participate in the study. Printed copies of consent forms and study information for parents of students in classes 9th–12th were handed out. Then, a day for data collection was fixed after discussing with the school coordinator. On the assigned day, students who had given assent and had their parents’ informed consent were asked to fill out forms in group settings, in the presence of the investigator and teacher, in their respective classrooms. The investigators explained the questionnaires in detail and clarified their doubts.
Their socio-demographic details were collected, and an indigenous self-rated questionnaire developed by Deshmukh and Chaniana for assessing knowledge of SRH among adolescent students was administered. 13 For this study, the initial three parts of this questionnaire, which were questions related to the reproductive system, sexually transmitted diseases, contraception, masturbation, abortion, and pregnancy were used. There were a total of 36 questions with three responses (Yes/No/Do not know). For the purpose of the statistical analysis of the present study, the appropriate or correct responses were marked as 1, and other responses or do not know responses were marked as 0. For some questions, “Yes” was the appropriate response; for others, “No” was (Table 2). This scale was also translated into Punjabi (local language) with the authors’ permission. Two independent translators, well-versed in English and Punjabi, performed forward translation followed by backward translation into English to check accuracy, and errors were corrected.
Following baseline data collection, the students’ questionnaire responses were reviewed to identify knowledge gaps and guide the preparation of educational content on SRH. A PowerPoint presentation was prepared, covering all items from the sexual health questionnaire, with emphasis on deficient areas and drawing on the United Nations Educational, Scientific and Cultural Organization (UNESCO) manual for guidance on adolescents’ sexuality education. 14 The investigators JS, AC and YS were trained by JG for the preparation and delivery of lecture material on the study subject to adolescents. The school was revisited by investigators to deliver the educational intervention. After discussions with the teachers and students, two-three most popular girls and boys from each section, from 9th to 12th classes, were selected as “Peer Leaders.” A total of 19 girls and 19 boys were selected as peer leaders. They were provided with an interactive session on reproductive and sexual health, separately for both girls and boys. They were encouraged to ask their doubts about the presentation. The lecture was delivered by JS, and the post-lecture discussion was mediated by all the investigators and team members. The sessions were held in a common area of the school library, where the group of students sat away from the library staff and teachers so they could ask the study investigators questions without hesitation. The discussions with peer leaders during the session and their queries were written down in the field notes. After sessions, the peer leaders were told to discuss what they had learned with their classmates and friends whenever they had a chance in the coming weeks.
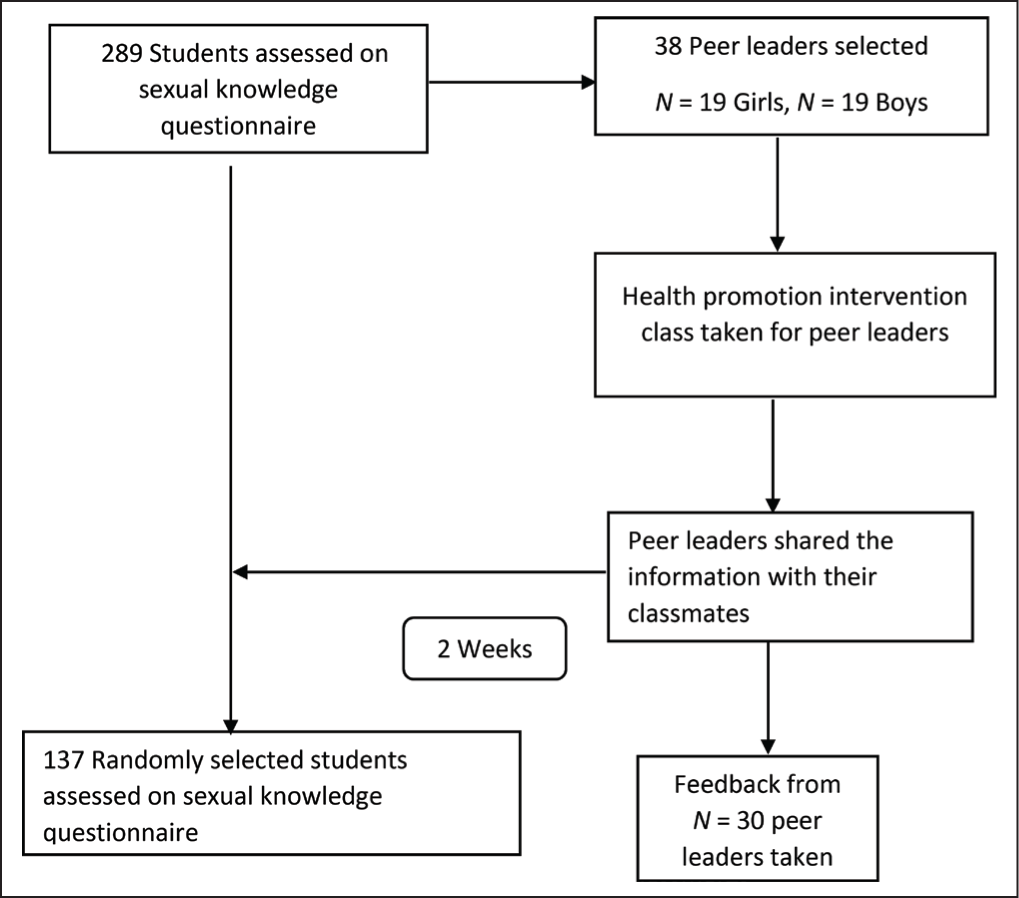
Two weeks after this session, the school was revisited. The questionnaire assessing SRH knowledge was administered to a randomly selected half of the students who had participated at baseline. On the same day, the peer leaders were called again to get their feedback and discuss their doubts in separate groups for boys and girls. N = 30 peer leaders (15 girls and 15 boys) were present that day, and the queries raised by them were also noted down. Feedback was collected to assess the feasibility and acceptability of the intervention. The field notes were reviewed for qualitative analysis, and emerging themes were coded manually. The study’s procedure and steps are shown in Figure 1.
Study Flow Chart.
Statistical Analysis
Data were entered into Microsoft Excel spreadsheets and analyzed using add-ins. Data normality was assessed using the Kolmogorov-Smirnov test, and it was decided to use nonparametric tests. Data were expressed as the median and interquartile range (IQR). The Wilcoxon signed-rank test was used to compare paired pre-intervention and post-intervention scores on SRH.
Ethics and Confidentiality
This study was conducted after obtaining permission from the Institutional Ethics Committee and the DEO. The survey was anonymous and included a confidentiality statement. Written informed consent from both students (assent) and parents/guardians, in their vernacular language (Punjabi) were taken. The ICMR guidelines for conducting biomedical research were followed as applicable.
Results
A total of N = 289 school-going adolescents (age range 12–19 years) were included in the study. By coding the correct/appropriate responses as 1, and incorrect and “Don’t know” responses as 0, the Cronbach’s alpha was found to be 0.671 for section A (Knowledge of male and female reproductive system), 0.587 for section B (regarding STDs, contraception, masturbation and sex-related questions), and 0.747 for section C (knowledge regarding pregnancy and abortion), overall suggesting acceptable internal consistency.
Impact of Educative Intervention on Knowledge of SRH
At baseline, knowledge regarding SRH was not significantly different among males and females (P = .390). Two weeks post-intervention, the questionnaire on knowledge of SRH was administered to N = 137 randomly selected students among the initially recruited students to check whether there was any change from baseline. The median scores increased significantly from baseline to post-intervention among both genders (Table 1). The effect size r for the Wilcoxon test was found to be 0.31 (Z = −3.63), indicative of a medium effectW.
Median Scores on the Knowledge of Sexual Health Questionnaire at Baseline and Post-intervention.

*P value < .05, Significant; **P value < .01, highly significant, ***P value < .001, very highly significant.
Responses of Students to Individual Questions at Baseline and Post-intervention
At baseline, the majority of the students answered correctly (appropriately) for most of the questions on sexual health except for the questions on oral contraceptive pills as a safe sexual practice (Question B.4), masturbation causes weakness (Question B.5), masturbation is a sin (Question B.6), talking about sex is a sin (Question B.7), homosexuality is unnatural (Question B.9), and one act of sexual intercourse can lead to pregnancy (Question C.4). Post-intervention, the proportion of students who gave correct (expected) responses increased on these questions. However, out of these questions, the majority of the students still did not give the correct answers to questions on oral contraceptive pills as a safe sexual practice (Question B.4), and masturbation causes weakness (Question B.5) (Table 2).
Distribution of Students with Correct Responses on Individual Items of the Sexual Knowledge Questionnaire at Baseline and Post-intervention.
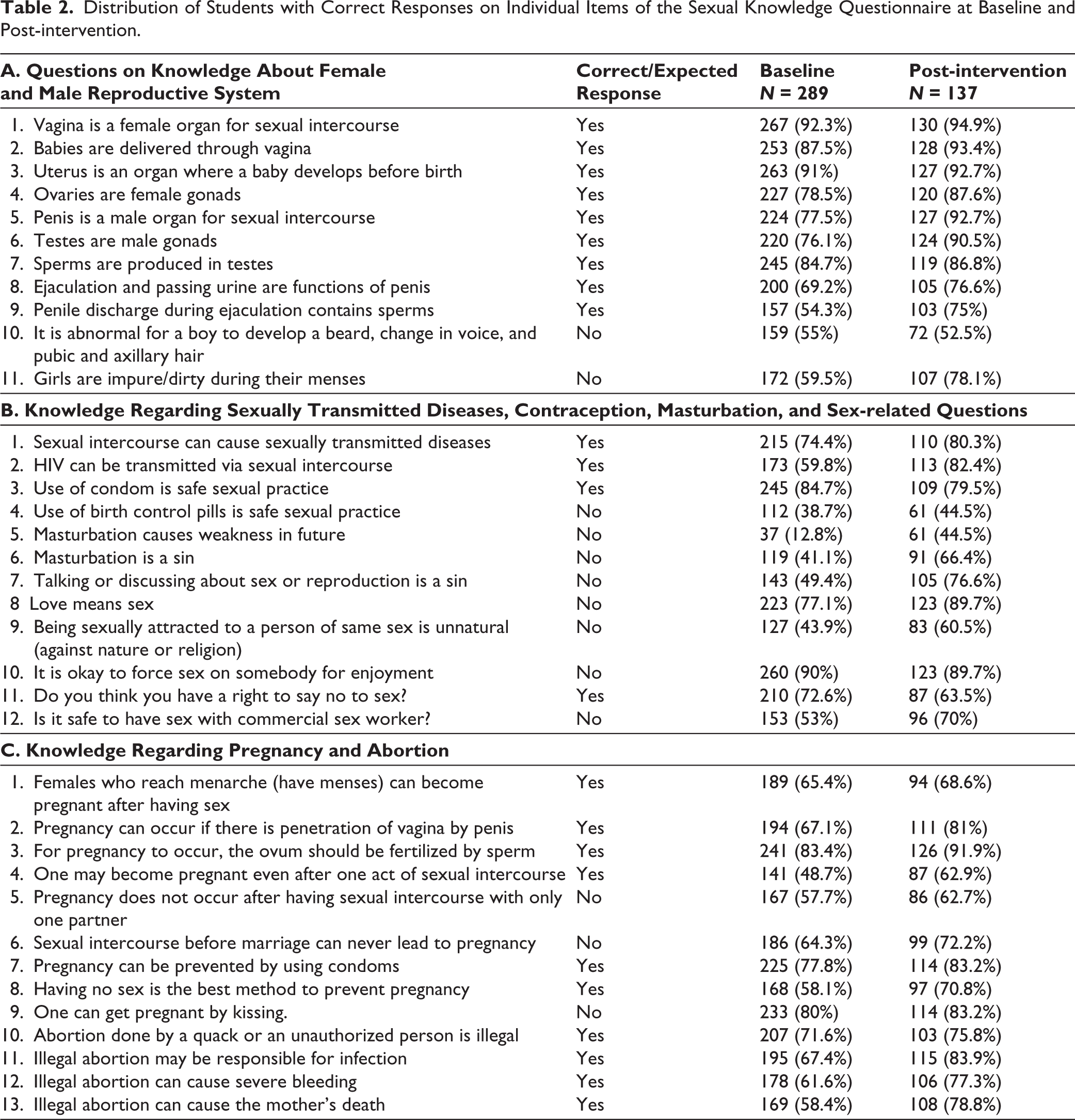
After the intervention, the percentages of correct (appropriate) responses increased regarding reproductive organs, ejaculation, sperm production, HIV transmission, masturbation being a sin, pregnancy and abortion. The percentage of correct (appropriate) responses on male puberty-related changes (Question A.10), use of condoms as a safe sexual practice (Question B.3), forcing sexual activity (Question B.10), and the right to say “no” to sex (Question B.11) did not increase post-intervention (Table 2).
Qualitative Summary of Sessions with Peer Leaders
During the educational sessions, the male and female reproductive organs and systems, and bodily changes during puberty were explained with the help of diagrams in the PowerPoint presentation. All the topics of the questionnaire related to reproductive systems, puberty, menstruation, menstrual hygiene, masturbation, sexual intercourse, fertilization, risk of STD, risk of pregnancy, contraception, homosexuality, right to say “no,” illegal abortion, and so on, were covered. During the session, it was observed that male students were hesitant to speak with female investigators, so they were given a separate area to discuss with male team members. Qualitative analysis of field notes was done, and separate themes were identified for sessions with male and female peer leaders.
Thematic Summary of Sessions with Female Peer Leaders
The major themes identified for the sessions with female peer leaders involved concerns related to menstruation, vaginal discharge, misconceptions on sexual intercourse and other queries related to reproductive health as described below.
Lack of Awareness on Menstruation
Most female students acknowledged that they had not heard anything about menstruation before menarche. They said that even their mothers had not informed them of anything. Some had heard about it from their friends, and one student said that she did not even tell her mother about her menarche and had been managing menstruation on her own since the beginning. They said that no one had ever explained to them the reason for menstruation. The 11th and 12th biology students said that they learnt about the reproductive system and menstruation by reading their syllabus books. The female students shared the prevalent cultural beliefs that some of them were not supposed to go to temples and the kitchen during menstruation. A few of them said that they would not care and would go to the kitchen during periods also. Some of them said that there was no restriction on them during menstruation in their homes. This was appreciated, and it was emphasized that menstruation is a natural process.
They asked about the normal duration of periods and menstrual cycles, clarity on irregular or heavy bleeding, the diet that should be taken during menstruation, and pain during menstruation. Many of them said that they bear the pain during menstruation without taking any medicine. Their queries were addressed, and they were informed that they can take normal painkillers available at home to manage dysmenorrhea.
Concerns About Vaginal Discharge
They asked about the relevance of white discharge (leucorrhea) and whether they should be worried about it. They were informed that it is mostly normal. It changes in amount and form during certain phases of the menstrual cycle, and other relevant information related to STDs was provided.
Misconceptions Related to Sexual Intercourse
A few students were curious about the hymen and said that they had heard that intercourse for the first time may be very painful and lead to heavy bleeding. A few other students also asked that can the hymen can be torn without intercourse. They were explained the anatomy with diagrams, and explained about the prevalent myths and their concerns were addressed.
Queries Regarding Male Reproductive System
Some students wanted to get clarification regarding the male reproductive system. They asked about reasons for male masturbation and sought clarity on the term “ejaculation,” and they asked about the difference between semen and sperm. Their queries were addressed again using diagrams.
STD-related Queries
They sought clarification on the symptoms of STDs. They were informed about rashes and other health risks. A few of them did not know the meaning of commercial sex worker, and it was explained to them. They raised queries related to male and female contraceptives, and which was better. Barrier methods of contraception were explained to them. They asked whether birth control pills were safe. It was explained to them that birth control pills, when taken regularly, prevent pregnancy, but do not prevent STDs.
Other Queries Related to Contemporary Issues
A few girls raised their queries about polycystic ovarian disorder (PCOD). One girl said that she had heard that girls with PCOD gain weight, and she was concerned about a friend who was overweight and would not exercise. They were explained the symptoms and causes. They were informed about the role of regular physical activity in staying healthy. The students also asked about in vitro fertilization, which was explained.
Thematic Summary of Sessions with Male Peer Leaders
The major identified themes from the field notes involved misconceptions and myths related to masturbation, ejaculation time and the size of the penis, described as follows:
Myths Related to Masturbation
The students were mainly concerned about the potential harm of masturbation. They said they had heard from their friends in the neighborhood that it might lead to weakness in the body, weight loss, weakness of eyesight, a decrease in blood levels, and the development of pimples on the face. Some of them felt that they would feel sleepy after masturbation. Their concerns were acknowledged, and they were informed that there were many myths prevalent in society related to masturbation and that it was harmless. They also asked about the normal frequency of masturbation and whether it is normal to masturbate daily. Some of them were concerned that masturbating daily might be affecting their performance in sports. They were giving the example that when they would masturbate often, they would not be able to do batting and bowling properly while playing cricket. So, they would decrease the frequency of masturbation in between. It was explained to them that every individual has different needs, and it does not lead to weakness in the body, even if done daily.
A few students were concerned about the harms of nightfall/nocturnal emissions. Their doubts were addressed, and they were also informed about the physiology and anatomy of the reproductive system to emphasize that it was normal.
Misconceptions Related to the Time of Ejaculation
They asked about the normal time for ejaculation. Some of them had watched pornographic videos and noted that the time to ejaculation was 20–30 min. They reported that their own time to ejaculate during masturbation was 2–3 min. They were reassured, and their myths were addressed regarding the normal time of ejaculation. They were informed that pornographic videos are often fake and made after video editing. A few boys also said that they had heard about the role of drugs like “Shilajeet” in improving the duration of ejaculation. They were informed that these were misconceptions and that using drugs may lead to many harmful consequences.
Misconceptions Related to the Size of Genitalia
They were also concerned about the normal size of the penis. They had compared the sizes to the people in the videos and to some of their friends. Their misconceptions were addressed by describing the reproductive systems again. They were suggested to avoid watching pornographic videos. They were asked for what other reasons pornography videos should be avoided; some of them acknowledged that it may lead to addiction. They were appreciated for their responses.
Queries Related to the Usage of Condoms
Some of them asked about the ways HIV can be transmitted and whether oral intercourse could potentially spread it. A few of them acknowledged that they do not derive that much pleasure while using condoms. The importance of using condoms was stressed, and their queries were addressed. They were informed that condoms do protect against HIV, but only if worn properly. The male peer leaders were also shown a short YouTube video on the correct way of wearing a condom. They were also told that condoms do not prevent other skin-to-skin contact infections.
Thematic Summary of Feedback Sessions
During the feedback session, the peer leaders were asked whether they could discuss the information learned with their friends and to share their experiences. They were also asked how the educational session helped them in increasing their knowledge and whether they could understand everything.
Discussion with Classmates
Most students were informed and were able to discuss the knowledge they had acquired with their classmates; several mentioned that having access to a PowerPoint presentation would have facilitated the discussion. Some female students said that when they discussed the topic, they felt their friends were not very interested, and some friends smiled or seemed embarrassed. They were encouraged to try again, as some hesitation is normal and expected among students. Conversely, some peer leaders reported that their friends engaged enthusiastically and expressed that they should have attended the session too. Some peer leaders said they could not find time to discuss the material they had learnt with their friends but planned to do so later.
Information Learnt by Peer Leaders
The peer leaders were also asked to share what new information they learned from the educational session. Most female students reported that they understood the reasons behind menstruation, learnt information about intercourse, fertilization, and pregnancy, and no one had previously told them about these topics. Some female students said the information regarding normal vaginal discharge, symptoms of STDs, urinary tract infection, illegal abortion, pubertal changes, masturbation, and contraceptives was new to them. The male students expressed that they learnt that masturbation and nightfall were harmless; their misconceptions related to the time of ejaculation, size of penis, and effects of drugs were resolved.
General Feedback
All peer leaders stated that they understood the lecture and that the sessions satisfactorily answered their queries and doubts. Students and teachers said that more such sessions should be held in the future. Overall, positive feedback was obtained from the peer leaders and the teachers regarding the study procedure and sessions.
Discussion
The present study was conducted to explore the knowledge about sexual health among school-going adolescents and to assess whether a peer training intervention is effective in a quasi-experimental phase. It was found that the peer training intervention appeared feasible, and an increase in awareness scores was observed following the intervention.
Post-intervention, there was a significant improvement in the scores of knowledge on the SRH questionnaire with a moderate effect. These findings are consistent with the possibility that peer leaders shared the information with their classmates. By educating only 38 students, information was diffused to a much larger number of students in a short span of time. Similarly, Parwej et al. 9 reported that the peer training intervention was less time-consuming and equally effective. Other previous studies also reported that health promotion interventions have been associated with improvements in adolescents’ knowledge, but most researchers had to educate several batches of students to achieve this.8,15-18
The majority of the participants answered correctly for most of the questions related to the reproductive system, STDs, contraception, sex-related questions, pregnancy, and abortion. A lesser proportion of students answered correctly (appropriately) in some areas of SRH, such as myths related to masturbation, talking about sex, homosexuality, and safe sexual practices, according to the quantitative data. Many previous studies from India have also reported poor knowledge among school-going adolescents in most areas related to SRH.3–6 This could be due to regional variation and different questionnaires used for assessment. The proportion of students who answered these questions (and most of the other questions) correctly increased post-intervention. However, the majority of the students still believed that masturbation could cause weakness. This deeply ingrained cultural belief might not have changed with a single peer education session. Further, the responses on male puberty-related changes, use of condoms as a safe sexual practice, forcing sexual activity, and the right to say “no” to sex did not change much. This may be because the peer leaders did not discuss these topics much.
Thematic analysis of the data showed that adolescents get information on SRH from their friend circle, and no parent or teacher educates them on this pertinent topic. They shared their experiences, their existing knowledge, reflecting prevalent myths and misconceptions on many sensitive issues. Sessions with female peer leaders revealed the cultural beliefs associated with menstruation, and they actively sought information on menstrual cycles, dysmenorrhea, vaginal discharge, sexual intercourse, and prevention of STDs. Male peer leaders were mainly concerned about the myths prevalent in society related to masturbation, the size of the penis, and the time of ejaculation. The session’s observations showed that, though they were initially hesitant to discuss, they later sought clarification on topics that were not even present in the questionnaire and were closely related to contemporary myths in India. 19 Discussing these issues with investigators was expectantly not easy, but the quality of their questions showed that they trusted the team members and were very concerned about those issues. Qualitative analysis of feedback shows that they learnt new information and the sessions satisfactorily addressed their queries. The peer leader and teachers gave positive feedback, indicating that the intervention was acceptable and feasible.
The strengths of the present study included the use of a mixed-methods intervention. The limitations included assessing only SRH knowledge, without assessing attitudes or practices. Second, only one follow-up post-intervention was conducted. Long-term follow-up may help retain learnt material better. Third, no control group was taken to compare the improvement in the knowledge score. This could not be done due to time constraints and feasibility issues. Additionally, no formal soft-skills training was provided during the session. However, the students were encouraged to discuss the information with as many other students as possible, and the importance of this topic was emphasized by explaining that accurate information could reduce suffering and help save lives. Another limitation was that audio recordings and transcriptions were not done for thematic analysis, which could have made the reporting more descriptive. Further, social desirability bias could not be ruled out in the subjective reporting during feedback.
Conclusion
The results of the present study helped identify knowledge gaps regarding SRH among school-going adolescents in this area of India. There are misconceptions and myths prevalent among both male and female adolescents that may lead to adverse consequences in the future. There is a dire need for correct scientific information on SRH among adolescents. The peer training intervention conducted in this study during the quasi-experimental phase was associated with a moderate effect. Overall, positive feedback was obtained from the peer leaders regarding this intervention. Adolescents may be more receptive to learning about SRH from their peers. Peer training interventions may be a promising approach for disseminating SRH information among adolescents. However, controlled studies with longer follow-up are needed to establish effectiveness.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Written Informed Consent and Assent were taken from all the participants. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki. The study was accorded Ethical Committee Approval vide the Institutional Ethics Committee (Approval No. Trg.9(310)2024/32876-77, dated 25.10.2024).