
Abstract
Background
Histological chorioamnionitis (HCA) is present not only in women with clinical chorioamnionitis (CCA) but also in a large subset with silent chorioamnionitis which has a risk of developing complications of preterm labor, fetal, and maternal infection.
Objectives
To assess HCA and funisitis, and their correlation with the early neonatal outcome.
Methods
Of 778 preterm babies born over a period of 1 year at ≤34 weeks gestation, 100 placentae were analyzed as per the inclusion criteria in this prospective study. Sections from the placenta, membranes, and umbilical cord were examined for histopathology. Clinical parameters in mother and neonate were recorded and correlation with HCA was estimated.
Results
The incidence of HCA, funisitis, CCA was 35%, 7%, and 24%, respectively. Sixteen of 24 (66.7%) CCA had HCA and 19/35 (54%) of HCA had no CCA. History of preterm premature rupture of membranes was there in 73/100 cases, of which 41 had HCA. HCA cases having duration of rupture of membranes (DROM) <24 h were 22/41 (53.6%), 77.2% of which developed early onset neonatal sepsis (EONS). Odds of EONS with DROM <12 and 24 h was 1.3 and 2.9, respectively. EONS was suspected in 28/35 (80%) of HCA versus 13/24 (54%) of CCA. Culture positive sepsis was seen in (9/28) 32% cases with HCA and funisitis. In the absence of HCA, EONS was suspected in 30.7% cases.
Conclusion
HCA has a better diagnostic ability to detect EONS. Sepsis screen on the basis of CCA alone can miss about 50% of cases.
Keywords
Introduction
The incidence of preterm babies in developed countries varies from 7% to 12% of all births. 1 In low- to middle-income countries, the incidence is less than 15% of all births. As per the World Health Organization estimates, there are 15 million preterm births globally and 1 million direct fatalities annually. In India, out of 26 million live births, 3.5 million births are preterm of which 3.03 lakh babies die due to subsequent complications. India tops the list of 10 nations contributing to 60% of the world’s premature deliveries. Chorioamnionitis is a major determinant of preterm birth and is estimated to be present in approximately 2% to 4% of term pregnancies, and in 40% to 70% of women who deliver prematurely. 2
Most of the studies on histological chorioamnionitis (HCA) are from high-income countries and studies from the developing world are scarce.3, 4 Microscopic evaluation of the fetal membranes and placentae serves as the gold standard in the diagnosis of chorioamnionitis. HCA is highly associated with preterm birth and subsequently with adverse neonatal outcome. It is present not only in women with overt signs of clinical chorioamnionitis (CCA) but also in a large subset of women with no clinical features or symptoms of infection, the understudied yet ominous entity of “silent chorioamnionitis.” These patients have a similar risk of developing complications of preterm labor, neonatal sepsis, and other fetomaternal complications.
Ethnicity, race, and socioeconomic factors along with period of gestation have an influence on incidence of HCA. Nevertheless, there exists a compelling lack of available studies highlighting the role of chorioamnionitis in preterm deliveries, especially from the Indian subcontinent. The present study aims to corroborate the data with regard to incidence and short-term neonatal outcomes of HCA.
Materials and Methods
The present prospective observational study was conducted in the Department of Pathology, in collaboration with the Departments of Obstetrics & Gynecology and Neonatology, Government Medical College and Hospital, Chandigarh, India. The study is reported as per the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, 2010 for observational studies. Ethical clearance was taken from the Institutional Ethics Committee. A written informed consent was taken from the mothers and a total of 100 placentae were collected from preterm deliveries of ≤34 weeks (June 2016-2017). Cases with unavailability of umbilical cord sample, maternal death in delivery room, maternal causes of preterm delivery (eg, antepartum hemorrhage, chronic maternal illness), congenital anomalies/malformations at birth, malformations of placenta, and cord and twin pregnancy were excluded from the study.
Primary Objective
To evaluate the incidence of HCA in the placenta and fetal membranes and their correlation with early neonatal outcome.
Secondary Objective
To compare the accuracy of HCA with CCA in detection of early onset neonatal sepsis (EONS).
Sample Size
Based on the available literature, we expected to have at least 40% incidence of chorioamnionitis, with α error of 0.05 and power of 90%. A sample of 79 was therefore required for 2-tail significance. To account for the sampling error, it was decided to enroll 100 placentae.
Histopathological Analysis
Placenta, placental membranes, and umbilical cord of neonates born on working days (8 AM-5 PM) were collected and preserved in 10% neutral buffered formalin. Placental specimens were grossly examined for any structural anomalies and physical signs of chorioamnionitis, including exudates, hemorrhages, vascular abnormalities, and status of membranes. Each specimen was measured and weighed. Sections were taken from each placenta and put into at least 4 blocks. One block included a roll of the fetal membranes and 2 transverse sections from the umbilical cord. Three full thickness sections of normal looking placental parenchyma were taken including area within central two-thirds of the placenta. Grossly identifiable lesions were documented and sampled with a minimum of 1 block. Sections were processed for paraffin embedding. Sections of 3 to 5 µm thickness were cut and stained with hematoxylin and eosin (H&E). A detailed microscopic examination was undertaken to determine the changes and abnormalities present in the form of maternal and fetal inflammatory reaction and any other pathology. A systemic staging and grading of the inflammation was performed in accordance with protocol provided in “placenta reaction patterns related to amniotic fluid infection sequence: nomenclature and definitions.” 5
A 2-tiered grading system and 3-tiered staging system was utilized to quantify both maternal and fetal inflammatory response. Maternal response was staged as stage 1 (subchorionitis/acute chorionitis), stage 2 (moderate-acute chorioamnionitis), and stage 3 (severe-necrotizing chorioamnionitis). Grade 1 showed focal/patchy and grade 2 had diffuse/confluent/severe neutrophilic infiltrate (≥10 × 20 cells in extent) between chorion and decidua; >3 isolated foci or a continuous band.
Fetal inflammatory response in the form of microscopically detected funisitis was staged (stage 1—phlebitis and/or intramural chorionic vasculitis, stage 2—umbilical arteritis or trivasculitis, and stage 3—necrotizing funisitis) and graded (grade 1—mild/moderate, scattered neutrophilic infiltrate and grade 2—severe, near confluent neutrophils with degeneration of vascular smooth muscle cells).
Neonatal Parameters
The demographic profile, obstetric and medical history, examination, relevant investigations performed, and treatment regimen in each case were recorded. Neonatal parameters at birth, condition during the course of admission, and outcome till discharge were noted. Primary short-term neonatal outcomes in terms of “EONS” and “respiratory distress” were studied. Other neonatal morbidities like patent ductus arteriosus, necrotizing enterocolitis, meningitis, intraventricular hemorrhage, periventricular leukomalacia, bronchopulmonary dysplasia (BPD), and retinopathy of prematurity were evaluated to gauge the effects of chorioamnionitis in preterm infants.
Definitions
HCA—Defined in terms of fetal and maternal inflammatory response. The maternal inflammatory response includes subchorionitis, chorionitis, and chorioamnionitis and the fetal inflammatory response includes chorionic vasculitis, umbilical phlebitis, and funisitis. The diagnosis of HCA was based on a semi-quantitative assessment of inflammatory cells in the amniochorion membranes, umbilical cord, and placental disc.
CCA—Considered in the setting of maternal fever along with any 2 of the following criteria: maternal leukocytosis, maternal tachycardia, fetal tachycardia, uterine tenderness, and foul smelling vaginal discharge/amniotic fluid. 6
Silent chorioamnionitis—No clinical features or symptoms of infection but having HCA.
EONS—Any neonatal sepsis occurring within first 72 h of birth. Sepsis was considered as probable in case of clinical symptoms and positive biochemical parameters but negative blood culture. If blood culture grew an organism, it was taken as proven sepsis.
The results of the pathological studies were correlated with the clinical findings for the final evaluation. Chi-square test and Fischer’s exact test were applied for categorical variables. Student t test was used for nominal data. Normality of the measurable data was checked using Kolmogorov-Smirnov test. Parametric tests (Student t test/ANOVA) was applied for normally distributed data. Nonparametric tests (Mann-Whitney U test/Kruskal-Wallis test) were utilized for skewed data. SPSS-19 (IBM SPSS Statistics for Windows, Version 19.0; IBM Corp) software was utilized for the statistical analysis.
Results
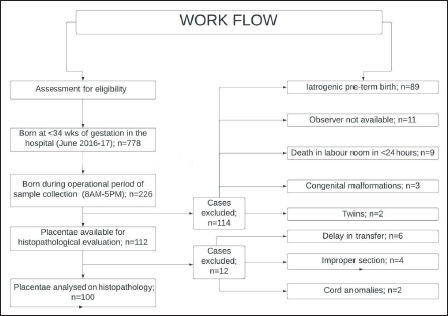
Of 778 babies born at ≤34 weeks of gestation, 112 were eligible as per the inclusion criteria while 12 were excluded due to sampling errors/cord anomaly or delay in transfer of placenta for histopathological evaluation (Figure 1). HCA was assessed in all the cases. The incidence of HCA, funisitis, and CCA was 35%, 7%, and 24%, respectively. The mean (±standard deviation) age of mothers in the study population was 25.6 ± 4.6 years. Nineteen women (27.9%) who were multigravida had a previous history of preterm birth. Half (50%) of the women received corticosteroids of which 74% received full course whereas 26% received a single dose. Intrapartum antibiotics were received by 89 women, 70 (78.6%) of whom received a dose of antibiotics 4 h before delivery. Most presented with complaint of preterm premature rupture of membranes (PTPROM) (Table 1). PTPROM was seen in 30/35 (87.5%) of HCA cases.
Workflow of the Current Study.
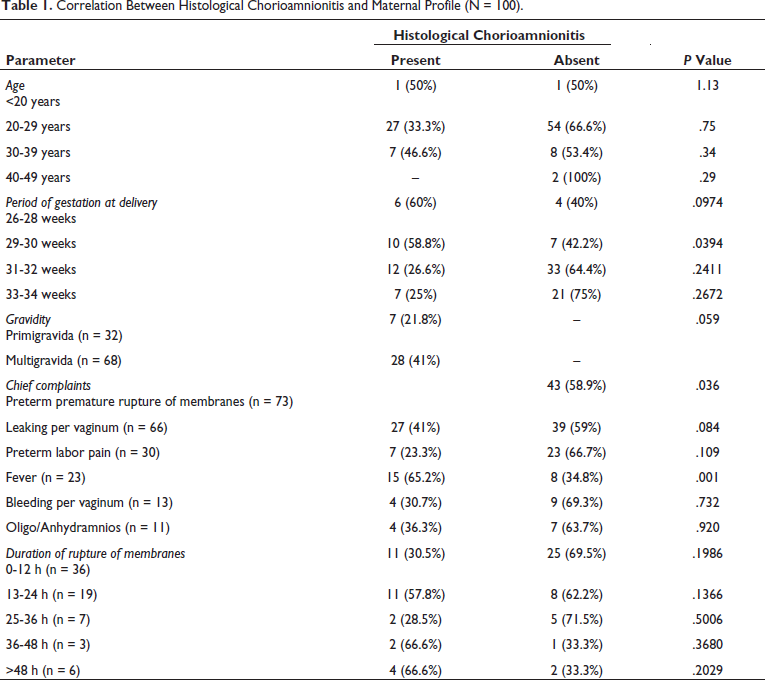
Correlation Between Histological Chorioamnionitis and Maternal Profile (N = 100).
For a valid statistical analysis, the neonates were divided into 2 groups; HCA positive preterm births (n = 35) and non-HCA preterm births (n = 65). The HCA positive subgroup showed a slight male preponderance (M:F = 1.18:1) whereas the non-HCA subgroup showed a slight female preponderance (M:F = 0.9:1). Neonates born to HCA positive pregnancies weighed slightly less (mean weight = 1.48 Kg) as compared to those born out of HCA negative preterm deliveries (mean weight = 1.64 kg). However, this parameter was not statistically significant (P value = 0.8).
Subchorionitis/Acute chorionitis—stage 1 was seen in 19 of the 100 placentae. Acute chorioamnionitis (Figure 2)—stage 2 was observed in 14 and necrotizing chorioamnionitis (Figure 3)—stage 3 in 2 placentae. Grade 1 and 2 were seen in 15 and 20 cases, respectively. Out of the 35 placentae detected with HCA, 7 (1—stage 1 and 6—stage 2) showed funisitis. Infarction necrosis was seen in 1/35 cases, focal calcification in 2/35 cases, and perivascular hemorrhage (Figure 4) in 3, one of which had HCA, grade 1.
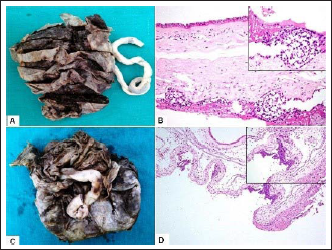
Acute chorioamnionitis. (A). Gross photograph of placenta showing opaque membranes in acute chorioamnionitis. (B). Acute chorioamnionitis (stage 2, grade 1) with presence of patchy neutrophilic infiltrate in chorion and amnion (H&E, ×200). Inset shows focal chorionic neutrophilic collections (H&E, ×400). (C). Gross photograph of placenta showing dull and opaque membranes in acute chorioamnionitis. (D). Acute chorioamnionitis (stage 2, grade 2) with presence of confluent neutrophilic aggregates in chorion (H&E, ×40). Inset shows neutrophilic microabscess (H&E, ×200).
Necrotizing chorioamnionitis (A and B) and acute subchorionitis (C and D). (A). Gross photograph of placental fetal surface showing thick, gray tan, and opaque membranes in necrotizing chorioamnionitis. (B). Necrotizing chorioamnionitis (stage 3, grade 2) with plentiful chorionic microabscesses, subamnionic degenerating neutrophils, and karyorrhectic debris admixed with bacterial colonies (H&E, ×200). (C). Acute subchorionitis (stage 1) showing neutrophils limited to the subchorionic layer (H&E, ×100). (D). Diffuse neutrophilic infiltrate admixed with subchorionic fibrin in acute subchorionitis (H&E, ×200).
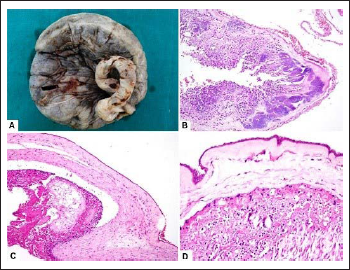
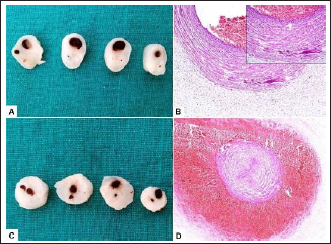
Funisitis (A and B) and perivascular hemorrhage (C and D). (A). Gross photograph showing multiple serial transverse sections from umbilical cord in funisitis. (B). Section from umbilical cord showing transmural neutrophilic infiltration of umbilical vein and Wharton jelly in funisitis (H&E, ×100). Inset shows the neutrophils in vessel wall (H&E, ×200). (C). Gross photograph showing multiple serial transverse sections from umbilical cord depicting perivascular hemorrhage. (D). Section from umbilical cord showing massive hemorrhage around the umbilical artery (H&E, ×40).
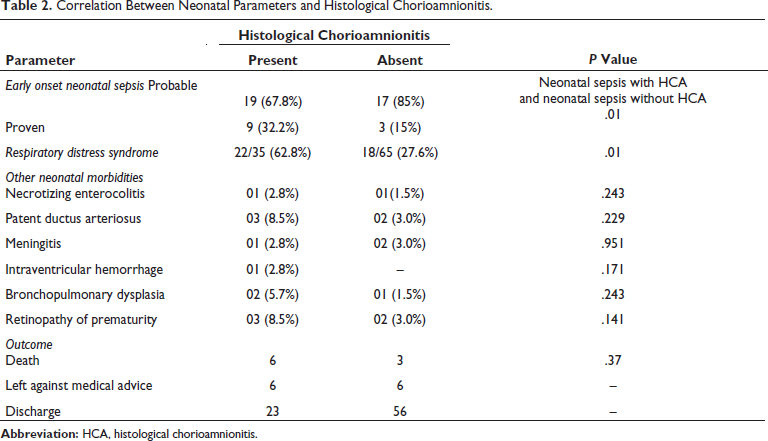
The APGAR scores in newborns in cases with HCA were significantly lower as compared to the non-HCA subgroup (P value < .05). Table 2 provides the correlation between neonatal parameters and HCA. In the HCA subgroup, 9% (2/22) cases that developed respiratory distress syndrome (RDS) were diagnosed later with BPD whereas 5.5% (1/18) of the cases in non-HCA, RDS subgroup developed BPD.
Correlation Between Neonatal Parameters and Histological Chorioamnionitis.
The Diagnostic Ability of CCA and HCA for EONS
HCA was seen in 16/24 (66.7%) of patients with CCA and 19/35 of the cases with HCA had absence of any signs of CCA and were designated as cases having “silent chorioamnionitis.” CCA was seen in 24% of the cases. Fever alone was seen in 9/24 (37.5%) of cases whereas 6/15 (62.5%) cases showed fever +1 more feature of CCA. Among HCA, 54% had a positive correlation with shorter gestation (<30 weeks).
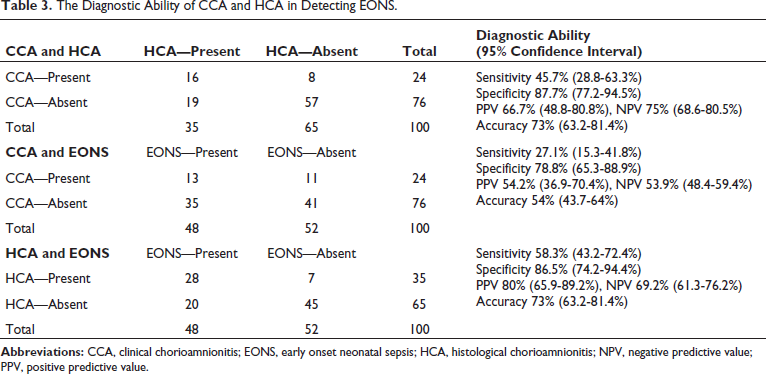
Of cases with DROM of <24 h, 77.2% later on developed EONS. Odds of EONS with DROM <12 and 24 h was 1.3 and 2.9, respectively. EONS was encountered in 13/24 (54%) of the cases with CCA. Blood culture positive sepsis was seen in 9/28 (32%) of cases with HCA and funisitis. Placental inflammation was seen in 13.5% (7/52) of placentae from infants without probable neonatal sepsis. Five of the 7 neonates with funisitis on histopathology were treated for probable EONS. HCA had better diagnostic ability to detect EONS (Table 3). In the absence of HCA, EONS was suspected in 30.7% of the cases.
The Diagnostic Ability of CCA and HCA in Detecting EONS.
Discussion
Chorioamnionitis is a commonly encountered obstetric problem, which when allowed to escape untreated can result in significant maternal and neonatal complications including mortality. The diagnosis of chorioamnionitis is clinched on the basis of either clinical and/or histological findings. 7 The plethora of clinical symptoms associated with chorioamnionitis (foul smelling discharge per vaginum, fever, maternal tachycardia, pain abdomen, and raised maternal leucocyte count) is a good predictor. The pathological examination provides a retrospective yet confirmatory proof of its existence and extent.
The clinical signs and symptoms of chorioamnionitis are not 100% sensitive. In the present study, 8 out of 24 cases with CCA did not have HCA. This can be explained by low sensitivity of maternal tachycardia, C-reactive protein (CRP), uterine tenderness, and maternal leukocytosis.8, 9 Furthermore, there remains a subset in which established HCA is unaccompanied by classical clinical features, “the silent chorioamnionitis.” 5 Although clinically silent, this entity is known to be closely associated with premature birth, reproductive casualty, and neonatal morbidity. In the current study, silent chorioamnionitis, with no clinical features or symptoms of infection but having HCA, was present in 54% cases with diagnosed HCA. On further analysis, it was noted that most of the cases (12/19, 63%) with silent chorioamnionitis had a mild (grade 1) inflammatory involvement while only 7 cases showed grade 2 and none of the cases showed grade 3 HCA. Better association of HCA with early neonatal and perinatal morbidities than CCA mandate routine placental histological examination in very preterm births for a good prediction of perinatal and neonatal outcome. 10 Recently, higher early CRP levels have been established as a surrogate predictor of HCA and its levels parallel the severity of HCA. 11
The rate of HCA was found to be inversely related to duration of gestation in this study, in keeping with the observations that lower the period of gestation, greater is the incidence of HCA.12–14 In a study by Mueller-Heubach and colleagues, 15 HCA was present in 34% (61/181) of placentae from preterm deliveries as compared to 19% (295/1524) in those with term deliveries. A slightly higher percentage of cases with HCA in the present study can be attributed to the inclusion of placentae from gestation age <34 weeks only as compared to all preterm deliveries in the aforementioned study.
The incidence of HCA among various races delivering at <32 weeks of gestation age has been reported to be 40% to 80% and is associated with poor neonatal outcome.12–14, 16 Bacteria have been recovered from subchorionic plate from 72% of placenta with HCA and 40% to 80% of these neonates develop neonatal sepsis.17, 18 It has long been debated whether the presence of intrauterine infection is a causative factor or a consequence of premature rupture of the fetal membranes.7, 19, 20 There is convincing evidence on both sides. On one hand, pre-existing genital tract infection may precipitate rupture of membranes. While on the other hand, the premature rupture of membranes may lead to the formation of a portal for entry of infection and its spread into the sterile amniotic cavity. However, in either scenario, the role of inflammatory cytokines in the initiation of labor is paramount. In the present study, PTPROM was present in 73% of the pregnant women who delivered earlier than 34 weeks of gestation. Of these women, 39.7% (29/73) had HCA. Fifty percent of these women with HCA had clinical features of chorioamnionitis. The incidence of HCA in PTPROM cases reported in literature ranges from 13% to 59%.21–23
A significant relationship between DROM and intraamniotic infection exists. 24 In the present study, the mean DROM in cases with HCA was 54 h whereas in cases without HCA, it was 16 h and a significant correlation between greater DROM and HCA was seen. Nonetheless, some researchers have documented a lack of correlation between rate of CCA and duration of the latency period.25–28 This observation has been used to favor and justify the expectant management of PROM pregnancies of less than 34 weeks, period of gestation as a significant number of fetuses would stand to benefit from the increased maturity gained during the latency period while the risk of chorioamnionitis and neonatal infection remain low.
Incidence of infections among preterm neonates inversely correlates with the gestational age.29, 30 The current study revealed a statistically significant higher incidence rate of EONS among infants exposed to HCA and funisitis. Probable EONS was detected in 28/35 (80%) of HCA as compared to 13/24 (54%) of CCA. HCA has a better diagnostic ability to detect EONS. Sepsis screen on the basis of CCA alone can miss about 50% of cases. Odds of developing EONS are high even with DROM less than 24 h, which is considered conventionally as prolonged rupture of membranes.
The APGAR scores in newborns in cases with HCA were significantly lower as compared to the non-HCA subgroup thereby suggesting the presence of perinatal asphyxia in affected neonates. The effect of chorioamnionitis on fetal lung development and subsequent neonatal respiratory outcomes is controversial. A comprehensive narrative review on the impact of HCA on respiratory outcomes in premature infants found considerably heterogeneous results. 31 In this study, 9% cases in HCA group developed BPD whereas 5.5% of the cases in non-HCA developed BPD. A recent systematic review and meta-analysis concluded that chorioamnionitis was a significant risk factor for BPD. 32
We have tried to establish the correlation of HCA and CCA with the early neonatal outcome and considering the scarcity of such studies from the Indian set up, this is the major strength of this study. However, determination of HCA was not point of care and was done from a research perspective in this study, which is a limitation. Correlation of neonatal CRP with HCA was not done in this study, which could have been done as CRP assessment is a point of care test. Future direction lies in evaluation of latency of rupture of membranes and development of EONS.
To conclude, HCA is an important entity responsible for a considerable proportion of preterm births and is associated with significant neonatal morbidities. HCA has better diagnostic ability to detect EONS as compared to CCA. There is hence a compelling need for enhanced preventive care strategies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance was taken from the Institutional Ethics Committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.