
Abstract
Introduction:
Congenital hypothyroidism (CH) is seen more often in preterm and low birthweight infants. However, very few studies exist that explore the epidemiology and risk factors associated with CH, especially from the Indian subcontinent.
Methods:
A cross-sectional screening study was carried out on 240 low birthweight (<2.5 kg) and late preterm (34-36.6 weeks) newborns not requiring ventilator support over a period of 18 months. A total of 0.5 mL of venous sample was obtained on day 4 of life for analyzing thyroid stimulating hormone (TSH), tetraiodothyronine (T4), as well as tetraiodothyronine (T3) levels by an architect plus Chemiluminescence microparticle immunosorbent assay. Neonates with TSH values of more than 20 mIU/L were categorized as having elevated TSH.
Results:
Elevated TSH was seen in 10 (4.2%) neonates. The presence of maternal anemia (P = .011), gestational diabetes mellitus (GDM) (P < .001), and maternal hypothyroidism (P < .01) was found to be significantly linked to elevated TSH levels. Other maternal comorbidities, gestational age, birthweight, as well as the nature of birth bore no significant relation with CH.
Discussion:
Elevated TSH was found to be common in late preterm and low birthweight newborns. Neonates of mothers suffering from hypothyroidism, advanced maternal age, GDM, and maternal anemia should be serially evaluated for thyroid abnormalities as they possess a significantly higher risk of having elevated TSH levels.
Introduction
Congenital hypothyroidism (CH) results either due to an absent/underdeveloped thyroid gland (dysgenesis), or its inability, to produce enough thyroid hormone (dyshormonogenesis). Since the clinical manifestations of CH are often subtle or absent at birth, a delay in its diagnosis threatens the neurodevelopmental function of infants, especially those that are preterm and/or have low birthweight.1-3
The reported incidence of both CH and preterm infants has increased significantly during the past 2 decades due to the practice of newborn screening (NBS) in most developed countries. 4 However, India has yet to embark upon a national NBS program despite screening guidelines being framed by the Indian Society for Paediatric and Adolescent Endocrinology (ISPAE) and strong advocacy by the Indian Academy of Paediatrics (IAP).5,6
Hence, epidemiological data about CH remains scarce in the Indian subcontinent with a few studies revealing an incidence rate anywhere between 1 in 479 in Kochi and 1 in 2,640 births in Mumbai.7,8 Despite our best effort, we could not find any Indian data about the incidence of CH in late preterm and low birthweight neonates. Thus, we carried out this study to screen for the presence of significantly abnormal thyroid profile in the hope of broadly estimating the burden of CH in late preterm as well as low birthweight babies born in a tertiary care hospital and correlate the findings with various demographic as well as maternal factors.
Materials and Methods
This cross-sectional screening study was conducted in the department of pediatrics after receiving institutional ethics approval. Participant recruitment and sample collection was carried out after obtaining a written and informed consent from the parents/guardians of the newborns over a period of 18 months (September 2019 to June 2021).
Consecutive, late preterm (34-36.6 weeks) as well as low birthweight (<2.5 kg) newborns, not requiring ventilator support and without severe congenital anomalies, were considered eligible for inclusion in the study. A total of 0.5 mL of venous sample was obtained on day 4 of life under strict aseptic precautions and transported to the central research laboratory for analyzing thyroid stimulating hormone (TSH), tetraiodothyronine (T4), as well as tetraiodothyronine (T3) levels by an architect plus Chemiluminescence microparticle immunosorbent assay. Neonates with TSH values of more than 20 mIU/L and T4 less than 10 ug/dL were categorized as having elevated TSH according to the latest guidelines and age-appropriate cut-off values.6,9 A repeat sample at 2 weeks of age or later was planned to confirm diagnosis of CH but could not be undertaken due to logistical constraints.
Quantitative variables were described using percentages, ranges, means, and standard deviations. Student’s independent t test, analysis of variance test, and Spearmen’s correlation analysis were performed using the Statistical Package for the Social Sciences Version 22 (SPSS Inc) as appropriate. The Pearson chi-square test was used to compare categorical data. A 2-tailed probability value of .05 or less was considered as statistically significant.
Results
Demographic Details
A total of 240 (135 females; 105 males) late preterm (mean gestational age: 35.465 ± 0.819 weeks) neonates with weight ranging from 1.4 kg to 2.5 kg (mean: 2.210 ± 0.2919) constituted our study population. The maternal age ranged from 18 to 36 (mean: 27.00 ± 4.045) years. A total of 166 infants (69.2%) were born after a normal vaginal delivery while the rest (74, 30.8%) needed a caesarean section. The majority of mothers (171, 71.3%) had no comorbidity while 26 (10.8%) had gestational diabetes, 25(10.4%) suffered from preeclampsia, while 10 (4.2%) had anemia. Maternal hypothyroidism was seen in 17 (7.1%) females, all of whom were under treatment.
Neonatal Thyroid Profile
Association of Maternal Variables With Congenital Hypothyroidism.
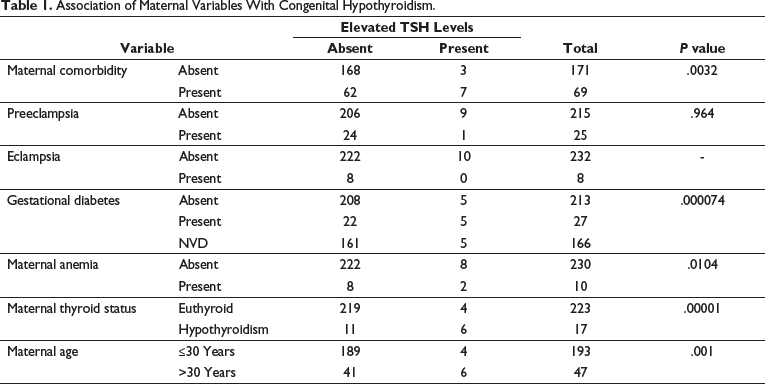
Serum TSH, but not serum T4, was significantly and positively correlated with maternal age (r = 0.280, P < .001), that is, an increase in serum TSH was observed with increasing maternal age. Neonates with elevated TSH were more likely to be the product of higher maternal age (32.20 ± 3.490 years) than those without CH (26.77 ± 3.920 years, P < .001). No correlation was seen between serum TSH/T4, gender, birth weight, or gestational age. Babies born by caesarean section were found to have a significantly higher serum TSH (8.79 ± 19.29 mIU/L) than those born via normal vaginal delivery (4.622 ± 10.357 mIU/L, P = .031). Mothers who were hypothyroid had a significantly higher serum TSH (33.49 ± 36.23 mIU/L) than those that were euthyroid (3.8 ± 6.97 mIU/L, P < .001).
Discussion
Several studies have demonstrated CH to be more common in India than the rest of the world. 10 However, to the best of our knowledge, no study exists documenting CH in low birth weight and late preterm Indian neonates, a group which is inherently more susceptible to adverse neurodevelopmental outcomes. Thus, we set about trying to fill this lacuna by analyzing the thyroid profile of late preterm low birth weight neonates without any congenital abnormalities. As suggested by previous studies, we analyzed venous samples on the third day to minimize the false positive high TSH that often happens in the initial 72 h of life due to a physiological rise. 11 Repeat samples could not be taken due to financial considerations as well as the fact that previous studies have shown that performing a second TSH screen in preterm infants is unnecessary. 12
Our study found the prevalence of elevated TSH in late preterm and low birthweight neonates to be significantly higher (1:25) than several European and American NBS programs (ranging from 1:105 to 1:1589).13-16 The prevalence of elevated TSH was also found to be much higher than an Indian study which had a prevalence of 1.7% screen positive cases. 17 Another Indian study found the prevalence of CH to be 3.1% in very sick preterm neonates admitted in the newborn intensive care unit. 18 Previous studies have found confirmed CH to be much more common in preterm neonates (around 2.5%) with some earlier European studies showing their incidence ranging from 1.5% to 18%.19-22 An earlier study from Wisconsin had found elevated TSH levels in only 0.43% of preterm infants on screening. 23 The prevalence of neonates with elevated TSH could have been high in our center due to it being a referral tertiary care hospital catering to high-risk pregnancies.
The demographic characteristics of neonates in our study were similar to most previous studies.24,25 However, our study, like others before it, found that a higher maternal age was significantly associated with a significantly abnormal thyroid profile. This could be due to the fact that an increase in maternal age leads to a decline in physiological and reproductive functions leading to adverse pregnancy outcomes. 26
In the present study, we found that elevated TSH levels had a statistically significant association with maternal hypothyroidism due to the fact that maternal and fetal thyroid functions are not entirely independent of each other, with the fetal thyroid activity depending on the availability of iodine transferred from maternal circulation. 27 This association has been reiterated by previous studies. 28 Gestational diabetes was found to be the most common maternal comorbidity in our study and its presence was significantly associated with the finding of elevated levels of TSH. Similar associations have been found in previous studies; however, the causal relationship between GDM and CH remains unclear.26,29,30 One possible mechanism for the same could be the increased risk of developing thyroid antibodies in mothers with GDM. 31
Anemia, seen in 10 of our mothers, was also found to be significantly associated with the detection of elevated TSH. Though we could find any study which had analyzed the reason behind their correlation, a possible mechanism for their association could be the important role of iron in the normal functioning of thyroid peroxidase, a heme-dependent protein which facilitates thyroid hormone synthesis. Like previous studies, no correlation was found between hypertensive disorders of pregnancy and CH. 24 Similarly, the mode of delivery was not found to have any association with CH.
To the best of our knowledge, this study forms the first exploratory study from the Indian subcontinent which establishes a nomogram in low birthweight as well as late preterms regarding the prevalence as well as risk factors of elevated TSH levels during screening. However, our study is not without limitations, the main limitation being the lack of a second sample after 2 weeks of birth to differentiate transient from permanent CH. This wasn’t possible due to the wide geographical spread, the pandemic, as well as the extremely low-income group of our patients. A study limited to a single center can also not portray the prevalence of CH accurately. Thus, future larger, multicentric studies are required to calculate the prevalence of CH accurately in the community.
In summary, we conclude that abnormal thyroid function is common in infants that are late preterms as well as low birthweight. This underscores the urgent need to embark upon a national newborn screening program following the guidelines already laid down by ISPAE and IAP. Clinicians need to give special emphasis to neonates born from mothers suffering from hypothyroidism, advanced maternal age, GDM, and maternal anemia as they are known to possess a significantly higher risk of developing CH.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.