
Abstract
Introduction:
World Health Organization (WHO) in 2014 recommended delayed cord clamping (DCC) in all babies who cry immediately after birth. Despite many benefits, there are concerns of increased rate of phototherapy in babies receiving DCC. This study was done to determine the increment in the rate of phototherapy required in infants managed with DCC vs infants managed with early cord clamping (ECC).
Methods:
A retrospective observational study was conducted in a tertiary care hospital in Pune, India. All the infants born between January 2018 and July 2018, for whom ECC was done, were compared with infants who were born between January 2019 and July 2019, after DCC policy was adopted. All the infants with birth weight ≥2 kg and gestation ≥35 weeks, who were with their mother, were included. Baseline characteristics were compared for both the groups. American Academy of Pediatrics guidelines for treatment of neonatal jaundice were used to determine the need for phototherapy. Number of infants in both the groups who required phototherapy were compared.
Results:
The ECC group had 565 infants while DCC group had 731 infants. There was no difference in the baseline characteristics of the 2 groups. Jaundice requiring phototherapy was noted in 31% of infants in the ECC group, compared to 45% in infants in the DCC group (relative risk: 1.47 [1.27-1.71] [P < .001]).
Conclusion:
In this study, DCC increased the need for phototherapy by 47% in late preterm and term infants. Randomized control trials with larger sample size are required to confirm this finding.
Introduction
Cord clamping is the procedure of occluding the cord after delivering a baby, so that it can be cut to facilitate separation from placenta. Practice of early cord clamping (ECC) was adopted as a matter of convenience, without any supporting evidence. It came in vogue in 1960s, as it was thought to reduce maternal postpartum hemorrhage. 1 However, review suggested that only the uterotonic drug might account for this effect and ECC did not have any additional benefit. 2 What constitutes a delay in cord clamping has always been a controversy. According to World Health Organization (WHO) guidelines, 3 delayed cord clamping (DCC) implies clamping the cord after 60 s or when the umbilical cord pulsations have ceased.
Despite multiple benefits like placental transfusion leading to higher hemoglobin levels and decreased iron deficiency, there have always been concerns about adverse effects of DCC. These include polycythemia and hyperbilirubinemia requiring phototherapy. 4 This study was planned to determine the increment in the rates of hyperbilirubinemia requiring phototherapy in infants who received DCC as compared to ECC. In resource poor settings, the avenues to diagnose and treat hyperbilirubinemia may be scarce and processes to diagnose and treat hyperbilirubinemia may have to be reviewed for effectiveness.
Methods
A retrospective study was conducted in a tertiary level neonatal intensive care unit (NICU) of Pune, India. DCC policy was adopted in August 2018. Five months washout period was kept. During DCC, infants were kept at the level of abdomen during vaginal delivery and just above abdomen on the thighs during caesarean section. DCC was ensured by 2 persons present in delivery room—pediatrician and assisting sister. Time for DCC was noted in the initial assessment sheet of the infant. Following the adoption of DCC policy, data from infants receiving DCC (January 2019 to July 2019) was compared to a period of 7 months in the previous year when ECC was in practice. Consent was not taken, as DCC was considered as standard practice. All infants with gestational age >=35 weeks, birth weight >= 2 kgs, who were hemodynamically stable, in room air and taking full feeds, were analyzed. Infants with any major congenital malformation, those who needed resuscitation, or those admitted to NICU immediately after delivery, were excluded. All infants born during the prespecified study period irrespective of the type of delivery were included. American Academy of Pediatrics guidelines for treatment of neonatal jaundice 5 were used and strictly followed to determine the need for phototherapy depending on the gestation, age in hours, and risk factors. Infants were assessed twice in the day, during morning and evening rounds. Transcutaneous bilirubinometry (TcB) using JM-100 was done in the infants who looked clinically icteric in good day light. In infants whose TcB came above the cutoff for the phototherapy range, or whose TcB came more than 15 mg/dL, serum bilirubin was tested using diazo method. Infants who were admitted to NICU for phototherapy in both the groups were compared. Data was entered in Excel sheet and results were tabulated and statistically analyzed by statistical package SPSS version 25.0. Independent t test was used to test the mean difference between the 2 group for continuous variables and chi square test was used to test the association for the categorical variables.
Results
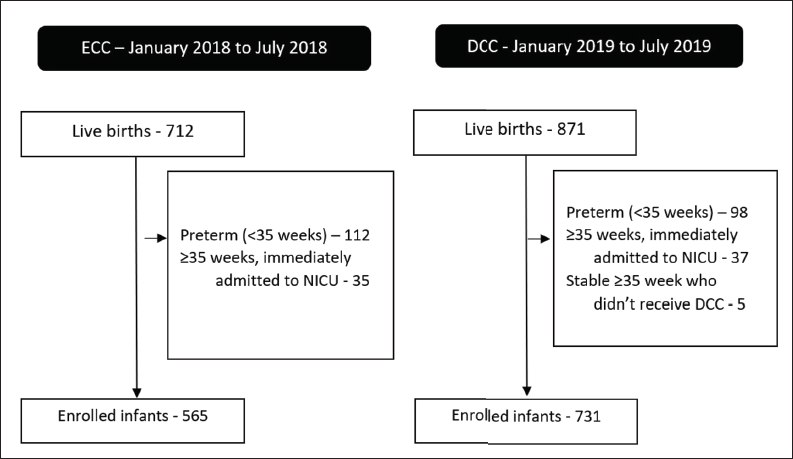
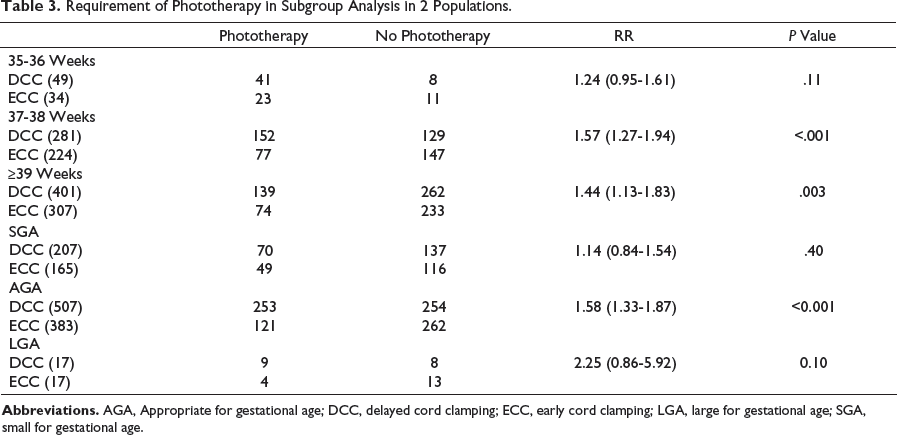
Out of total 712 live births in January 2018 to July 2018, 565 were enrolled. Whereas in January 2019 to July 2019, 731 infants received DCC and were enrolled out of the total 871 live births (Figure 1). The baseline characteristics of the 2 groups were similar (Table 1). Phototherapy for jaundice was required in 31% infants in first group, compared to 45% (P < .001) in infants born after DCC policy was adopted (Table 2). On subgroup analysis, increment in phototherapy was seen in all gestations, but in late preterm didn’t reach statistical significance (Table 3).
Patient Enrolment Flow Diagram.
Baseline Characteristics of the 2 Populations.
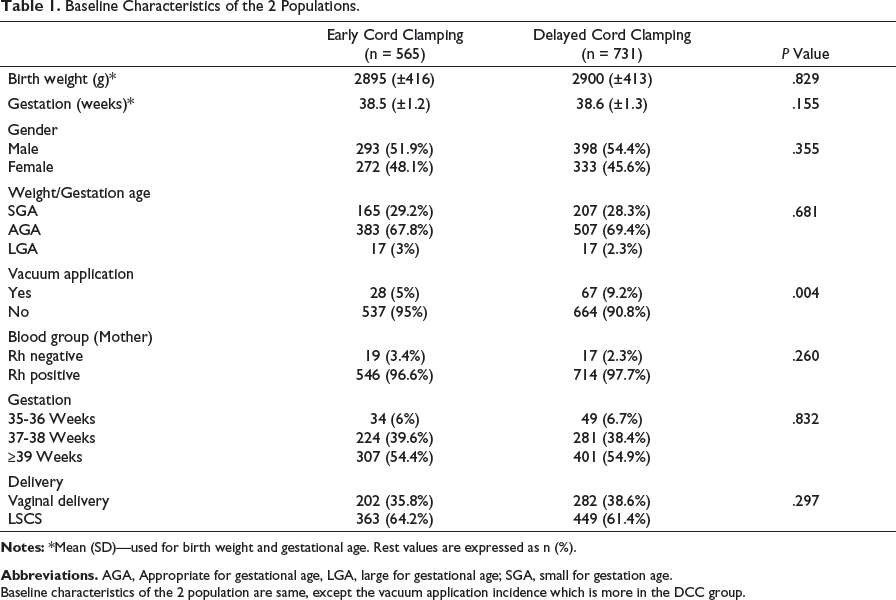
Baseline characteristics of the 2 population are same, except the vacuum application incidence which is more in the DCC group.
Requirement of Phototherapy in the 2 Populations.

Abbreviations. DCC, Delayed cord clamping; ECC, early cord clamping.
Requirement of Phototherapy in Subgroup Analysis in 2 Populations.
Discussion
In this study, a retrospective analysis was done to assess the difference in the rate of phototherapy required, before and after DCC policy was adopted. Our study showed increased need of phototherapy in infants undergoing DCC by 47%, which would ultimately result in prolonged duration of hospital stay as well as expenses for the family. Baseline characteristics of the 2 groups were similar. The number of infants requiring phototherapy (both ECC and DCC periods) is higher in our study as compared to previously documented phototherapy rates (5-15%).6, 7 This high rate of requirement of phototherapy even in infants who received ECC care may be explained by rigorous monitoring by TCB followed up with serum bilirubin. Being a referral hospital, high-risk pregnancies including Rh negative mothers and gestational diabetes are managed in the center. This might explain the high frequency of hyperbilirubinemia and phototherapy. A significant increase in number of infants requiring phototherapy was noticed, after DCC policy was followed.
Many studies and meta-analyses4, 8-10 have established the benefits of DCC, both in preterm and term infants. In a study, it was found that term infants received significant amount of blood being passed from placenta (placental transfusion), up to the volume of 81 mL (range: 50-163 mL) or 25 mL/kg (range: 16-45 mL/kg). 8 They also observed that blood transfused through DCC constitutes approximately 20% of the infant’s blood volume at birth. Similar figures have also been observed by Yao et al. 9 According to the Cochrane review, DCC not only results in higher hemoglobin level in neonatal period at 24 to 48 h (mean difference: 1.49 g/dL, 95% confidence interval [CI] 1.21-1.78; 884 infants), but also less of iron deficiency (relative risk [RR]: 2.65, 95% CI 1.04-6.73; 5 trials, 1,152 infants) at 3 to 6 months of age. 4 In preterm infants, DCC has been reported to decrease intraventricular hemorrhage, increase hematocrit, decrease the need for transfusions and inotropes, and decrease incidence of necrotizing enterocolitis.10-12
Whilst DCC has shown to be greatly beneficial, it has some adverse effects. Placental transfusion will result in more RBC load, overloading newborn’s metabolism leading to polycythemia and hyperbilirubinemia.
In a Cochrane analysis, it was concluded that difference in clinical jaundice did not reach statistical significance (RR: 0.84, 95% CI 0.66-1.07) between the 2 groups; however, fewer infants in the ECC group required phototherapy for jaundice than in the late cord clamping group (RR: 0.62, 95% CI 0.41-0.96, I 2 5%). 4 According to Rincón et al, 13 DCC increased the chances of polycythemia but there was no statistically significant difference in serum bilirubin levels and jaundice requiring phototherapy in the 2 groups. 13 In a prospective randomized controlled trial, serum bilirubin levels were compared after 72 h in the 2 groups. The mean total bilirubin level of infants in group with ECC was 2.06 mg/dL and in DCC group it was 4.92 mg/dL (P value: .003). 14 Same study also found that the mean hematocrit level was significantly higher in the DCC group with the mean of 48.67 (range: 32-71%) in comparison to the ECC group with the mean of 42.36 (range: 30-70%) with P value of .002. In our study, we have found that the increment in phototherapy is increased by 47% in DCC group as compared to ECC group. The increment is statistically significant.
On subgroup analysis—difference not reaching statistical significance in late preterm, SGA and LGA group—could be due to smaller representation of these subgroups. The strength of the study is robustness of the implementation of inclusion and exclusion criteria and the analysis of the data. We would like to conduct a prospective trial comparing the effects of DCC and ECC on requirement of phototherapy, but it will be unethical to not offer DCC given the proven benefits of DCC.
Being retrospective, the main limitation of this study is that some data could not be retrieved regarding the other possible etiologies of hyperbilirubinemia like Rh and ABO incompatibility, sepsis, cephalhematoma, dehydration status, or any other evidence of hemolysis which might explain the difference in our result. There was also difference in the rate of assisted vaginal deliveries in the 2 groups which might cause cephalhematoma and difference in the rates of hyperbilirubinemia. But due to small size, adjusted analysis could not be done for the same. As the 2 groups are demographically similar and also that the data was compared for similar duration in the same institute, we hope that it would mitigate the effects of various other etiologies of jaundice in newborn. Also, data regarding hemoglobin levels and polycythemia and patient outcomes like duration of phototherapy and hospital stay is lacking.
Conclusion
DCC significantly increased the requirement of phototherapy. It has important implication on availability of phototherapy treatment at places where DCC is standard practice. Despite increased risk of phototherapy, DCC has proven short- and long-term benefits for infants. Providing phototherapy by mother’s side will be useful in reducing the separation of mother baby duo and will be helpful in establishing breastfeeding.
Footnotes
Acknowledgment
We would like to acknowledge the technical support provided by Mr Rupeshkumar Deshmukh, for his contribution in statistics for this research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was taken from the ethics committee of the college.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.