
Abstract
Introduction
Atomoxetine, a selective norepinephrine reuptake inhibitor, is commonly prescribed for the treatment of attention-deficit/hyperactivity disorder (ADHD). Although it is generally safe, rare psychiatric adverse effects, including mania, have been reported. 1 Psychogenic polydipsia is described in adults with mania,2-4 but no reports linked to atomoxetine. We present a rare case of atomoxetine-induced mania with polydipsia in a child.
Case Report
An 11-year-old boy, born of a non-consanguineous marriage via emergency cesarean section due to meconium-stained liquor, presented with excessive water intake and hyperactivity.
His temperament was slow to warm up; he was physically developing within normal limits, with a height of 140 cm at the 25-50th percentile, and a weight of 28.38 kg at the 10-25th percentile.
At 2 months, was diagnosed with a left duplex pelvicalyceal system with Grade 3 vesicoureteral reflux (VUR) and vesicular diverticulum after urinary tract infection and remained stable thereafter.
He was diagnosed cross-sectionally at 10 years of age with a disorder of intellectual development, mild ADHD, and chronic motor tic disorder as per the International Classification of Diseases, 11th Revision criteria, by a child and adolescent psychiatrist in the Department of Psychiatry at a tertiary care hospital based on clinical interview and observation.
Clonidine was initiated for ADHD and titrated to 175 mcg/day (≈0.006 mg/kg/day) over 3 months, with partial improvement. Due to persistence of symptoms, atomoxetine was added at 10 mg/day (≈0.37 mg/kg/day) and increased to 20 mg/day (≈0.74 mg/kg/day), following which approximately 50% improvement was observed over 2 months. To achieve further benefit, the dose increased to 25 mg/day (≈0.93 mg/kg/day).
Three weeks after dose escalation, he developed manic symptoms such as elated mood, irritability, reduced need for sleep, disinhibition, overfamiliarity, hugging, and reduced regard for social boundaries. There was a new onset of demanding behavior for toys and the phone. There were polydipsia and polyuria. Twenty-four-hour input-output was 6.6/4.3 mL/kg/hour.
Investigations revealed low serum osmolality (263 mosmol/kg H2O) and low urine osmolality (57 mosmol/kg H2O), indicating dilute urine. Routine urine, microscopy, serum sodium, potassium, chloride, calcium, magnesium, glucose levels, and ultrasound KUB were unremarkable. Micturating cystourethrogram was suggestive of persistent Grade 2 VUR, and dimercaptosuccinic acid scan showed an old upper pole scar with no active disease.
Water restriction improved urine output and osmolality, ruling out diabetes insipidus and supporting psychogenic polydipsia. Atomoxetine was discontinued, was admitted, and a pediatrician and pediatric nephrologist were consulted.
At admission, he had increased psychomotor activity, elated affect, irritability, overfamiliarity, reduced need for sleep, impaired social boundaries, with no psychotic symptoms. Risperidone was initiated at 0.5 mg/day and titrated to 2 mg/day over 6 days. Polydipsia resolved within 3 weeks, with normalization of fluid intake on serial input-output monitoring.
Manic symptoms such as elated mood and irritability subsided; however, subsyndromal features, including residual disinhibition and activity levels above baseline, persisted for approximately 4 months while on risperidone 2 mg/ day. During this phase, he remained more active than baseline, with occasional disinhibited social behavior, though affect was euthymic and sleep normalized. These symptoms were monitored clinically and gradually improved without further dose escalation. ADHD symptoms were managed with continued clonidine at 175 mcg/day, with approximately 60% improvement from baseline.
Discussion
This case highlights two key findings: Atomoxetine can precipitate mania, a rare but important effect in children with neurodevelopmental conditions, and polydipsia may occur as an adverse effect of atomoxetine. The temporal sequence, with emergence 3 weeks after dose escalation and resolution on discontinuation, suggests a probable dose-dependent reaction. The Naranjo adverse drug reaction score was five, indicating a probable adverse drug reaction to atomoxetine.
Proposed Mechanism of Atomoxetine-induced Polydipsia
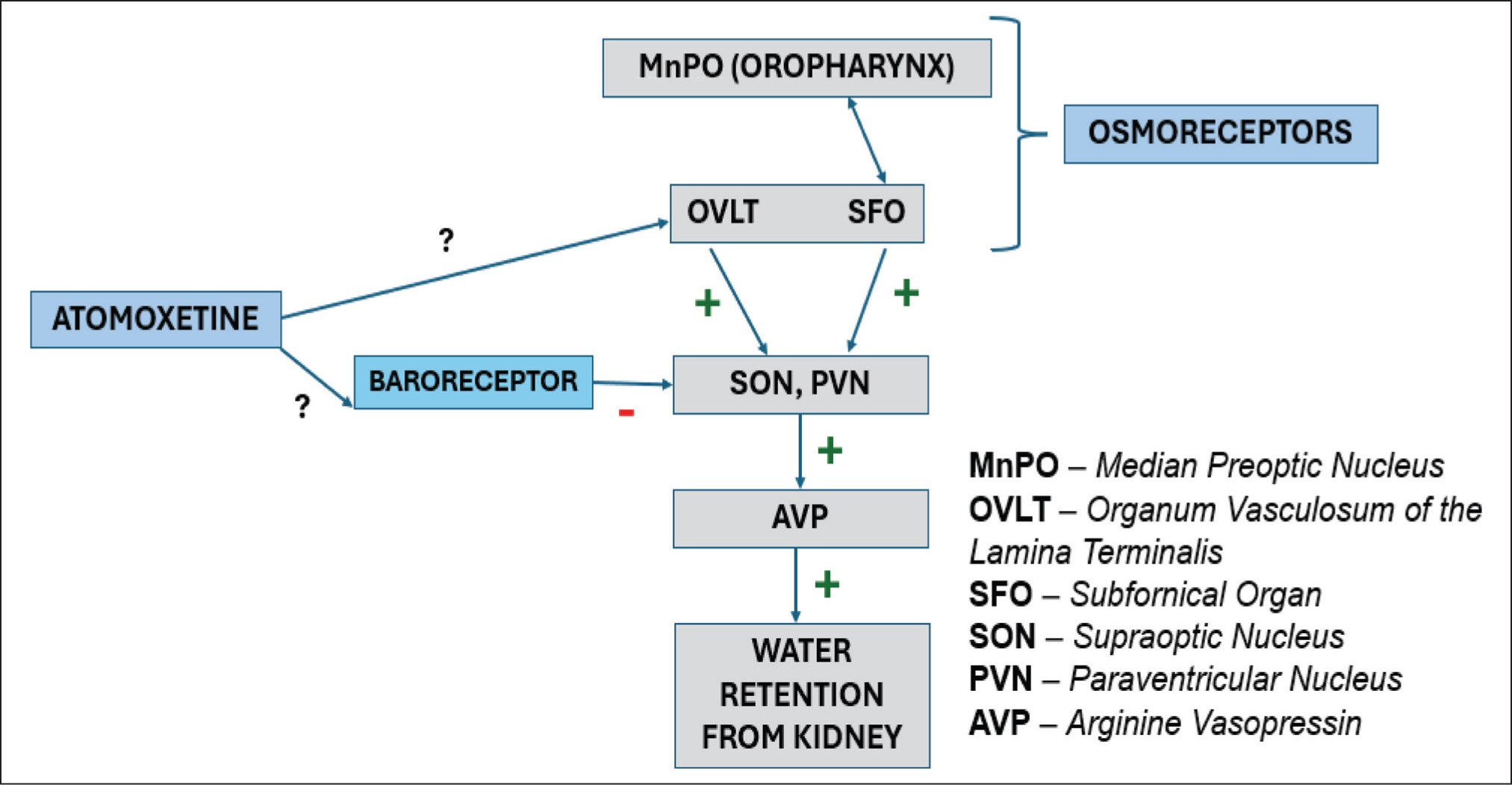
Water homeostasis is influenced by the osmolarity of blood (via thirst centers [OVLT, MnPO, SFO]) and volume of blood (via peripheral baroreceptors in the aortic arch), which influence AVP release (via neurons of PVN/SON) and water retention (Figure 1). 5 While the thirst center stimulates AVP secretion, an increase in baroreceptor tone via norepinephrine inhibits AVP secretion. 6 The mechanism of atomoxetine-induced polydipsia is not clear. Atomoxetine increases synaptic catecholamines. However, atomoxetine may directly influence the thirst center or may influence the baroreceptor signaling (Figure 1).
Mechanism of Atomoxetine-Induced Polydipsia.
Mania is associated with polydipsia. However, the mechanisms are unknown. Chronic psychiatric conditions (mainly psychosis) are posited to influence water homeostasis via multiple mechanisms, namely, thirst regulation, lowering the osmotic threshold for vasopressin release, and enhancing the sensitivity of renal receptors to AVP. 6 Catecholamine-driven AVP dysregulation and mania-associated polydipsia may account for atomoxetine-related polydipsia in our case.
Conclusion
Atomoxetine may induce mania and contribute to polydipsia in children. Early recognition and drug withdrawal can prevent complications.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The caregiver consented to publication of clinical information. Patient identity will be protected. Ethical approval was obtained from the Department’s Scientific Review Committee.