
Abstract
This article describes a case of severe hyperleukocytosis in a preterm infant with fetal inflammatory response syndrome (FIRS) associated with funisitis of umbilical cord and intrauterine inflammation. FIRS is a cause of leukocytosis in newborn, as well as leukemoid reaction in 21 trisomy, congenital leukemia, sepsis, and steroid prophylaxis. Inflammatory response syndrome is associated with high mortality, developmental impairment and complications of prematurity like intraventricular hemorrhage, chronic lung disease, periventricular leukomalacia, and sepsis.
Keywords
A baby was born early preterm (at 29 weeks 4 days gestation) from spontaneous birth, after pregnancy insurgent by medically assisted heterologic procreation. Prenatal blood tests were negative for chromosomal abnormalities. Prenatal ultrasound investigations were normal. The course of pregnancy was physiological until the onset of fever 2 weeks before childbirth. Hence, for risk of preterm birth the mother was hospitalized, and an incomplete steroidal prophylaxis was administered, due to unstoppable labor. Mother was feverish during labor, for which complete intrapartum antibiotic prophylaxis was carried out.
At birth the amniotic fluid was clear, but smelly. Maternal blood exams showed neutrophil leukocytosis (GB 28.790/mmc N 27.640/mmc) and increased inflammation indexes (polymerase chain reaction [PCR] 107 mg/L). The maternal vagino-rectal swab for Streptococcus Agalactiae was negative.
At birth, for presence of inadequate crying and bradycardia, the newborn received neonatal resuscitation by positive pressure ventilation for about 3 minutes. At the appearance of spontaneous breathing, for persistence of respiratory distress, support via nasal-C-PAP was continued until the fourth day of life.
Apgar index was 5-8-8 at 1, 5, and 10 minutes, respectively. No dysmorphic features were seen.
Blood analysis from umbilical artery was not significant for perinatal asphyxia (pH 7,37, pCO2 40 mmHg, HCO3: 23,6 mmol/L, BE: −1,5 mmol/L, Lac: 3,12 mmol/L).
Blood exams at entrance in the neonatal intensive care unit, found an important leukocytosis (GB 69.000/mmc, N 17.960/mmc L 4.140/mmc, M 4.140/mmc, E 1.380/mmc, and B 1.380/mmc), despite normal hemoglobin (12 g/dL) and platelets (300.000/mmc) values. The PCR was 23 mg/L. Furthermore, an antibiotic therapy with ampicillin and gentamycin was administered, followed by cefotaxime for the total duration of 21 days. Blood cultures were negative.
At 48 h of life, blood tests showed hyperleukocytosis (GB 180.000/mmc, N 103.000/mmc), without changes in hemoglobin and platelets, slight increase in PCR values (29 mg/L). Lactate dehydrogenase was 1.127 U/L (normal values: 934-2150 UI/L). At peripheral smear, the finding of 30% of metamyelocytes, promyelocytes, myelocytes, with absence of blasts allowed to exclude neonatal leukemia. Cancel “Blood culure was negative.” The search for cytomegalovirus in urine was negative. Neonatal karyotype was regular.
The thyme-chest ratio, measured by ultrasounds, was found to be 0,11 (normal values: 0,44-0,47) confirming a small thyme for gestational age.
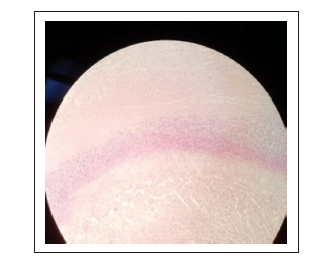
On the fifth day, the histopathological documentation of funisitis (Figure 1) as well as the finding of necrotizing vasculitis in umbilical cord (Figure 2) confirmed the diagnostic suspicion (based on the maternal history) of “Triple I” (intrauterine inflammation, infection, or both). Leukocytosis and thymic hypoplasia were therefore associated with a fetal inflammatory response syndrome (FIRS).

In third day of life, the brain ultrasounds found intraventricular hemorrhage of grade II according to Volpe’s classification (0,6 × 1 cm), in the presence of bilateral periventricular hyper-echogenicity, stable, and then resolved at subsequent ultrasound monitoring.
On the ninth day, a worsening of ventilatory conditions required again respiratory support via high-flow nasal-cannulas. Meanwhile, the chest radiography, that in third day of life had a good expansion of the lung fields, showed parenchymal opacification. Oxygen therapy was continued until 31 weeks of postmenstrual age (PMA) and ventilatory support continued until 32 weeks of PMA.
Regarding leukocytosis, there was a gradual normalization: on the seventh day of life, GB equal to 76.000/mmc and 14 days equal to 14.000/mmc.
Broncho-reactivity and increased susceptibility to infections remained. Thyme dimension normalized within first year of life.
Discussion
Physiologically at the time of birth, and in greater measure in the preterm, there is an elevation of leucocytes and neutrophils, which reach a peak in the first 24 h of life: at that age leukocytosis appears for values greater than 30.000/mmc. 1 2 A condition of hyperleukocytosis is defined by a white blood cell count >100.000/mmc.
A leukemoid reaction, which has a prevalence of 3% to 15% in neonatal intensive care, is characterized by a leukocytosis >50.000/mmc or neutrophils count >10 DS in relation to age with peripheral smear which shows a significant increase of neutrophil precursors in the absence of blasts. 3
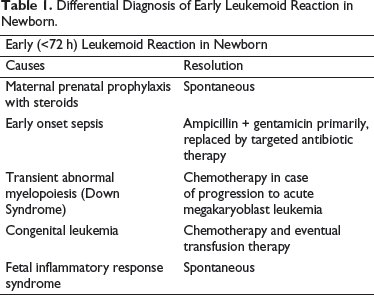
Most common causes of leukemoid reaction in the newborn in the first hours of life (<72 h) are represented by (Table 1):
Antenatal administration of betamethasone: leukocytosis in this case is particularly strong up to 3 days of life and occurs mainly in the preterm infant <32 weeks of gestational age, in which steroid prophylaxis is usually used to accelerate lung maturation and surfactant production.
4
Infections (early onset sepsis): early sepsis, within the first 72 h of life, can cause leukocytosis and hyperleukocytosis.
5
The therapy of choice in this case is represented by the association of penicillin/ampicillin and aminoglycoside as first line, replaced by antibiotic therapy targeted according to the results of hemoculture, for 10 total days in case of sepsis and 21 in case of meningeal involvement.
6
Leukemoid reaction in Down Syndrome: patients with 21 trisomy have an increased risk of acute lymphoblastic leukemia and acute myeloid leukemia. They can develop a transient abnormal myelopoiesis (TAM) that presents as leukemoid and thrombocytosis reactions: 10% of TAM progress within 4 years of life to acute megakaryoblast leukemia.
7
Most cases of TAM resolve spontaneously, while infants with hyperleukocytosis, fetal hydrops, disseminated intravascular coagulation, kidney, liver, and heart failure may benefit from chemotherapy treatment.
7
Congenital leukemia: rare forms of leukemia that appear in the first month of life are usually characterized by leukocytosis, hepatosplenomegaly, meningoencephalitis, and skin manifestations (“Blueberry Muffin Spots”). In this case, blasts appear in the peripheral blood and in the bone marrow aspirated.
8
Treatment is based on supportive transfusion therapy and chemotherapy. FIRS: FIRS secondary to condition of chorioamnionitis (current Triple I confirmed).
9
Differential Diagnosis of Early Leukemoid Reaction in Newborn.
What Is FIRS
FIRS describes a condition characterized by systemic activation of the fetal immune system with multiorgan involvement as a result of an intrauterine inflammatory process and it is associated with a high risk of morbidity in the neonatal period. 10 It can present in preterm infants with intact membranes, with early membrane rupture and also in intrauterine infections of viral origin (especially cytomegalovirus).
Chorioamnionitis, FIRS, and early onset sepsis represent a continuum in which each of them is a necessary but not sufficient condition for the onset of the other. Ascending intrauterine infection/inflammation is one of the two main pathological processes related to preterm birth.
It begins at the level of chorion, deciduous, and can eventually lead to the involvement of the fetus. Acute inflammation from neutrophil infiltration can propagate to the umbilical cord resulting in funisitis, where histological examination shows the presence of necrotizing vasculitis, as happened in our case. Funisitis is known to be the histological marker of FIRS; both funisitis and FIRS can determine early onset sepsis. 10
The diagnosis of FIRS is based on the histopathological record of chorioamnionitis (Triple I confirmed) with funisitis and/or levels of IL-6 in the cord blood >11 pg/mL. 11 High maternal inflammation indexes (PCRs) before, during, and after childbirth correlate with an increased incidence of FIRS. 12
In the fetal period, the gold standard for diagnosis is represented by invasive procedures such as amniocentesis and cordonocentesis through the measurement of intra-amniotic or cordial concentrations of cytokines (es IL-6), while postnatal diagnosis of FIRS is established through the histology of amniotic and fetal membranes.
To avoid complications arising from invasive prenatal procedures, ultrasound methods are currently being evaluated to identify fetuses with FIRS. Among these, the measurement of thyme seems to be promising: a small fetal thyme could constitute a reliable marker of FIRS. Thymic hypoplasia appears to be secondary to the migration of lymphocytes into the affected organs, and to the activation of hypothalamic-pituitary-adrenal axis in response to acute inflammation, with secondary thymocytes apoptosis at high levels of endogenous cortisol. 13 According to the antenatal data, Di Naro et al, 14 found that all preterm infants with intact membranes, with histological finding of funisitis, and affected by FIRS, had, as in our case, a small thyme after birth.
Infants who develop FIRS in uterus have an increased risk of adverse outcomes such as sepsis, early and late onset, intraventricular hemorrhages, retinopathy, periventricular leukomalacia, and pulmonary bronchodysplasia. 15 They frequently present acute respiratory distress, easily remittent, due to cascade of interleukins inducing the production of surfactant; then bronchodysplasia can develop because inflammation causes alveolar development arrest. The heart (diastolic dysfunction resulting in reduced range and secondary hypoxic-ischemic brain damage), kidney, skin, and adrenal glands can also be involved.
Francis et al, 16 in an observational prospective study that compared infant outcomes (EGs between 26 and 34 weeks) with FIRS infants matched for gestational age without FIRS, found that the former had a significantly higher risk of hypotensive shock at birth, motor development impairment and cerebral palsy.
Hyperleukocytosis in FIRS resolves spontaneously with normalization of values from 5 to 15 days.
In conclusion, in the newborn, leukemoid reaction due to FIRS must be discerned by sepsis, congenital leukemia, and 21 trisomy. An early identification of newborns developing FIRS in uterus is important to initiate proper clinical monitoring and to identify clinical manifestations of the neonatal syndrome.
Footnotes
Authors’ Contributions:
Conceptualization: ST, LC, FM; Resources: LC, CR, IB, SZ, GP; Writing: original draft preparation: ST, SV, FM, AS.
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Human and Animal Right
All persons gave their informed consent prior to their inclusion in the study.