
Abstract
Introduction:
Children with autism spectrum disorder (ASD) often exhibit atypical sensory responses, including hyper-reactivity, hypo-reactivity, and sensory-seeking behaviors. Assessing the severity of these patterns is essential for early identification, individualized intervention, and progress monitoring. Although several international measures exist, culturally relevant and context-specific tools are necessary for accurate assessment in the Indian context. This study aimed to develop and conduct content validation of the Indian Scale for Assessment of Sensory Reactivity in Autism (ISARA).
Materials and Methods:
A two-phase mixed-method design was employed. An in-depth interview (IDI) guide was developed through a literature review and reference to existing sensory reactivity scales. It was refined with expert input from psychiatrists, child psychologists, speech-language pathologists, and occupational therapists experienced in ASD care. IDIs were conducted with parents (n = 20), audio-recorded, transcribed, and translated from Hindi to English. Manual coding and thematic analysis identified emerging sensory reactivity patterns. Experts evaluated face validity, followed by qualitative feedback to refine items. Item-level content validity ratio (I-CVR), Domain-level Content Validity Index (D-CVI) and Scale-level Content Validity Index (S-CVI) were computed for content validation.
Results:
Thematic analysis yielded four domains: sensory hyper-reactivity, sensory hypo-reactivity, sensory-seeking, and attentional and socio-emotional response. Sixty-three items (I-CVR = 0.8–1.0) were retained. D-CVI ranged from 0.83 to 0.92, indicating good to excellent validity, with an overall S-CVI of 0.86.
Discussion:
ISARA demonstrated strong content validity and cultural relevance for assessing sensory reactivity in Indian children with ASD, providing a foundation for further psychometric validation in larger samples. Future research will focus on establishing the psychometric robustness of ISARA.
Keywords
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental condition that typically appears in early childhood and is primarily characterized by persistent difficulties in social communication and interaction, along with restricted and repetitive patterns of behavior, activities, or interests. 1 Beyond these core features, challenges with sensory processing are highly prevalent but often underrecognized in individuals with ASD. Sensory processing may manifest in multiple forms, including heightened sensitivity (hyper-reactivity), reduced sensitivity (hypo-reactivity), or unusual sensory-seeking behaviors. Recognizing their significance, DSM-5 2 incorporated sensory processing abnormalities as one of the defining criteria for ASD. Specifically, they are categorized under the restricted and repetitive behavior domain and are described as hyper- or hypo-reactivity to sensory input or unusual interests in sensory aspects of the environment. 1 These issues can span across multiple sensory modalities such as vision, hearing, touch, taste, smell, proprioception, and vestibular functioning and may lead to overwhelming discomfort, avoidance behaviors, or, conversely, intense fascination with sensory stimuli. For example, children with ASD (CwASD) may cover their ears in response to ordinary sounds, avoid certain textures in food or clothing, or seek excessive movement and tactile input. Such sensory processing difficulties not only influence daily functioning and learning but also contribute significantly to behavioral challenges, anxiety, and difficulties with social participation, thereby underscoring the importance of their systematic assessment and management. 3 Accurate identification of specific patterns of sensory responses and their associations with emotional, behavioral, and cognitive functioning is crucial for guiding the selection of appropriate interventions. Tailoring or modifying sensory environments and components can not only reduce maladaptive behaviors but also promote the overall well-being of families and enhance the quality of life of CwASD. Importantly, the formal inclusion of atypical sensory behaviors as a diagnostic criterion in DSM-5 2 underscores their central role in ASD management and highlights the pressing need to develop reliable and valid assessment tools for measuring these sensory features.
Sensory processing difficulties are a cross-cutting feature of ASD and are closely associated with restrictive and repetitive behaviors (RRBs), which often function as strategies to regulate atypical sensory input. Repetitive actions such as hand flapping or rocking may help children cope with sensory over- or under-stimulation, while hypersensitivity can result in avoidance of certain stimuli, and hyposensitivity may lead to sensory-seeking behaviors.4,5 These behaviors provide a sense of predictability and control in overwhelming sensory (L54) environments. Sensory processing challenges are also linked to difficulties in socio-emotional reciprocity, as sensory dysregulation can impair a child’s ability to perceive and respond to social-emotional cues. Consequently, understanding how CwASD interact with caregivers and others is essential for developing more individualized and effective intervention approaches. 6
Some parent-scored instruments to assess sensory symptoms in CwASD, include the sensory profile-2, 7 the sensory behavior questionnaire, 8 the sensory experiences questionnaire, 9 and the sensory processing measure (home form). 10 These parent-report measures are valuable for collecting information on children’s sensory-related behaviors. However, a major limitation of these assessment tools is their reduced capacity to capture the sensory processing difficulties in CwASD in our cultural context. In addition to parent-report measures, several clinician-administered observational assessments include the sensory processing scale assessment 11 and the sensory processing measure for preschool. 12 Despite their utility, these tools are constrained by lengthy administration times and limited applicability across age groups. Furthermore, because younger CwASD often experience significant challenges in language and cognitive functioning, they are less able to reliably self-report their sensory experiences. 13
The INCLEN diagnostic tool for ASD (INDT-ASD) 14 and the Indian Scale for Assessment of Autism (ISAA) 15 are well-validated and culturally appropriate instruments for the identification and severity assessment of autism in the Indian context; their primary focus remains on core diagnostic domains such as social interaction, communication, restricted and repetitive behaviors. Sensory features, although clinically significant in autism, are not comprehensively assessed as a distinct domain within these tools. Given the growing recognition of sensory reactivity as a key component of ASD, there remains a need for specialized instruments that provide a detailed and domain-specific evaluation of sensory reactivity patterns with direct implications for individualized treatment planning and intervention. To address these gaps, there is a need to develop a sensory reactivity questionnaire for CwASD in India that is accessible, easy to administer, and suitable for a broader range of mental health professionals. Accordingly, the present study aimed to capture parental experiences and expert perspectives on patterns of sensory reactivity and to develop and conduct content validation of a sensory reactivity scale designed to help professionals and parents observe diverse dimensions of sensory behavior, including hyper-reactivity, hypo-reactivity, sensory-seeking patterns, and related attentional and socio-emotional features.
Methods
Study Design
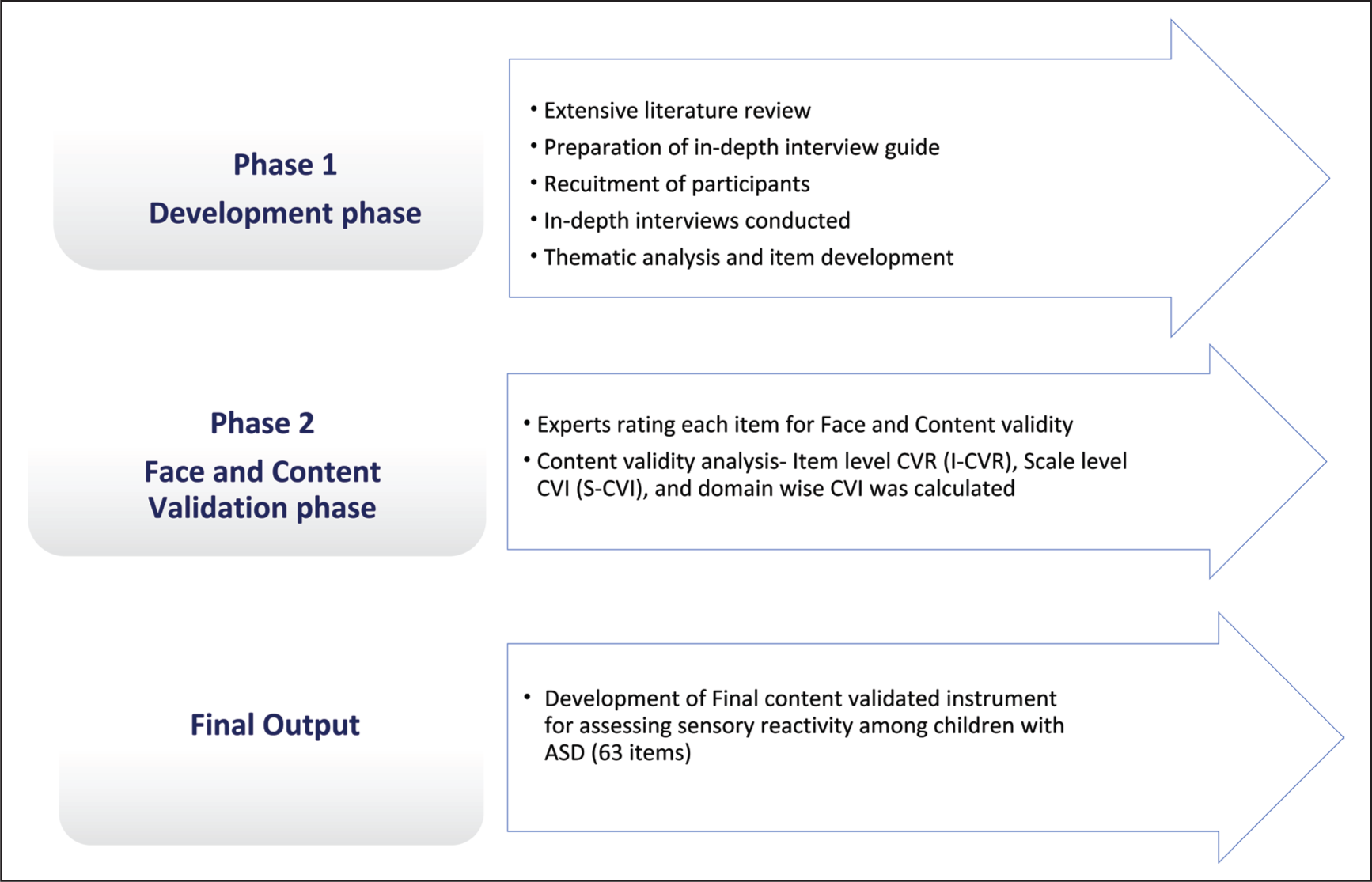
The study was carried out in two phases using a sequential mixed-method research design using both qualitative and quantitative methods (Figure 1 depicts a schematic representation of the flow of the study).
A Schematic Representation of the Flow of the Study.
IDI Guide Development
The in-depth interview (IDI) guide was developed to identify and clearly define key domains of sensory reactivity in children with ASD. A thorough review of the literature and existing scales measuring sensory reactivity, by systematically reviewing tools and questionnaires that evaluate sensory responses across various major modalities such as visual, auditory, tactile, and others, was conducted. The literature review also analyzed the theoretical bases and psychometric strengths of these instruments to map essential domains, including sensory hyper-reactivity, sensory hypo-reactivity, sensory-seeking and their association with attentional and socio-emotional functioning. We focused especially on the sensory profile 2 questionnaire for the development of our interview guide. It is a caregiver questionnaire consisting of 86 items under four quadrants of seeking, avoiding, sensitivity, and registration; scored on a five-point Likert scale for assessing the levels of severity: 1-almost never (10% or less), 2-occasionally (25%), 3-half the time (50%), 4-frequently (75%), and 5-almost always (90% or more). 7 The guide was refined for culture-appropriate content with feedback from experts, including psychiatrists, child psychologists, speech-language pathologists, and occupational therapists specializing in ASD. Based on this synthesis, a final interview guide with proposed items was prepared and subsequently refined with inputs from experts. Open-ended questions focused on the child’s preferences, unusual behaviors, differences noticed compared to peers, responses to various situations, and daily living activities. Closed-ended questions examined sensory responses across multiple domains, namely, visual, auditory, tactile, olfactory, gustatory, vestibular, and proprioceptive, as well as attentional and socio-emotional aspects. Concluding questions invited parents to share any additional observations or details not previously discussed.
Participants
Phase 1 (Qualitative)
The inclusion and exclusion criteria, which have been described in detail in our protocol paper 16 briefly were: parents of children with DSM-5 ASD diagnoses but without psychiatric or physical comorbidities which could influence the evaluation of sensory issues. Considering their prevalence, CwASD with comorbid attention deficit hyperactivity disorder, mild intellectual disability, or anxiety disorders were not excluded.
Procedure and Setting
Children presenting to the child guidance clinic of a free tertiary care hospital who were clinically diagnosed with ASD as per DSM-5 were screened after obtaining parental consent, and finally, 20 parents of CwASD were enrolled. Audio-recorded interviews (open and closed-ended questions in Hindi, the preferred language) were conducted at the child guidance clinic by a multidisciplinary team comprising a psychiatrist, clinical psychologist, and an occupational therapist. Socio-demographic information was obtained using a semi-structured proforma. When new topics or patterns emerged, additional probing was undertaken to explore in-depth. After each session, interviews were transcribed and translated from Hindi into English. Thematic analysis was then performed manually to identify recurring patterns and core themes. Data collection continued until thematic saturation was reached.
Data Analyses (Phase 1)
All data was entered into password-protected files. For socio-demographic analysis, Jamovi software was used for quantitative data. For qualitative data, the steps used are described in detail. The process followed five steps of phenomenological thematic analysis. Initially, the researchers developed a holistic understanding of sensory reactivity, then segmented the transcripts into meaningful units to explore specific parental experiences. These meaningful units were elaborated into detailed thematic structures, which together formed the conceptual basis of sensory reactivity as experienced by parents of CwASD. 17 All audio-recorded interviews were repeatedly listened to, reviewed and transcribed. The transcripts were then translated from Hindi to English following established guidelines for qualitative research translation, and accuracy was verified by all members of the research team. 18 Each transcript was carefully read and re-read to ensure consistency with the original data, facilitating a deep familiarization with participants’ narratives. Manual coding was conducted independently by one psychologist, one psychiatrist and two occupational therapists. Emerging codes were compared, refined, and grouped to identify subthemes. Subsequently, superordinate themes through a stepwise process involving open, axial, and selective coding were derived. Categories and themes were iteratively reviewed, compared, and cross-checked by another researcher to ensure completeness and accuracy. 19 The analysis emphasized the relationships between themes and supporting participant quotations, ensuring that interpretations were grounded in the data. Interviews were structured to progress from general to specific questions, and the use of audio recordings allowed for the capture of emotional tone, pauses, and non-verbal cues, enriching the analysis. Analytical rigor was maintained through internal review and consensus among all researchers.
Item Generation
Items for the sensory reactivity scale (tentatively named Indian Scale for Assessment of Sensory Reactivity in Autism [ISARA]) were generated from four primary sources, including the author’s clinical experience with CwASD, an exhaustive review of literature on sensory processing and reactivity, IDIs with parents, and consultations with subject-matter experts and mental health professionals working in the field of ASD. The initial pool of items was framed to represent the sensory reactivity dimensions. Care was taken to avoid the use of past tense, double negatives, and complex or ambiguous sentence structures. Cultural relevance and linguistic appropriateness were also ensured to enhance the comprehensibility and applicability of the scale for the target population.
Questionnaire Formation (Phase 2: Face Validity)
It encompassed all the processes required to check the representativeness and relevance of the elements. Items for face validity were examined for consistency, accuracy, and fitness for the sensory reactivity dimension. This process focused on at least three features of the test items: relevance of item content to the domain, balance of coverage of the content domain, and technical quality of the items, response formats, and scoring procedures. A total of 10 experts were selected to reduce the likelihood of a chance agreement. They were included based on their expertise in the content area and instrument development, having at least 5 years of working experience with CwASD. The experts were instructed to emphasize the items’ clarity, specificity, and grammatical structure; add or delete items; and make any additional suggestions. Congruency, readability, accuracy, language, and representativeness were all prioritized. A five-point Likert scale format was adopted. The response categories and respective scores were: (0) Never experienced/never exposed, (a) occasionally, (b) infrequently, (c) frequently, and (d) almost always. A high total score would indicate higher sensory issues in the child.
Judgment-quantifying Stage (Phase 2: Content Validity)
It involved the assessment of the content validity of the individual items (Item-level content validity ratio [I-CVR] = Item-level content validity ratio) and the complete questionnaire (Scale-level Content Validity Index [S-CVI] = Scale Content Validity Index). For the assessment of content validity, Lawshe’s method was applied using the formula (ne – N/2)/(N/2) where nₑ represents the number of panellists indicating an item as “essential” and N denotes the total number of panellists. Ten experts independently rated each item on a four-point scale: (a) Must be retained, (b) May be retained, (c) May or may not be retained, and (d) Must be removed to avoid biasing their responses toward a particular option. After collecting the ratings, the number of experts who classified each item as “Must be retained” or “May be retained” was counted. These ratings were then used to compute CVR, which quantitatively reflected the essentiality of each item, ultimately helping determine which items should be retained or revised. Items with a CVR value below 0.60 were removed, while others were revised based on expert feedback. Finally, items having a CVR greater than or equal to 0.80 were retained. D-CVI and S-CVI were obtained by adding the item-level CVR 0.8 or 1 of all items divided by the total number of items. 20
Ethical Procedures
The study has been approved by the institutional ethics committee (AIIMS/Pat/IEC/2022/1022; dated March 3, 2023), and was carried out in accordance with the 2017 ICMR ethical principles for biomedical research. Children were enrolled in accordance with precisely stated inclusion and exclusion criteria. Parents of participating CwASD provided written informed consent. The information gathered from the participants was categorized or anonymized to safeguard their identity, and their privacy ensured intact while reporting the findings of the study. At any time, parents and /or participants could withdraw from the study. The study was registered with the Clinical Trial Registry of India (CTRI/2024/09/074306).
Results
Socio-demographic and Clinical Profile
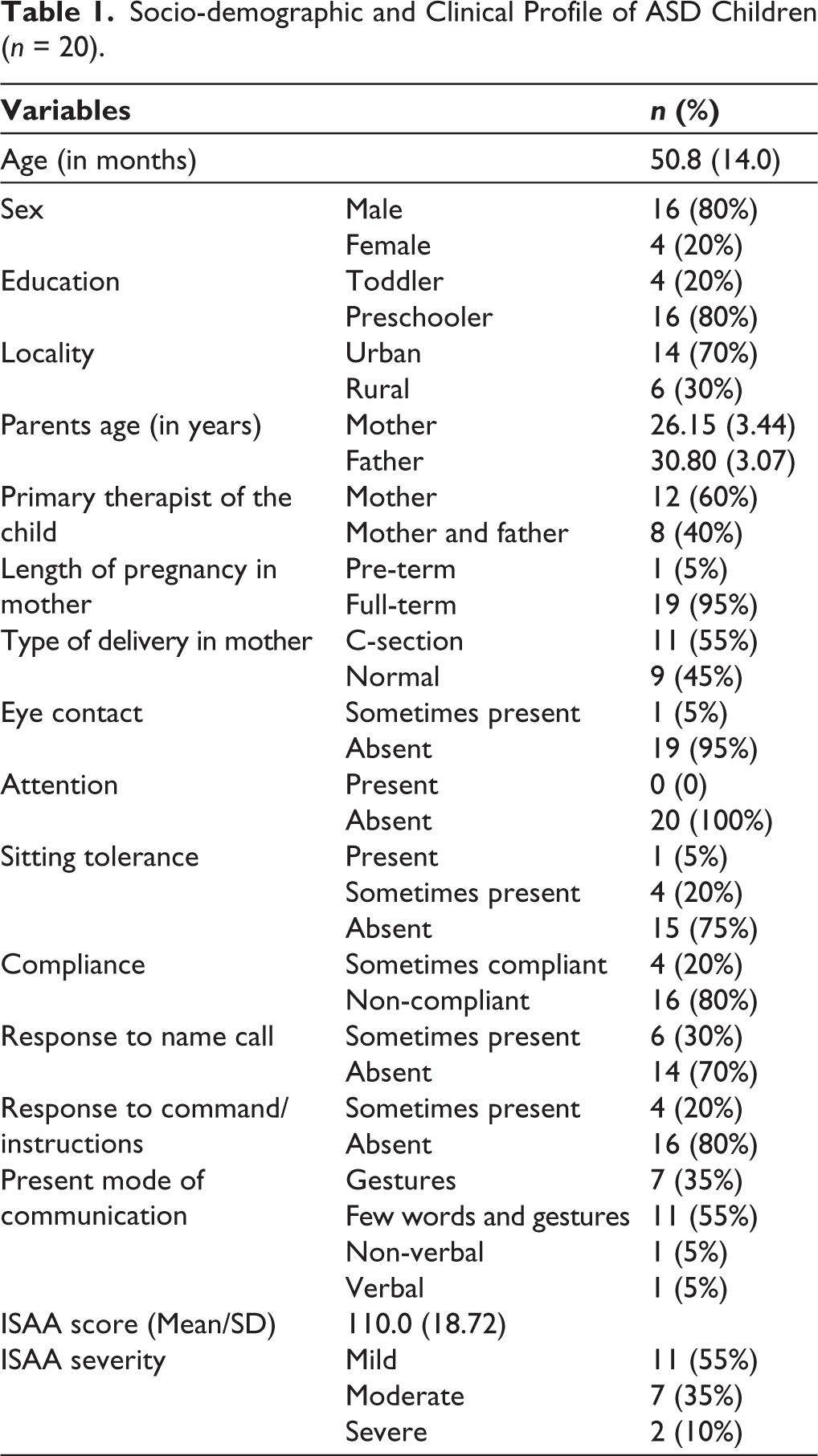
We recruited 20 parents of CwASD with a mean age of 50.8 months (SD = 14.0). Most ASD children were males (80%) and preschoolers (80%), with most residing in urban areas (70%). Mothers were reported as the primary therapists in 60% of cases, while both parents were involved in 40%. Clinical observations revealed absent eye contact in 95% of children, absent attention in all, and poor sitting tolerance in 75%. Non-compliance was reported in 80%, while 70% did not respond to name call, and 80% did not respond to instructions. In terms of communication, 55% used a few words with gestures, 35% used gestures alone, and very few were verbal (5%). The mean ISAA score was 110.0 (SD = 18.72), with 55% categorized as mild autism and 35% as moderate autism and 10% as severe autism (Table 1).
Socio-demographic and Clinical Profile of ASD Children (n = 20).
Thematic analysis of parents’ narratives revealed four major superordinate themes reflecting the lived experiences of CwASD: Sensory hyper-reactivity, Sensory hypo-reactivity, Sensory-seeking, Attentional and socio-emotional response. Each theme comprised multiple subthemes capturing the nuanced challenges faced by families (Table 2).
Thematic Analysis Showing Various Themes of Sensory Reactivity from the Lived Experiences of Parents (N = 20) of Children with ASD.
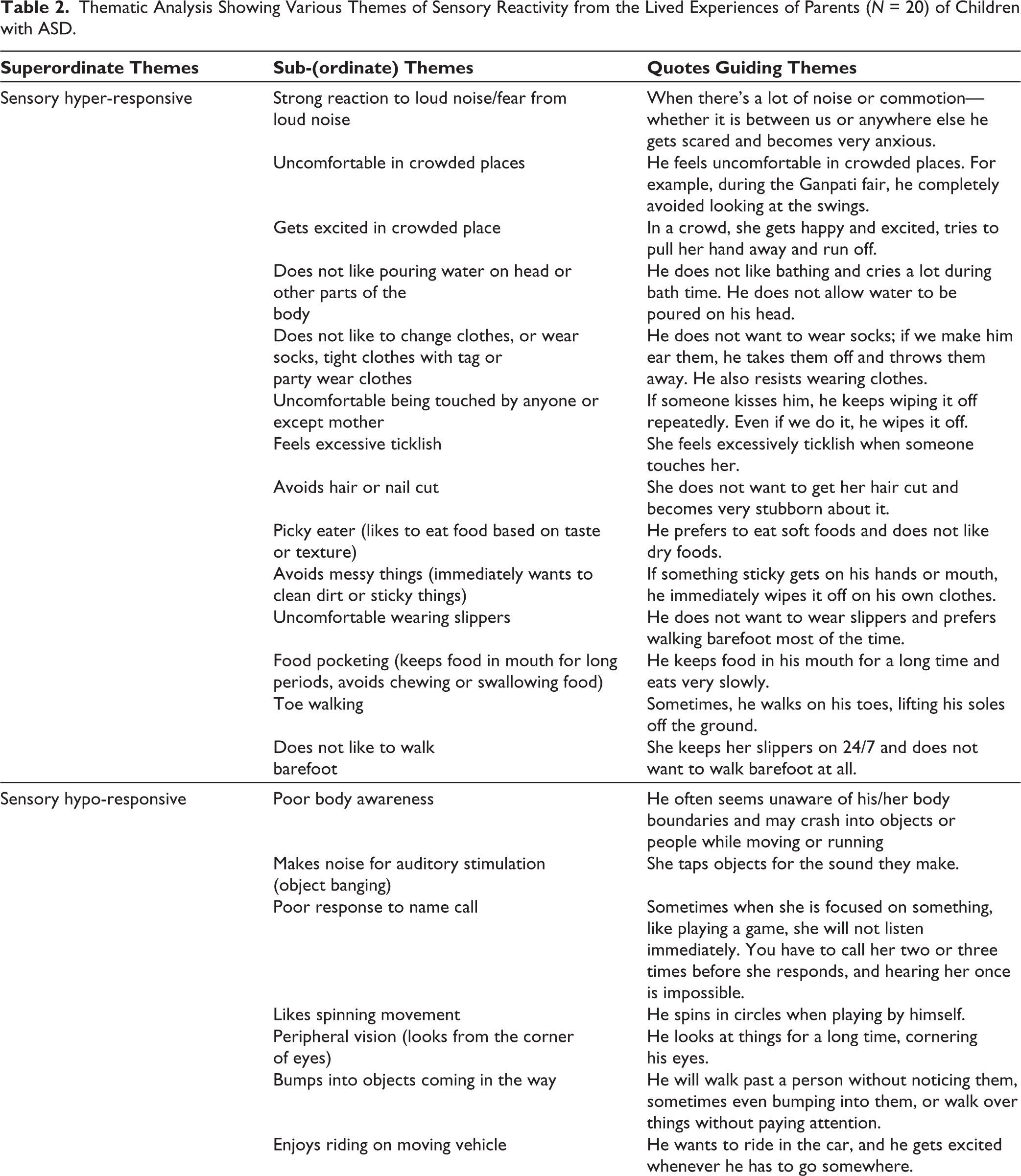
Sensory hyper-reactivity emerged as a prominent theme, where children demonstrated heightened reactions to ordinary sensory inputs. Parents frequently described intense fear or discomfort in response to loud noises (e.g., fireworks, mixer grinders), crowded places, or tactile stimuli such as pouring water on the head, cutting hair or nails, and wearing certain clothes (tight clothing, tags, or party wear). Some children displayed heightened tactile sensitivity, being overly ticklish or avoiding physical contact except with their mothers. Feeding difficulties were commonly reported, such as selective eating based on food texture, storing food in the mouth, and avoiding sticky or messy food. Other indicators of hypersensitivity included toe-walking and resistance to walking barefoot, suggesting discomfort with certain sensory experiences.
In contrast, sensory hypo-reactivity reflected diminished or under-responsive behaviors. Parents observed poor sitting tolerance, weak responses to name calls, and frequent engagement in auditory stimulation through object banging. Many children actively sought vestibular input through spinning movements, using peripheral vision, bumping into obstacles, or enjoying rides in moving vehicles, indicating lowered sensory awareness or integration.
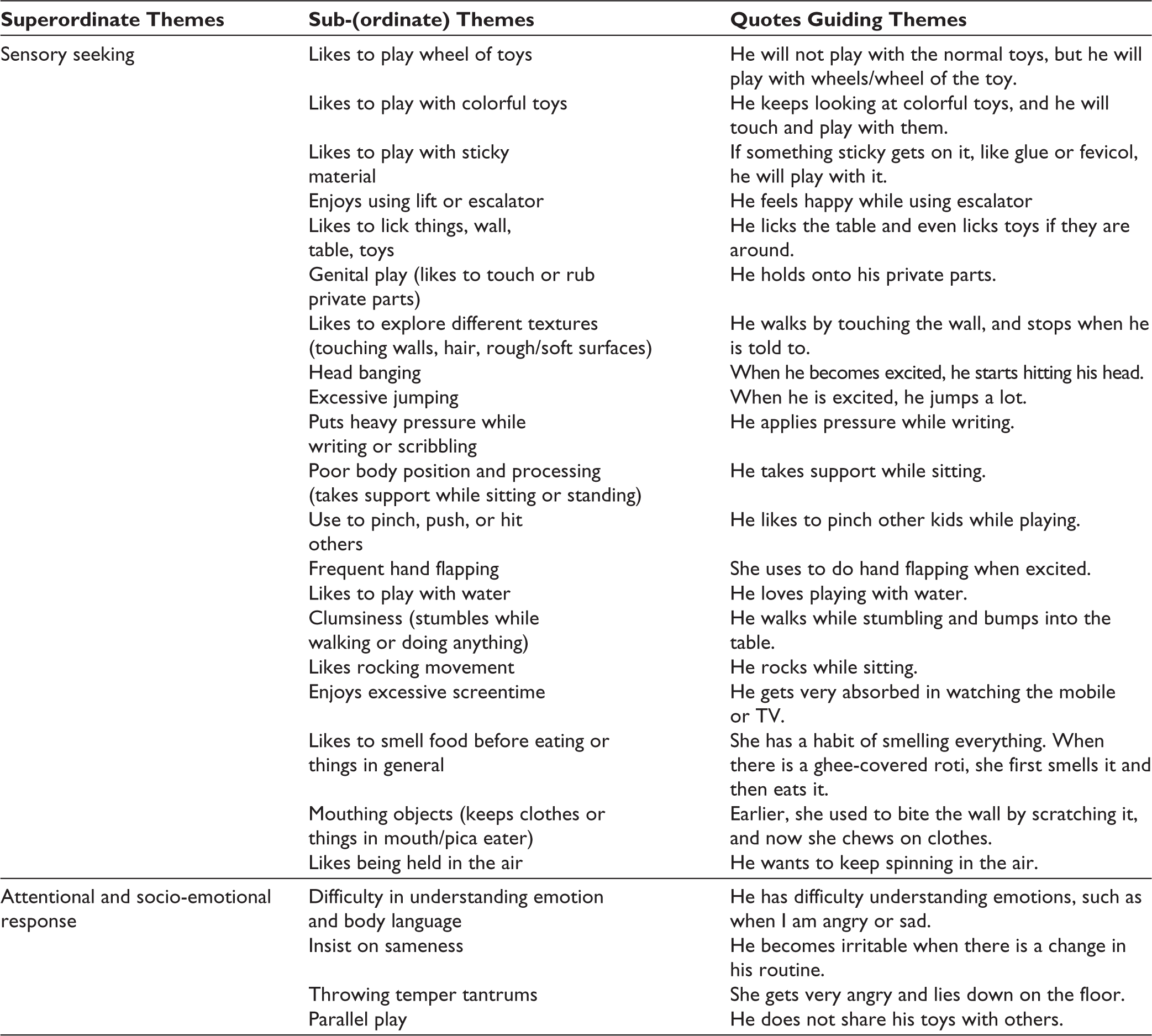
The third theme, sensory seeking, encompassed behaviors characterized by the active pursuit of sensory stimulation. Children were described as fascinated by spinning wheels, colorful objects, and sticky materials. Many exhibited repetitive motor behaviors such as hand flapping, head banging, excessive jumping, rocking, or purposeless wandering. Sensory exploration included licking or mouthing objects, smelling food or non-food items, and touching varied textures (e.g., walls, hair, surfaces). Other behaviors included clumsiness, applying heavy pressure while writing, and insistence on being lifted or held in the air. Several parents highlighted risky or socially inappropriate behaviors, such as genital play, pinching, pushing, or hitting others.
Finally, attentional and socio-emotional responses captured difficulties in interpersonal and emotional domains. Parents noted that their children struggled to understand emotions, body language, and social cues. Many insisted on sameness and routine, displayed temper tantrums when routines were disrupted, and tended to engage in parallel play rather than interactive play with peers.
Face and Content Validation
A total of 77 items were forwarded for peer review and experts for face validation. Face validation was undertaken to ensure that the items developed for the study were clear, relevant, and appropriate or important for capturing the construct of sensory reactivity of CwASD. In this stage, the proposed items and themes/dimensions (e.g., sensory hyper-responsivity, sensory hypo-responsivity, sensory seeking, and attentional/socio-emotional response) were reviewed by a panel of 10 experts, including psychiatrists, psychologists, occupational therapists, and researchers with expertise in ASD and child development. The experts were asked to evaluate each item for clarity, comprehensibility, cultural appropriateness, and alignment with the intended construct. Additionally, five parents of CwASD were invited to provide feedback on the wording and interpretability of the items, ensuring that the language was simple, unambiguous, and reflective of real-life experiences. This dual feedback process helped identify items that were confusing, overlapping, or not representative of the constructs. Based on suggestions, minor modifications were made, such as rephrasing complex terms, clarifying examples (e.g., specifying common loud noises such as fireworks or household appliances), and ensuring that the items were contextually relevant to the Indian population. A few items that combined multiple constructs, such as crowd versus loud noise, were revised to specifically target sound sensitivity, while food-related items were reframed to emphasize avoidance of unfamiliar or unpleasant tastes. Footwear and touch-related items were clarified to highlight tactile sensitivity, and visual fixation items were reworded to reflect repetitive visual focus. Certain items, such as toe-walking, head banging, excessive screen time, enjoyment of water play, and roaming, were identified as motor or behavioral, rather than sensory in nature, and were recommended for exclusion or reclassification. Overlapping items, such as bumping into objects and body boundary unawareness, were merged to avoid redundancy. Additionally, some attentional and socio-emotional related items (e.g., eye contact, playing alone, refusal to share, irritability with routine change) were considered more aligned with core ASD features than sensory reactivity, suggesting the need for exclusion or placement under a separate domain. To enhance the precision of the developed tool, new and refined wording was provided for items related to tactile discomfort, repetitive hand movements, attraction to shiny objects, and strong sensory-seeking behaviors such as pressing or pushing.
Data Calculations
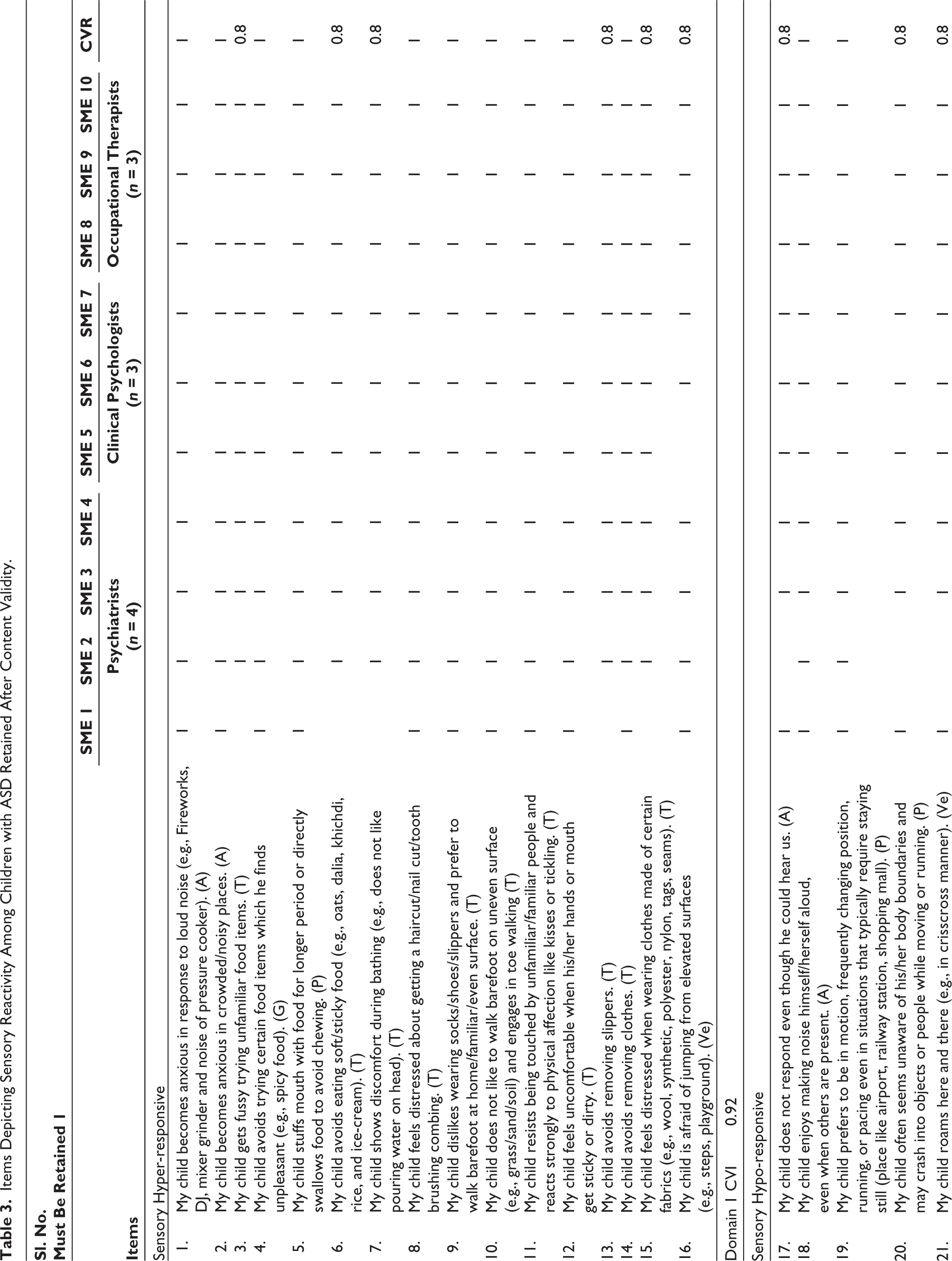
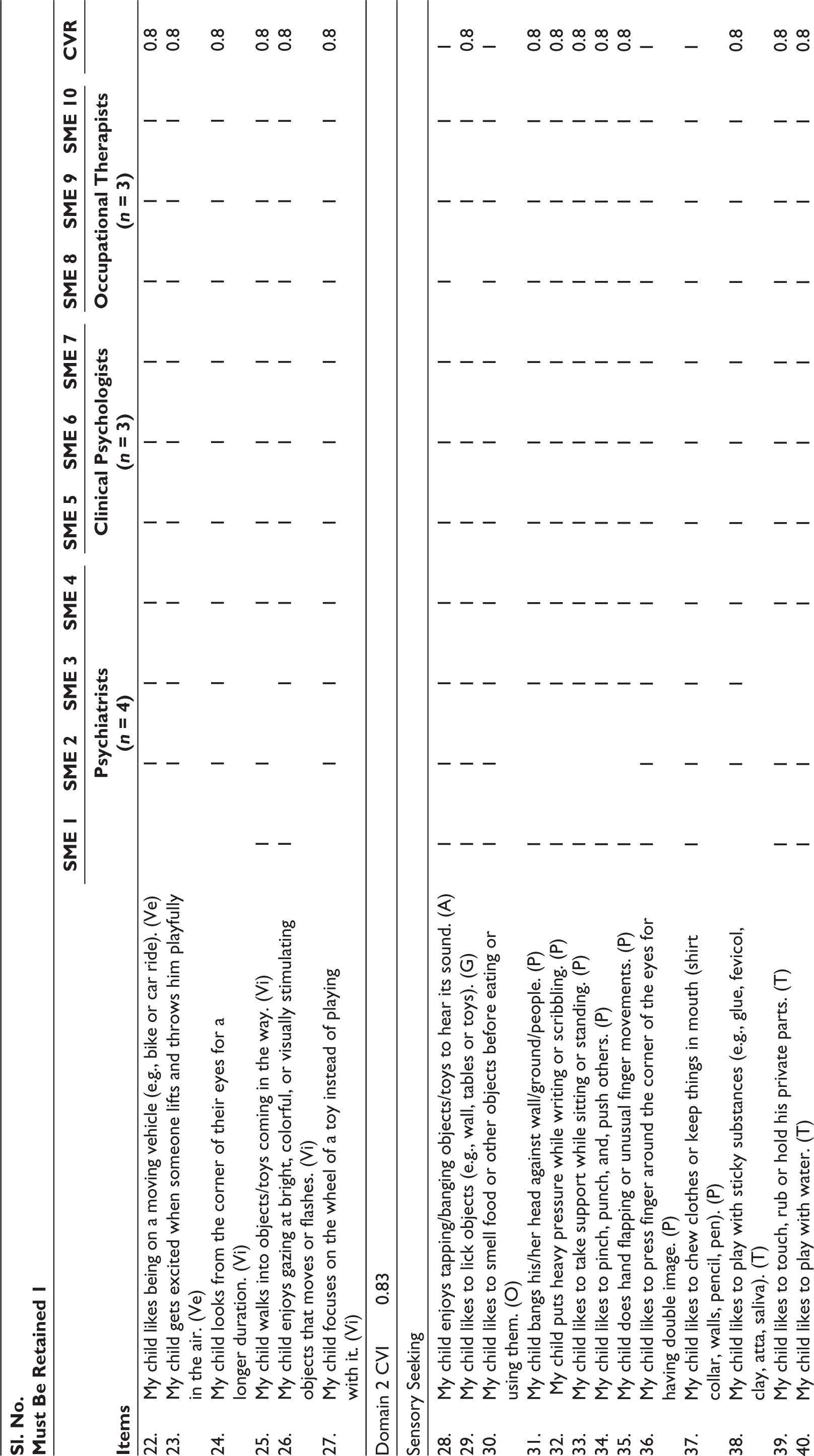
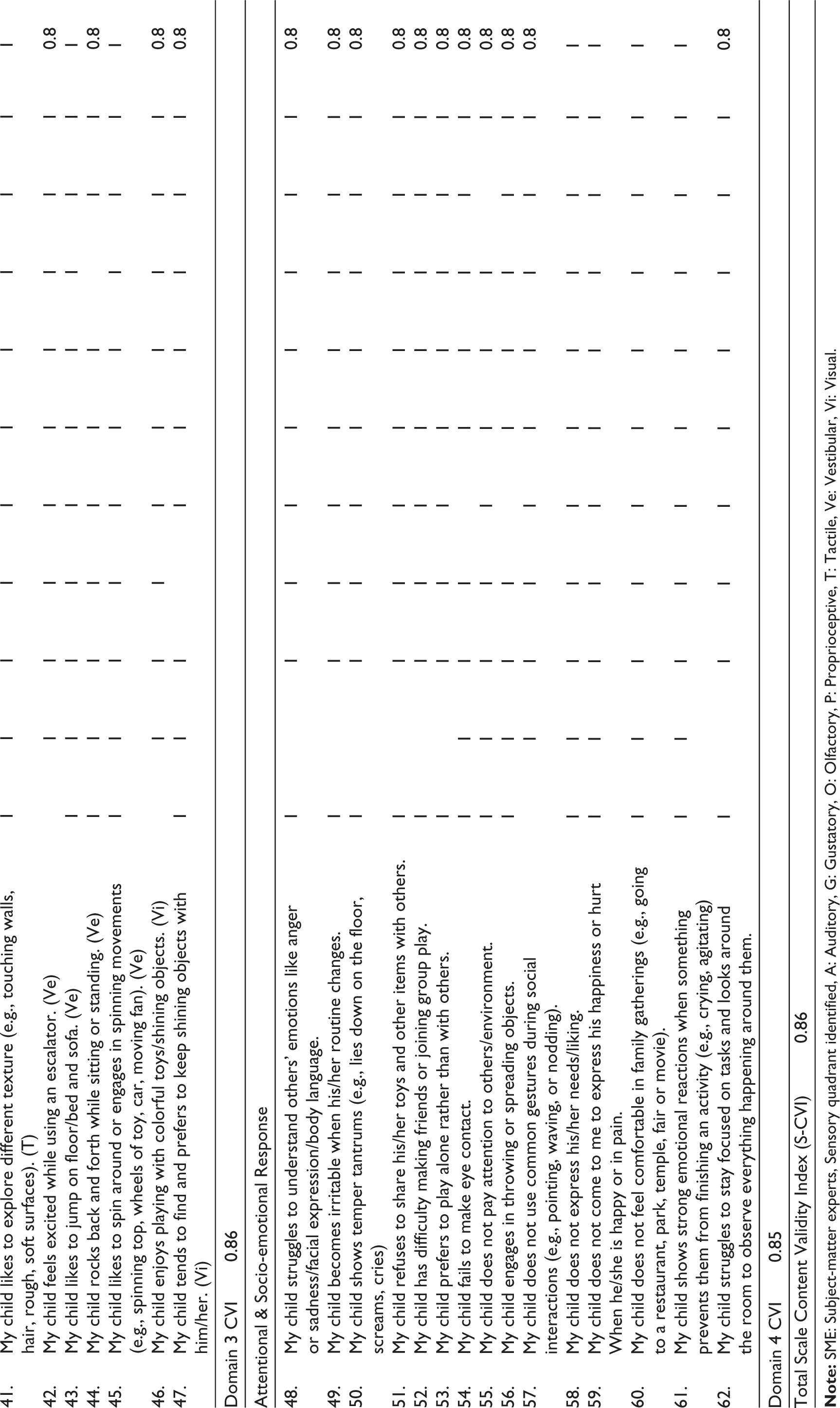
In the next two steps (CVR and CVI calculation), we used experts’ item ratings to decide about item inclusion/revision/exclusion. CVR of the items are calculated in the first round. A few items were clubbed together as they illustrated the same meaning. The content validity analysis of the scale, assessed using Lawshe’s method 19 with 10 subject-matter experts, demonstrated that the majority of items achieved high CVR values, with many receiving unanimous agreement (CVR = 1.0), indicating their essentiality. Items in the sensory hyper-responsive domain showed excellent agreement (D-CVI = 0.92), while the sensory hypo-responsive (D-CVI = 0.83), sensory seeking (D-CVI = 0.86), and attentional and socio-emotional response (CVI = 0.85) domains reflected excellent to good agreement among experts. Finally, 62 items were retained after content validation and overall, the total S-CVI for the scale was 0.86. Table 3 shows retained content validated items of sensory reactivity in CwASD.
Items Depicting Sensory Reactivity Among Children with ASD Retained After Content Validity.
Discussion
The present study describes the development and content validation of a newly developed scale assessing sensory reactivity and attentional–socio-emotional responses in CwASD. Our thematic analysis identified four interrelated sensory reactivity domains (sensory hyper-reactivity, hypo-reactivity, sensory-seeking, attentional and socio-emotional responses) that closely mirror established models of sensory atypicalities in autism and are consistent with both international and recent Indian work. Atypical sensory reactivity is widely reported in ASD, with prevalence estimates ranging widely but often very high, and neurophysiological and behavioral studies indicate multi-modal sensory differences underpinning many functional difficulties. 21
Our thematic analysis revealed sensory hyper-reactivity as the most prominent theme in a pilot study, 22 where children showed extreme reactions to everyday sensory inputs, such as disliking being touched by anyone except their mother, and avoiding messy foods. Some also showed hyper-reactivity through behaviors like toe walking or refusing to go barefoot. The intolerance to normal sounds or touch and the discomfort caused by clothing tags or dirt on clothes not only led to irritability but also restricted participation in typical social and play activities. The second theme, sensory hypo-reactivity, involved under-responsiveness, where affected children seemed less aware of sensory input. They might not respond to their name, seek strong movements like spinning or bumping into things, and show poor attention or body awareness. Sensory seeking included behaviors where children actively crave sensory stimulation. They might stare at spinning objects, engage in repetitive actions like flapping or rocking, or explore by touching or rubbing private parts (genital play), which emerged as a new theme in our study. Finally, the attentional and socio-emotional domain is related to difficulties in social understanding and emotional control. Children struggled with reading and expressing emotions, facial expressions, insisted on routines, had tantrums over change, and preferred solitary or parallel play instead of interacting with others. All these behaviors are consistent with sensory modulation difficulties, which may interfere with the child’s ability to adapt to the everyday environment. The fine-grained new subthemes in our study (e.g., getting excited in crowded places, object banging, genital play, excessive screen time, peripheral vision, fascination with shiny objects, holding objects with heavy pressure) align with item-level clusters identified in sensory profiling and echo findings from recent Indian qualitative studies that emphasize locally specific triggers and cultural contexts of caregiving. 22 Parents also reported challenges in managing these behaviors, which in turn strained family dynamics and limited opportunities for the child’s social interaction and learning.
The overlap between sensory modalities and sensory reactivity domains may occur across certain items due to the multidimensional and interconnected nature of sensory experiences in CwASD. For example, Item 24 (“My child looks from the corner of their eyes for a longer duration”) is categorized under visual hypo-reactivity because the behavior is interpreted as a compensatory response to reduced registration of typical visual input, with the child relying on peripheral vision to enhance perception. However, this behavior may also appear similar to visual sensory seeking, as the child engages in an unusual visual strategy to obtain clearer or more salient sensory information. In contrast, Item 36 (“My child likes to press finger around the corner of the eyes for having double image”) is classified as proprioceptive sensory seeking because the primary behavior involves self-generated pressure around the eyes, providing proprioceptive and tactile input. Although the resulting double vision is a visual phenomenon, the motivating sensory experience is considered to be the active seeking of proprioceptive stimulation rather than visual input itself. Thus, classification of items within the instrument is based on the predominant sensory modality and the most likely underlying sensory reactivity pattern driving the behavior.
Face and content validation were conducted to ensure that the identified themes and items accurately, clearly and comprehensively represented the construct of sensory reactivity in CwASD. It was crucial to establish its conceptual and linguistic appropriateness before proceeding to empirical testing. Face validation was conducted to confirm that the items were easily understandable, relevant, and culturally appropriate from both expert and parental perspectives. This process confirmed that the words, examples and overall structure of the items were clear and meaningful in the Indian context and reflective of real-life experiences of ASD children.
Content validation was carried out using Lawshe’s method to quantitatively assess the relevance, representativeness, and adequacy of each item. The scale demonstrated an overall S-CVI of 0.86, indicative of excellent content validity, thereby supporting the adequacy of the item pool and overall instrument. At the domain level, sensory hyper-reactivity obtained the highest CVI (0.92), indicating strong expert consensus, while sensory hypo-reactivity (0.83), sensory seeking (0.86) and attentional and socio-emotional responses (0.85) reflected good agreement. When compared with other sensory reactivity tools, the content validity of the present scale is promising and as strong as that of the Eyuboglu Sensory Reactivity Scale (ESRS), 23 which reported item-level CVI values ranging from 0.80 to 1.00 and an overall CVI of 0.94. The inclusion of socio-emotional dimensions reflects the growing recognition of the interconnectedness between sensory reactivity and social functioning in ASD. 9
Many widely used measures, such as Dunn’s sensory profile and its short form, were primarily developed based on theoretical frameworks and systematic research through clinical observation. 7 More recent instruments, such as the sensory reactivity in autism spectrum (SR-AS) 24 and the sensory perception quotient (SPQ), 25 have emphasized ecological validity by incorporating input from autistic adults and clinicians. In this respect, the present scale from India contributes to the existing literature by employing a transparent and systematic quantitative approach through content validation, involving a diverse panel of experts. This approach enhances the methodological rigor and credibility of the tool’s development process. Overall, our instrument represents an initial effort to develop a culturally relevant sensory assessment tool within the Indian context.
Taken together, the findings suggest that the present scale demonstrates excellent content validity overall, although there is always scope for refinement. Specifically, items with CVR values (0.8) may be reconsidered for clarity, cultural appropriateness, and clinical relevance. Moreover, subsequent validation studies should extend beyond content validity to include assessments of construct validity, reliability, and cross-cultural applicability. By integrating both sensory and socio-emotional domains and employing systematic content validation, the present scale addresses a critical gap in existing measurement tools and offers a promising framework for assessing sensory reactivity in children with autism. This is the first Indian developed parent-rated tools addressing sensory issues in CwASD, while existing tools are predominantly western in origin.
Our limitation includes interviewing a few single parents (four mothers) due to logistical issues; this potentially might have limited the richness and depth of the data obtained. The study sample included children aged 2–6 years; therefore, findings may not fully represent the sensory reactivity patterns of children in other age groups with ASD. Furthermore, the study was conducted in a single tertiary care hospital, which may limit the generalizability of the results to other regions. Certain culturally specific sensory triggers, such as variations in food texture and smell, exposure to festival- related stimuli, and differing noise environments in urban and rural settings, may not have been adequately captured. Our qualitative approach provides depth and novel item ideas, but cannot establish factor stability, unlike large quantitative cohort and factor-analytic studies that estimate psychometric structure.
We plan to address these limitations in subsequent studies as follows. Building on these findings, the next phase of research will focus on establishing the psychometric robustness of ISARA. This will include evaluation of reliability measures such as internal consistency and test-retest reliability, as well as construct validation through assessment of convergent and divergent validity with established standardized tools. Conducting this validation on a larger and more diverse sample will enhance the generalizability and clinical applicability of the instrument. Future translation and cultural adaptation of ISARA in the Hindi language will be undertaken, and refinement of the wording of the items will be done to improve cultural relevance, clarity and specificity in context to sensory processing difficulties in CwASD. Ultimately, a psychometrically sound and culturally relevant tool like ISARA could serve as a valuable resource for clinicians, researchers, and educators in early identification and intervention planning for CwASD and may also inform adaptations in other socio-cultural contexts across India.
Clinically, our findings support targeted, individualized sensory interventions (e.g., feeding interventions for pocketing; graded tactile desensitization for clothing avoidance). Taken together, the present work offers a culturally grounded item pool ready for further psychometric testing (e.g., factor analysis, reliability assessment) and highlights the need for mixed-methods studies that combine parent report, clinician observation, and objective sensory measures to produce robust, generalizable tools for sensory reactivity for children with ASD in Indian settings.
Conclusion
The present study successfully developed and established the content validity of the ISARA. The tool encompassed four superordinate domains that collectively capture the multifaceted nature of sensory reactivity in CwASD. The high item-level CVR and scale-level CVI scores, along with excellent domain-wise validity indices, indicate that the items are clear, relevant, and culturally appropriate for the Indian context. The findings demonstrate that ISARA is a valid and contextually sensitive instrument for assessing sensory reactivity among Indian CwASD. The present study establishes a strong foundation for the development of a culturally sensitive tool to assess sensory reactivity among Indian CwASD.
Footnotes
Acknowledgements
This study is supported by Indian Council of Medical Research, Government of India (ICMR Grant-File No. GRANTATHON2/MH-13/2023-NCD-II; 2022-17781) and the training grant “Psychiatric Research Infrastructure for Intervention and Implementation in India (PRIIIA)” (D43 TW009114, HMSC File No 2019-7623 dated January 6, 2020, funded by Fogarty International Center, NIH). The authors sincerely thank Kapil Dev Kumar and Rimjhim Rani, Occupational Therapists at AIIMS Patna, for their immense contribution to the current project work. They are also grateful to Dr. Smita N. Deshpande, Dr. Rajshekhar Bipeta and Dr. Pankaj Kumar for their valuable mentorship; Dr. Ashoo Grover, Dr. Neha Dahiya, Dr. Ravinder Singh, and Dr. Harpreet Singh from ICMR for their support and guidance; and Professor V. L. Nimgaonkar, Dr. Mary Hawk, Dr. Triptish Bhatia, and the PRIIIA faculty for their academic inputs. The authors further acknowledge Dr. Naveen Raj, Speech-Language Pathologist, other mental health experts who contributed to the face and content validation of ISARA, and the project staff members of the Department of Psychiatry, AIIMS Patna, for their valuable assistance.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for the research from Indian council of medical research, Government of India (ICMR Grant-File No. GRANTATHON2/MH-13/2023-NCD-II; 2022-17781) and the training “Psychiatric Research Infrastructure for Intervention and Implementation in India (PRIIIA).”
Informed Consent and Ethical Approval
Institute ethics committee approval: Ethical approval for this work was obtained from our institute ethics committee (AIIMS /Pat/IEC/2022/1022). The authors certify that they had obtained written informed consent from the parents and verbal assent from children with ASD. The participant’s name and initials were not published, and due efforts were made to conceal their identity.