
Abstract
Background
Sub-Saharan African countries, especially the Eastern region, present the dismal picture of neonatal mortality (NM) in the globe. The majority of these deaths could be avoided if effective health measures are provided throughout pregnancy and childbirth. Although antenatal care (ANC) is assumed as one of the viable interventions that contribute to neonatal survival, the effect of ANC on NM was not systematically analyzed in Eastern Africa. Thus, the study aimed to determine the pooled effect of ANC on NM in Eastern Africa.
Methods
PubMed, EMBASE, CINAHL, and HINARI databases were searched using appropriate keywords from January 1, 1990 to February 12, 2021. Independent authors selected eligible articles and extracted data. The risk of a bias assessment tool for nonrandomized studies was used to assess the quality of the study. Comprehensive meta-analysis version 2 was used for meta-analysis. The random-effect model was employed, and the outcome is expressed as a risk ratio with 95% confidence interval (CI).
Results
In total, 1149 studies were identified through database search, and only 27 studies were included in the meta-analysis. Having at least 1 ANC visit during pregnancy reduced the risk of neonatal death by 42% compared to their counterparts (RR = 0.58, 95% CI [0.47, 0.71]). The pooled prevalence of NM was 8.5% (95% CI [7.3, 9.6]), with NM rate of 46.3/1000 live births.
Conclusion
The study indicated that NM might be decreased even with a single ANC visit when compared to no visits. Scaling up ANC services through ANC promotion and tackling service-related barriers could potentially reduce NM in Eastern Africa.
Background
Globally, an estimated 2.5 million children died in the first month of life that accounts 7000 neonatal deaths per day.1, 2 Neonatal mortality (NM) has contributed to 47% of under-5 mortality,2, 3 and surprisingly, 80% of neonatal deaths resulted from preventable and treatable causes. 4 Although substantial progress has been made in reducing childhood mortality, 5 there is a slow decline in neonatal mortality rate (NMR). Also, there is a huge gap in newborn survival between countries of varying economic status. 5
Sub-Saharan Africa (SSA; 41%) and South Asia (38%) contributed to almost 80% of newborn deaths worldwide. 3 The NM rate, stands at 27/1000 live birth, is the highest in the globe, 6 and the region has shown a very sluggish decline in NM over the last two decades. 7 Generally, the vulnerability of neonatal death is estimated to be 10 times more as compared to developed countries. 3 Within SSA, the NM rate is unevenly distributed and the burden is unacceptably high in the Eastern African countries that accounted for almost half of the neonatal deaths. 8 This regional variation and high burden of NM in the Eastern African region are because of differences in the quality of healthcare governance and financing, low standard maternal health service, and poor socioeconomic status. 9
There has been a continuous decline in under-5 mortality worldwide; however, NM remained stagnant in many developing countries, 10 and its contribution to under-5 mortality was persistently high since the inception of the millennium development goals (31% in 1990, and 41% in 2018), especially in many SSA countries. 11 12 13
Effective and timely maternal health-care service before conception, during pregnancy and childbirth, could save nearly 3 million newborns in high-burden countries. 14 Sustainable development goals aim to reduce NM to as low as 12 deaths per 1000 live births by the year 2030. 15 However, current trends showed more than 60 countries (with the majority situated in the Eastern Africa region) might miss this target. 16 Therefore, achieving sustainable development goals requires ensuring universal access to safe, effective, high-quality, and affordable health care for women and children. 17
Antenatal care (ANC) is an ideal entry point for maternal and neonatal health-care providers to ensure access to numerous health-care interventions. 18 It is recognized as one of the fundamental strategies to reduce stillbirth and NM regardless of the socio-demographic backgrounds.19, 20 However, studies from Eastern Africa that investigated the relationship between ANC and NM have found conflicting reports as some studies found the reduced risk of neonatal death among mothers who had at least 1 ANC visit,19, 212223242526 while others did not find evidence of an association between having ANC and neonatal death. 27 28 29 30 31 32 Thus, having pooled evidence emanated from systematic review and meta-analysis is highly crucial and demanded to inform policymakers in the Eastern Africa region and to clearly understand the relationship between ANC and NM. Additionally, the magnitude of NM showed great disparities across countries in Eastern Africa at different periods ranging from 13.2% 33 to 65.6%. 32 Therefore, the primary aim of this systematic review and meta-analysis was to investigate the effect of ANC on NM in Eastern Africa. Furthermore, as a secondary aim, this review aimed to determine the pooled prevalence of ANC service utilization and NM in Eastern Africa.
Materials and Methods
The present systematic review and meta-analysis were conducted following the preferred reporting items for systematic reviews and meta-analysis guideline checklist 34 (Additional File 1 Table S1).
Search and Identification of Studies
The study search was carried out by the 2 reviewers (GT and KS). The searches were mainly focused on both published and unpublished studies/grey literature available from January 1, 1990 to February 12, 2021. We searched studies mainly from well-known databases such as PubMed, EMBASE, CINAHL, and HINARI. We also retrieved records through the CENTRAL library and Google Scholar.
The search was performed using the following medical subject headings (MeSHs) or terms: “Antenatal care,” “prenatal care,” “obstetrics,” “pregnancy care,” “maternity care,” “maternal health services,” “perinatal mortality,” “neonatal mortality,” “neonatal death,” and “newborn death” (Additional File 2 Table S2). The search terms were developed based on the population, intervention/exposure, comparator/control, and outcome.
Eligibility Criteria
The following eligibility criteria were used for studies to be included in this systematic review and meta-analysis process. Observational studies (cross-sectional, case-control, and cohort) published in the English language and had reported on the association between ANC and neonatal survival in Eastern Africa were included. Nevertheless, articles that report NM and perinatal mortality together, compared number of ANC visit to NM (without Yes/No response for ANC) were excluded from the meta-analysis. Moreover, studies emanated from review, commentary, editorials, fact sheets, and policy briefs were not included in systematic review and analysis.
Selection Process
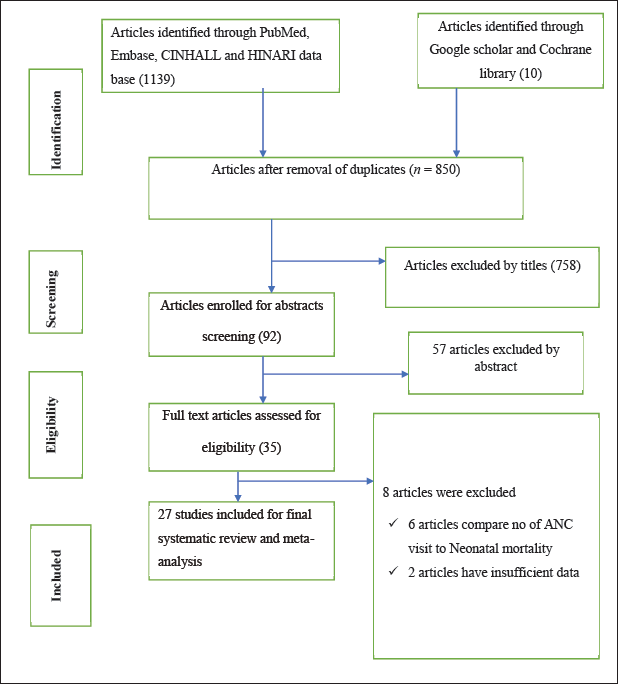
The studies' screening and selection process were carried out in 3 stages. First, studies were screened by title and abstract. The two authors (GT and YS ) screened studies based on their titles and abstracts independently. Studies that reflect the effect of ANC on NM in their title and abstract sections were included for further full-text assessment. Second, the full texts of the studies were assessed based on the predetermined inclusion criteria. The 2 authors (GT and YS) screened the studies thoroughly by reading the full text. Third, the included studies were appraised for methodological quality. Any disagreement between the 2 reviewers was resolved through discussion and common consensus. In the case of divergent ideas on the status of studies, the 3 reviewers (AM, KS, and AS) were consulted and gave final remarks on the fate of the studies. The overall selection process of the studies is recorded on the preferred reporting items for systematic reviews and meta-analysis flow diagram (Figure 1).
Flow Chart Showing the Procedure of Selecting Studies for the Systematic Review and Meta-analysis Conducted in Eastern Africa, 2021.
Methodological Quality Appraisal
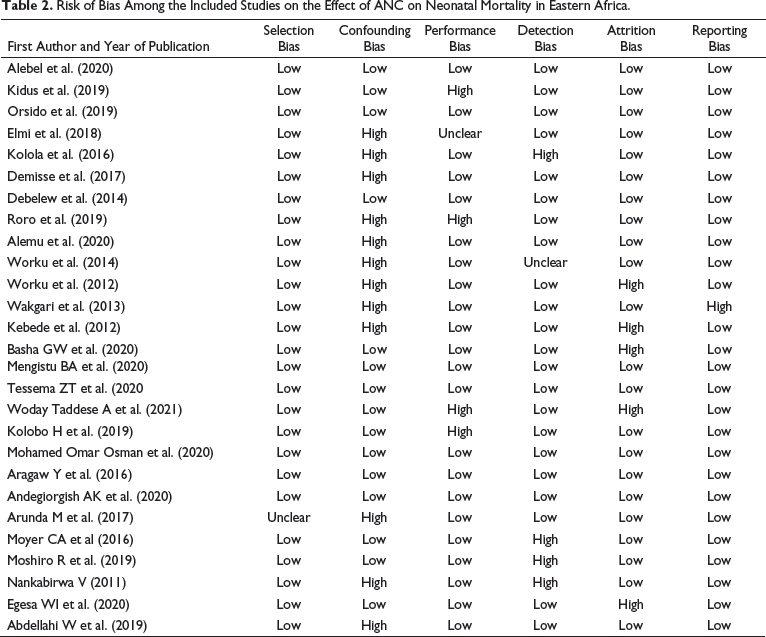
Authors rigorously assessed the quality of all the included studies using the risk of bias assessment tool for nonrandomized studies. 35 Accordingly, 5 parameters such as selection, confounding, performance, attrition, and reporting bias were used to assess the quality of the articles. The result of the bias for each parameter was rated as “low risk,” “high risk,” and “unclear” based on the assessment tool.
Measurement of Outcome and Exposure
We used NM as an outcome variable that was defined as the death of the neonate within the first 4 weeks (28 days) of life. 36 The presence and absence of ANC visits were used as an exposure variable, and an ANC service utilization in this study is defined as women having at least one ANC visit.
Data Extraction
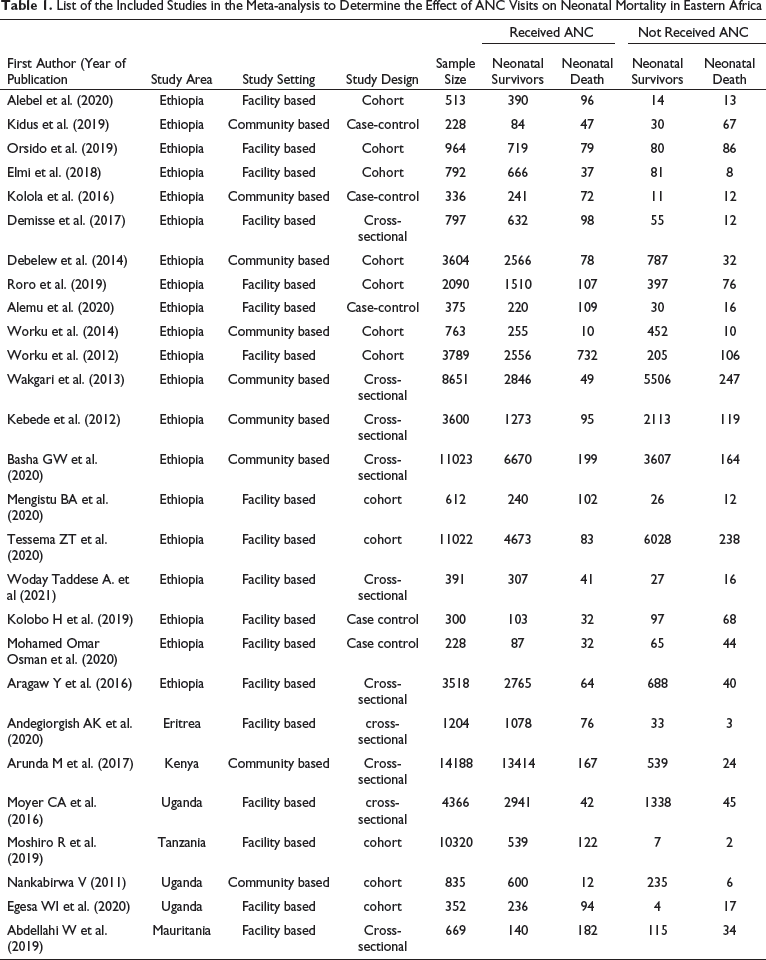
List of the Included Studies in the Meta-analysis to Determine the Effect of ANC Visits on Neonatal Mortality in Eastern Africa
Data Synthesis and Analysis
A Microsoft excel spreadsheet software was used to extract data from potentially eligible articles and then exported to comprehensive meta-analysis version 2. The random effect models were fitted to determine the pooled effect size with a 95% confidence interval (CI) to investigate the effect of maternal ANC services utilizations on neonatal death, and the pooled prevalence of NM mortality and ANC service utilization. 37 The existence of heterogeneity was assessed by the chi-square test (Cochrane Q test), and the level of heterogeneity was determined by using the I-squared statistic (I2). 38 Sensitivity analysis was conducted to assess the stability or robustness of the pooled estimates to outliers and the impact of individual studies. Furthermore, possible sources of heterogeneity were explored using subgroup analysis. Publication bias was evaluated using Egger’s test and the existence of publication bias was declared at P value < .1. 39 The pooled effect size was reported in the form of relative risk with 95% CI and P value.
Results
Study Characteristics
We identified 1149 studies, of which, 35 full texts were asse-ssed for eligibility criteria. We excluded 8 studies, 6 because of NM compared to the number of ANC visits33,40,44 and 2 due to insufficient data.45, 46 Finally, 27 original studies were included for this systematic review and meta-analysis (Figure 1).
The majority of the included studies were published in the last 5 years. We included 12 cohort-studies,21, 22, 24, 26, 28, 30, 31, 4748495051 10 cross-sectional,19, 25, 27, 29, 32, 5253545556 and 5 case-control studies.23, 57585960 The sample size of the studies is ranged from 228 to 14,188. In this systematic review and meta-analysis, 6 countries of the Eastern African region were represented (Table 1).
Risk of Bias Assessment
Risk of Bias Among the Included Studies on the Effect of ANC on Neonatal Mortality in Eastern Africa.
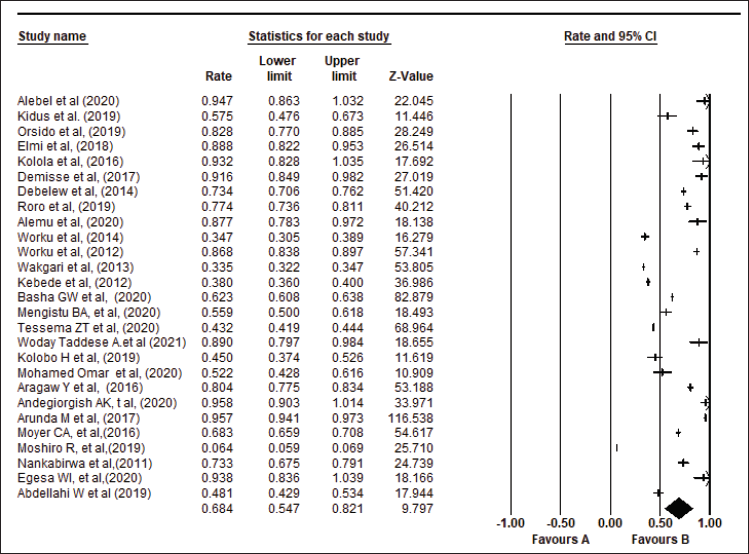
The Pooled Coverage of ANC Services
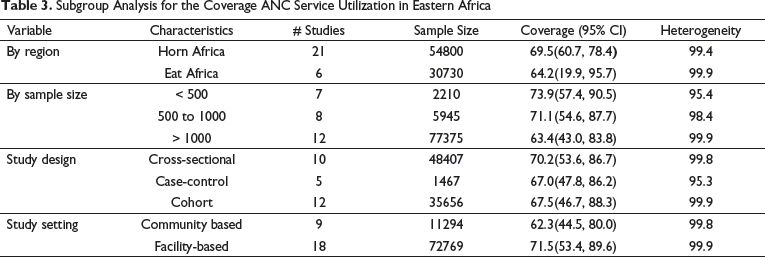
Subgroup Analysis for the Coverage ANC Service Utilization in Eastern Africa
Meta-Analysis of Overall ANC Service Utilization in Eastern Africa.
Publication bias among the included studies identified with the Egger regression test was significant for publication bias. To further rule out, trim-and-fill analysis was applied in the random-effects model. After trim-and-fill analysis, no study was trimmed to the left and right side of the mean, and publication bias was also not indicated in Begg’s test with a P value of < .06.
The Pooled Prevalence of NM in Eastern Africa
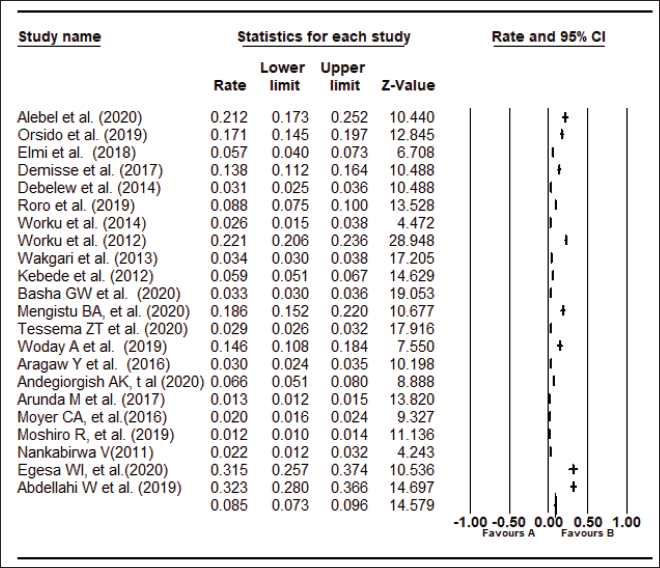
To compute the pooled prevalence of NM, 5 studies that did not report on the total population were excluded. From 83,550 live births, 3875 died within 28 days of birth, with a NM rate of 46.3 per 1000 live births, and the remaining 79,675 survived beyond the first 28 days after birth.
Based on the result of 22 eligible studies, the pooled prevalence of the NM was 8.5% (9.5% CI [7.3, 9.6]; I2 = 98.8%, P value < .01) in Eastern African region (Figure 3).
Meta-analysis of Prevalence of Neonatal Mortality in Eastern Africa.
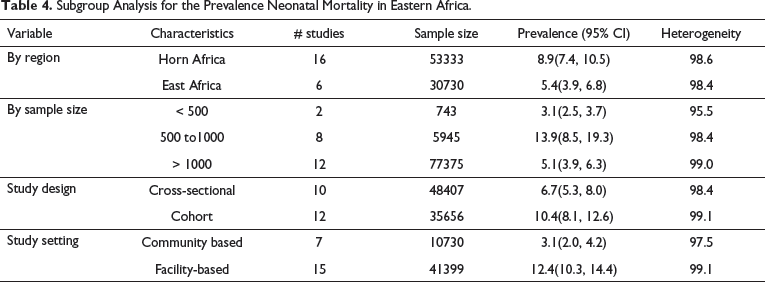
Subgroup Analysis for the Prevalence Neonatal Mortality in Eastern Africa.
Effect of ANC on Neonatal Mortality
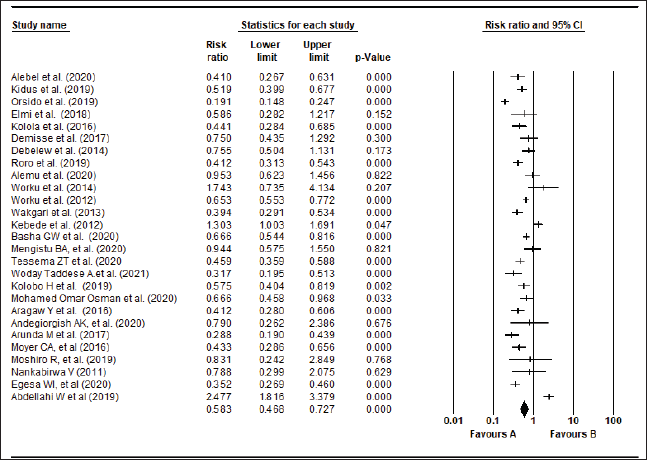
From the 27 studies included in this review, 17 studies showed that having at least 1 ANC visit was significantly associated with NM. In the random effect model, the pooled effect of ANC on NM was (RR = 0.58 [0.58 [95% CI [0.46, 0.72]]]) for neonates born to women who had at least 1 ANC visit compared to neonates born to women who had no ANC visit (Figure 4).
Meta-analysis About the Effect of ANC on Neonatal Mortality in Eastern Africa.
Studies’ Heterogeneity and Publication Bias
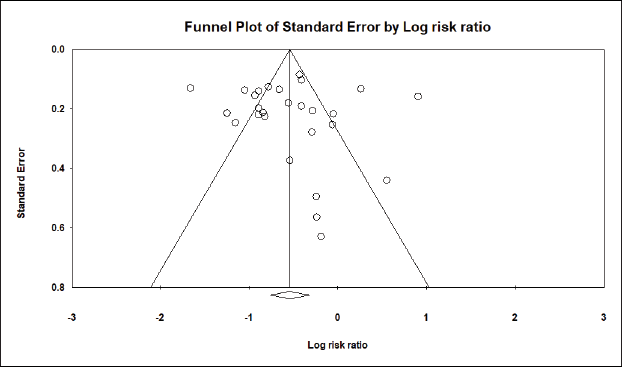
Substantial heterogeneity was found across studies included for determining the effect of ANC on NM, with I2 statistics = 89% and P value < .001. Subgroup analysis was carried out to identify sources of heterogeneity using study design, setting, study region, and sample size. Accordingly, in a subgroup analysis, heterogeneity was slightly reduced when subgrouping was done by study design, and moderate heterogeneity was detected among case-control study design (RR = 0.60 [95% CI [0.47, 0.75]]; P value = .09 for heterogeneity test, I2 = 49.2). The visual inspection of the funnel plot for the effect of ANC on NM illustrated a symmetrical distribution (Figure 5). Moreover, the Egger’s test indicated no publication bias among studies included (P value = .77). Hence, no major threat to the validity of the review.
Traditional Funnel Plot of 27 Included Studies of the Effect of ANC on Neonatal Mortality in Eastern Africa, 2021.
Discussion
Although several interventions have been made to improve the survival of newborns in recent years, NM remains a major concern worldwide, and SSA countries have a disproportionate burden of neonatal death; its impact is unacceptably high in many of the Eastern African countries. 61 Importantly, ANC is one of the fundamental strategies recommended to avert the risk of NM irrespective of sociodemographic backgrounds. In an attempt to improve the effectiveness of ANC on the neonatal outcome, so far several strategies and approaches have been implemented in SSA countries in general and the Eastern African region in particular.62, 63 Despite these efforts, the coverage of ANC service utilization and its effect on NM was not determined in the Eastern African countries. Hence, the current systematic review and meta-analysis aimed to determine the regional coverage of ANC service utilization and summarized the effect of ANC on NM in Eastern Africa.
In this meta-analysis, we found that the proportion of women who received at least 1 ANC service is 68.4% (95% CI [54.7, 82.1]). The finding of this study is consistent with a systematic review and meta-analysis result reported from Ethiopia which showed that the proportion of women who received at least 1 ANC was 63.77%. 64 However, the proportion of women receiving at least 1 ANC in this study is lower than the global average (87%), 65 and a demographic health survey reported from Kenya (96%) 66 and South Africa (94%). 67 The lower utilization of ANC in Eastern African countries might be related to poor quality of healthcare governance, inadequate health financing and human health resources, low standard health service delivery, and lack of transportation services to health facilities. 68 Furthermore, poor economic growth and political instability of the region, absence of a wide range of societal participation, and insufficient cost expenditure in health and related sectors have also led to unsatisfactory progress in reducing socioeconomic inequalities in health and reproductive, maternal, neonatal, and child health service interventions, especially among the most deprived groups.9, 61
The subgroup analysis of this study illustrate that the coverage of ANC service utilization among women is higher in facility-based (71.5%) compared to community-based studies (62.3%). The possible explanation for this may be because of women who are accessed from health facilities are better aware of their health and have better health-seeking behavior to improve the well-being of pregnancy outcomes compared to women recruited from the community setting.
Our study reveals that the pooled prevalence of NM is 8.5% (95% CI [7.3, 9.6%]) which was relatively consistent with a systematic review and meta-analysis reported from Ethiopia (6.78%). 69 However, the NM rate in this study (46.3 per 1000 live births) was higher than a systematic review and meta-analysis reported from worldwide (32.9 per 1000 live births) 70 and SSA (26.3 per 1000) live births, 14 and NM in West Africa (28.0 per 1000 live birth). 61 This high prevalence of NM in Eastern Africa is largely explained by high home birthing practice, 71 low standard maternal health services, poor socioeconomic status of the communities, and decades of political instability or conflicts. 9 The burden is further aggravated by unreliable transportation services to a health-care facility and the inability to pay for some medicine and additional laboratory investigation despite a free maternity care service decree in many of the Eastern African countries. These contribute to unacceptably high NM in the region.61, 72
Subgroup analysis by study region notes that the prevalence of NM is higher in the horn of African (8.9%) compared to the East African region (5.4%). The increased burden of neonatal mortality in the region is because the horn of Africa can be characterized as the most deprived and the poorest region in Africa, where the most basic needs of life (clean water, food, health care, and education) are not available to the majority of the population. 73 The region also lags behind the target such as skilled birth attendance and early postnatal care, and treatment interventions during pregnancy and childbirth that possibly can contribute to NM. 74
Furthermore, the pooled prevalence of NM rate is higher among participants recruited from the facility (12.4%) compared to community-based studies (3.1%), which was similar to a meta-analysis study reported from Ethiopia. 69 In this meta-analysis, most of the studies from a health facility were conducted on neonates that were admitted to the facility. Therefore, the overrepresentation of sick children might contribute to a relatively higher NM among studies conducted in a health facility compared to community-based studies.
This review showed the relationship between maternal ANC service use and NM. Accordingly, we found that a 42% reduction in risk of NM among women who attended at least 1 ANC visit compared to women who did not attend ANC visits. This is in line with a systematic review and meta-analysis reported from SSA (a 39% risk reduction) Ethiopia (a 58% risk reduction) of NM born to women who initiated at least 1 ANC visit.14, 63 Similarly, a systematic review and meta-analysis conducted in Zimbabwe and a demographic and health survey report from SSA demonstrated that the use of ANC service lowers the risk of NM by 41% 75 and 48%, 76 respectively.
It is important to note that more than a third (36%) of NM are attributable to infections that are largely related to maternal infection during pregnancy which in turn put a growing fetus at risk of developing neonatal complications, while the remaining causes of death include preterm and birth asphyxia. 77 ANC provides opportunities for disease prevention, early identification, and treatment of pregnancy complications which in turn help reduce the risk of neonatal infection and death. The provision of prophylaxis to anemia, malaria, and early detection and treatment of syphilis and urinary tract infections during ANC 78 can help to tackle the leading contributors of NM such as preterm birth and low birth weight. 79 For instance, intermittent preventive treatment of malaria in pregnancy reduces antenatal parasitemia and placental malaria and is associated with reductions in low birth weight (by 29%) and NM (31%). 80
Furthermore, ANC is essential to protect women from possible pregnancy complications through providing health promotion including counseling about birth preparedness and complication readiness plan during pregnancy that can indirectly reduce risks of NM. 18 Most importantly, ANC increases the women's chance of adhering to the continuum of care (institutional delivery/skilled birth attendants, and postnatal care), 81 82 83 hence, would reduce NM through the provision of quality essential newborn care including neonatal resuscitation, 84 newborn immunization, 85 counseling on breastfeeding, and maternal nutrition86, 87 that contributes to neonatal survival.87, 88
Strength and Limitations of the Study
One of the major strengths of this study was the inclusion of a large number of studies that fairly represented Eastern African countries through the use of a very sensitive search strategy. However, the findings are based on the data extracted from observational studies that are associated with inherent biases, the existence of heterogeneity even after subgroup analysis, and limiting the search to an article published in the English language was considered as limitations of this study. Despite these limitations, the current review has provided evidence regarding the relation between ANC and NM and indicated the need to scale up ANC as a strategy to reduce NM in Eastern Africa.
Conclusion
One-third of pregnant women did not receive at least 1 ANC service from a skilled provider, and the prevalence of NM was relatively high in the region. According to this finding, NM was markedly declined for neonates born to women who had as few as 1 ANC visit compared to those who had no ANC visit. Therefore, intensifying efforts that improve ANC service volume could yield in reduced NM in Eastern Africa.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material for Antenatal Care Predicts Neonatal Mortality in Eastern Africa: A Systematic Review and Meta-analysis of Observational Studies by Getahun Tiruye, Kasiye Shiferaw, Addisu Shunu, Yitagesu Sintayeu and Abdulbasit Musa Seid, in Journal of Neonatology
Footnotes
Authors' Contributions
Conceptualization: Getahun T., Kasiye S. Methodology, software, formal analysis, validation, data curation, and investigation: Getahun T., Abdulbasit M. Seid, Kasiye S., Yitagesu S., and Addisu Shunu. Writing original draft preparation, writing review, and editing: Getahun T., Abdulbasit M. Seid, Kasiye S., and Addisu Shunu. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.