
Abstract
Objective
To compare an infrared thermometer (IRT) at the forehead with a Digital thermometer (DT) at the axillary site in neonates in the delivery room.
Methods
Temperature was assessed simultaneously in 65 neonates born at ≥34 weeks in the delivery room with IRT at the forehead site and DT at the axillary site at 1 and 5 min of age. Immediately after delayed cord clamping, skin-to-skin contact (SSC) was given for vaginal-born neonates, and a radiant warmer was used for cesarean-born neonates.
Results
In a total of 130 paired measurements, the intraclass correlation coefficient (ICC) between the IRT and the DT was good, ICC = 0.859, P < 0.001; the bias (SD) was –0.16(0.42)°C in Bland-Altman analysis. The correlation between IRT and DT during SSC was ICC = 0.881, P < .001, and the bias (SD) was –0.14(0.33)°C; and for neonates cared under radiant warmer, the ICC was 0.846, P < .001 with bias (SD) of –0.17(0.47)°C.
Conclusion
Temperature assessed by IRT at the forehead site shows good reliability with DT at the axillary site in neonates for thermal management in the delivery room.
What Is Known?
DT is commonly used to assess temperature monitoring in neonates.
What This Study Add?
IRT at the forehead site is clinically reliable for temperature assessment in neonates during delivery room care.
Introduction
Hypothermia causes significant morbidity and mortality in neonates. 1 Temperature drops of 1°C below 36.5°C during hospital admission are associated with increased neonatal mortality. 2 In a retrospective study, around 25% of neonates born at >34 weeks gestational age became hypothermic within 6 h of birth and hypothermia increased the risk of adverse outcomes that is, neonatal intensive care admission, respiratory distress, and longer duration of hospital stay. 3 Thermal care and serial temperature monitoring in the delivery room for all neonates are the first and foremost steps towards a better physiological state. Immediately after delivery, uninterrupted skin-to-skin contact (SSC) between mother and infant is the current standard of care to initiate breastfeeding and hypothermia prevention; and it is endorsed by the World Health Organisation. 4 However, repeated temperature monitoring during SSC is also requested for late preterm, early term neonates, low birth weight infants, and small for gestational age neonates, considering the potential risk of hypothermia. 5
Neonatal temperature is conventionally measured by various techniques, that is, human touch, mercury-glass thermometer, and digital thermometer (DT). 6 Among them, DT at the axillary site is a commonly accepted method for temperature measurement in both developed and developing countries. The application of DT during SSC care is associated with an interruption in the thermal covering of the neonate (warm blanket) and disturbance in the neonatal behavioral state. Infrared thermometers (IRT) give instantaneous temperature readings without touching the skin’s surface or causing any disturbance. It measures the temperature from the radiated heat from the subcutaneous arterial blood supply at the forehead site. 7 Overall, the utility of IRT was well accepted by all clinicians and public places during the COVID pandemic. Similarly, it may help in avoiding cross-infection between neonates. However, the use of IRT in neonates has not been reliably studied. The present study was to compare the temperature measurements by IRT at the forehead site with the axillary temperature recorded by DT in neonates immediately after birth.
Methods
This comparative prospective study was conducted in the delivery room of a tertiary care hospital in India over a period of two months, between August 2022 and September 2022. The institutional ethical committee had approved this study, and parental written informed consent was obtained prior to enrolling study participants.
All intramural singleton neonates born at a gestational age of ≥34 weeks were enrolled in this study. Neonates requiring resuscitation, the presence of respiratory distress, and major congenital malformations were excluded.
All mothers with a gestational age of ≥34 weeks who were prepared for vaginal delivery were antenatally counseled for SSC. However, SSC was not practised in neonates born by cesarean section during the study period. Prior to each delivery, there was a discussion between the attending pediatrician and obstetrician about the plan for delayed cord clamping and SSC in vaginal delivery cases. All measures were taken to maintain an optimal delivery room temperature of around 23°C–25°C for each delivery. A nursing officer was present at each delivery to record time and for documentation. Once the baby was delivered, the birth time was duly noted, the neonate was assessed, and immediate care was taken as per neonatal resuscitation protocol by one of our research team members. 8 After birth, the neonate was placed on the mother’s abdomen, and the baby was immediately dried with a pre-warmed cloth. The presence of spontaneous breathing effort, gestational age-appropriate muscle tone, and a heart rate of more than 100 per minute defined a neonatal vigorous state. Cord clamping was done at least 60 sec after birth.
The baby, delivered by vaginal birth, was put between the mother’s breasts in a prone position with SSC, and the baby’s face was turned to one side close to the mother’s nipple. 9 The baby was covered by a pre-warmed cloth during SSC. For a cesarean-born neonate, the baby was transferred to a radiant warmer after cord clamping and routine care was given. The baby was closely monitored by the pediatrician and nursing personnel for 1 h in all deliveries.
The pediatrician and the nursing officer took body temperature readings from each newborn (both vaginal and cesarean born) at 1 min and 5 min of age. Axillary temperature measurements were recorded using a DT (Dr. Trust USA DT) after cleaning the axilla with a dried swab. Simultaneously, non-contact temperature measurement at the mid-forehead site was done by a single factory-calibrated IRT device (Sahyog Wellness Multi-Function Non-Contact Body IRT). Both temperature recordings were in degrees Celsius. Any decision regarding the thermal management of the baby was based solely on the DT reading. Neonates were labeled euthermic and hypothermic when their axillary temperatures were 36.5°C–37.5°C and <36.5°C, respectively. 10
Sample Size
Assuming the minimum acceptable reliability of IRT intraclass correlation coefficient (ICC) = 0.8; expected reliability of ICC = 0.9 and two repetitions per subject, with a 95% confidence interval and 80% power, the calculated sample size was 58. Assuming a 10% dropout, the final sample size was calculated to be 65.
Statistical Analysis
Continuous data were represented as mean (SD), and categorical variables as frequency (%). Agreement between temperature recording with DT and IRT was analyzed by ICC 11 and Bland Altman (BA) analysis. 12 The ICC value shows the reliability between two methods of temperature recording; that is, >0.9 – excellent, 0.75–0.9 – good, and 0.5–0.75 – moderate. In BA analysis, bias indicated the average difference between DT and IRT; and 1.98 times SD represented the upper and lower limit of the line of agreement (LOA). Data were analyzed by software IBM SPSS version 24.0 (IBM Corp). A P-value < .05 was considered to be statistically significant.
Results
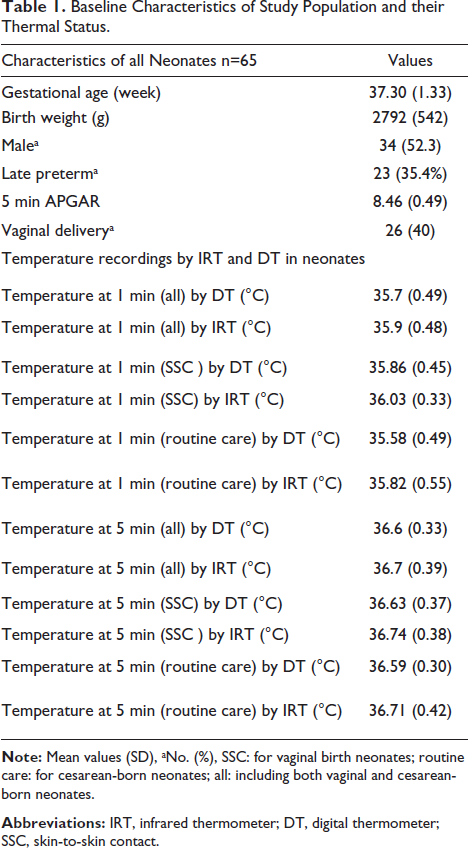
During the study period, a total of 97 neonates at gestational age ≥34 weeks were delivered, and 32 were excluded (3 maternal complications, 5 multiple pregnancies, 12 needed resuscitation, 10 had respiratory distress, and 2 had congenital malformations). A total of 65 singleton neonates underwent simultaneous temperature monitoring with DT and IRT; 26 (40%) were given SSC after vaginal delivery. A total of 130 paired temperature readings were obtained in 65 neonates, of which 79 paired were hypothermic by DT readings. The baseline neonatal characteristics and thermal status are depicted in Table 1.
Baseline Characteristics of Study Population and their Thermal Status.
Temperature recording with IRT showed good reliability with DT (ICC = 0.859, p < .001); and in BA analysis, the bias (SD) between DT and IRT was –0.16 (0.42)°C and 96.9% of the data points remained within both arms of BA analysis. During hypothermia (n = 79 paired observations), IRT showed good reliability with DT (ICC = 0.778, p < .001), and the bias (SD) between DT and IRT was –0.28 (0.42)°C.
For vaginal-born babies during SSC (n = 52 paired), the ICC between DT and IRT was 0.881, P < .001, and the bias (SD) was –0.14 (0.33)°C; and for the cesarean neonates, the ICC between DT and IRT was 0.846, P < .001. and the bias (SD) was –0.17 (0.47)°C.
Discussion
This study showed good reliability between IRT and DT in healthy neonates immediately after birth. The average difference (bias) between them is acceptable for clinicians, but there is a wider LOA in Bland-Altman’s analysis. To the best of our knowledge, this is the first study to detect the accuracy of IRT in temperature measurement in neonates in the delivery room.
Previous studies assessed the accuracy of IRT outside of the delivery room, in neonatal intensive care units.13–17 Duran et al. and De Curtis et al. validated the IRT in preterm neonates <1500 g and neonates born at 25–41 weeks gestational age, respectively.13, 14 Whereas Can et al., Uslu et al., and Smith et al. demonstrated against the utility of IRT for sick neonates.15–17 The device’s precision was influenced by multiple factors, including birth weight, environment temperature, and type of ventilator support used. 17
In our study, IRT at the forehead overestimates axillary site temperature readings, similar to the majority of previous studies.13, 15, 16 However, Smith et al. found that IRT at the forehead underestimates DT temperature readings in general, overestimates DT under radiant warmer, and underestimates DT during routine cot care. 17 Overall, the bias temperature in BA analysis can help clinicians determine the average difference between DT and IRT; and a wider LOA demands further innovation in the IRT device. The average difference between DT and IRT was greater, and the reliability between both methods of temperature reading decreased during hypothermia. It could be explained by subcutaneous peripheral vasoconstriction during hypothermia, the site from which heat is radiated and measured by the IRT device.
IRTs could measure temperature by detecting the infrared energy emitted by the different body sites, such as the temporal artery, forehead, and foot area, while DTs typically use a metal probe to measure temperature orally, rectally, or axillary (under the armpit). The temporal artery sites provided better accuracy than the forehead in one study, 16 but due to the limited area of the temporal artery, the neonate’s forehead may be the preferred site in a well-wrapped neonate in the delivery room or at any point in postnatal care. In Duran et al., a better behavioral state and less pain were found during IRT temperature recording than DT from the axillary site. 13
We acknowledged our study limitations by taking a small sample size from a single centre. We enrolled only vigorous late preterm and term neonates after the practise of delayed cord clamping, where a better hemodynamic state was presumed. In future studies, the utility of IRT for extreme preterm neonates will need to be assessed, as those require multiple strategies to prevent hypothermia. Similarly, the accuracy of IRT needs to be evaluated for asphyxiated neonates, who are vulnerable to the harmful effects of hyperthermia.
The device recommended to measure neonatal temperature should be precise and reliable. Hence, IRT should not replace DT to confirm hypothermia; rather, the use of IRT may avoid the repeated use of DT. In conclusion, IRT may be used for serial temperature monitoring in delivery room care for the prevention of hypothermia, prioritizing during SSC in late preterm and term neonates. As IRT provides quick and non-contact temperature measurements, it may be preferred when dealing with a newborn who may be fussy or restless.
Authors’ Contributions
SKP: Conceptualization, critical inputs to manuscript writing, and supervision. SSB: Principal investigator, analysis, and manuscript writing. VSH: Data collection and manuscript writing. CJ: Data collection and manuscript writing All authors approved the final version of the manuscript, and are accountable for all aspects related to the study.
Data Availability
The data that support the findings of this study are available and can be provided by the corresponding author, based upon reasonable request.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
The institutional Ethics Committee of the Kalinga Institute of Medical Sciences, KIIT University has approved the study: KIMS/KIIT/IEC/876/2022, dt. 22/04/2022.The patient’s identity is not exposed in this study; hence individual patient consent was not taken for publication.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.