
Abstract
Respiratory distress syndrome (RDS) is the most common major morbidity in preterm infants. The recent 6th edition of European consensus guidelines (2023) on RDS gives comprehensive care pathways for management of this vulnerable population based on updated evidence until the end of 2022. The current update also aims to highlight the major updates from the previous version (2019) and to compare the surfactant and non-invasive respiratory support guidelines from the National Neonatology Forum, India.
Preterm birth, as defined by birth prior to a 37- week period of gestation, is the leading cause of neonatal mortality and the second leading cause of under-5 mortality. 1 Respiratory distress syndrome (RDS) is the most common major morbidity in preterm infants. The recent 6th edition of European consensus guidelines (2023) on RDS 2 gives comprehensive care pathways for the management of this vulnerable population based on current evidence up to the end of 2022. This article aims to highlight the major updates from the previous version (2019) 3 (Table 1) and to compare the surfactant and non-invasive respiratory support guidelines from the National Neonatology Forum (NNF), India.4, 5
Updates in European Consensus Guidelines for the Management of Respiratory Distress Syndrome.
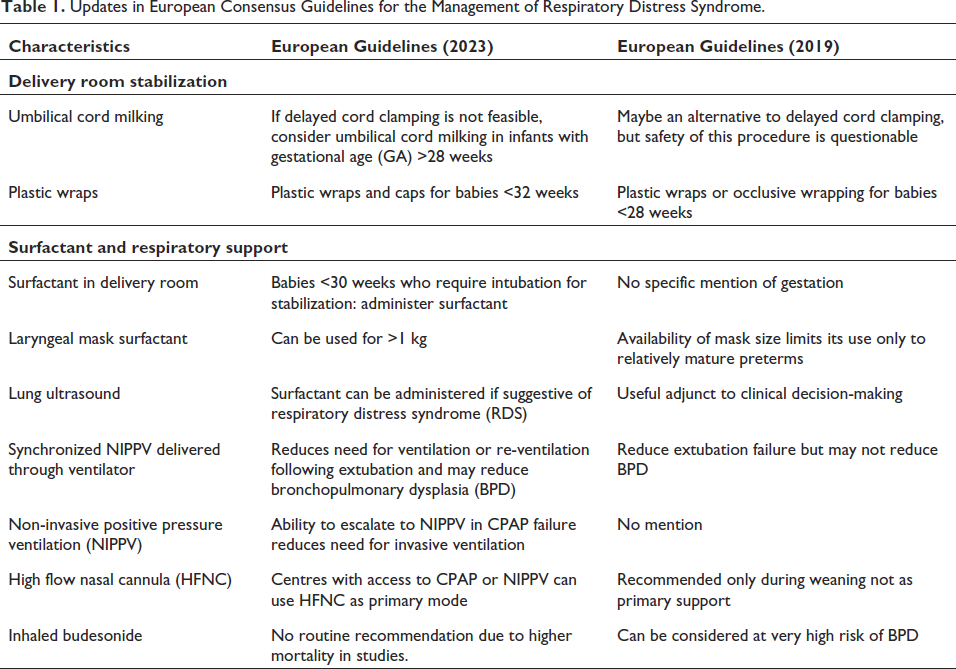
The following recommendations have been continued, as in the previous version: intra-uterine transfer of high-risk pregnancies < 30 weeks, single course antenatal steroids <34 weeks, single repeat course <32 weeks, MgSO4 <32 weeks for fetal neuroprotection, short term tocolytic use to allow completion of corticosteroids or intrauterine transfer, delayed cord clamping for 60 seconds, preference over T piece than bag and mask, FiO2 targets for managing preterms, LISA, early rescue surfactant when FiO2 >30% and CPAP pressures ≥6 cm H2O, oxygen saturation targets (90–94%), lung-protective strategies like volume-targeted ventilation, permissive hypercapnia, early caffeine, caffeine for extubation, short tapering dose of dexamethasone to facilitate extubation for ventilation beyond 1–2 weeks, selective opioid analgesia, enteral feeding, optimum parenteral nutrition, judicious antibiotics, optimum blood pressures, expectant management of PDA, and thresholds for PRBC transfusion.
Major implications of the guidelines in the Indian scenario NNF, India, has published the Clinical Practice Guidelines (CPG) on non-invasive respiratory support (January 2020) and surfactant replacement (December 2021). Following are the differences:
CPAP initiating pressures: NNF CPG,
4
based on evidence comparing lower initial pressure (≤5 cm H2O) versus higher initial pressure (>5 cm H2O), has recommended lower initial pressures (5 cm H2O) as they have similar clinical outcomes with concerns of increased risk of pneumothorax with pressures of 8 cm. Although starting at 6 cm pressures may have the advantages of better splinting of the airways, higher functional residual capacity, and better lung inflation as per European guidelines,
2
it is prudent to start at 5 cm and gradually hike respiratory support based on the clinical situation to reduce air leaks in our settings. Prophylactic surfactant for preterm babies requiring intubation in the delivery room: As such, prophylactic surfactant and the minimum gestation of its administration are not mentioned by NNF
4
or European consensus.
2
NNF CPG
4
recommends surfactant if preterm <28 weeks get intubated during resuscitation in the delivery room. While European guidelines
2
have extended until 30 weeks based on subgroup analysis of the lesser risk of mortality and chronic lung disease in this population,
6
in the current scenario, the minimum gestational age for delivery room surfactant in babies requiring intubation should be based on the unit’s resuscitation protocol and parents’ decision for resuscitation or comfort care. Laryngeal mask airway (LMA) to deliver surfactant: LMA requires less technical skill and is relatively easy to implement in large-scale resource-limited settings compared to both intubation and LISA. NNF CPG
4
has recommended LMA only during research contexts in less than 37 weeks. While European guidelines
2
have recommended LMA for surfactant administration in babies >1 kg based on recent evidence of non-inferiority to INSURE,
7
NRP 2020 guidelines
8
recommend using LMA for resuscitation in neonates equal to 2 kg. Late preterm population: NNF CPG
4
recommends surfactant administration at FiO2 >40% and PEEP ≥7 cm H2O based on 3 RCTs, which show reduction in air leaks, need for mechanical ventilation, and persistent pulmonary artery hypertension. European guidelines have not made any separate recommendations for this specific group of neonates. Repeat dose of antenatal steroids: NNF guidelines
4
doesn’t recommend repeat doses of steroids. However, European
2
and recent WHO guidelines
9
recommend repeat dosing for anticipated preterm delivery if administered 1–2 weeks earlier in less than 32 and 34 weeks, respectively. Umbilical cord milking: Both IAP
10
and NRP resuscitation guidelines
8
have made no recommendation regarding umbilical cord milking as a placental transfusion strategy. Until further evidence is available and recommendations are made by standard resuscitation programs, umbilical cord milking cannot be advised as a routine strategy in neonatal resuscitation.
In conclusion, although the recommendations from the latest European guidelines are contextual and restricted to developed nations, many are still applicable or can be adapted to Indian scenarios for optimal outcomes in preterms with RDS. With evolving evidence, the update to the existing CPG will bring in newer recommendations in years to come.
Author Contributions
AC conceptualized the draft, did a literature search, and wrote the first draft. AA contributed to the review of the literature and drafted the initial manuscript. TS provided critical inputs in the manuscript and approved the final manuscript. She was the guarantor of the manuscript and provided critical inputs in the manuscript and approved the final manuscript. All the authors approved the final version as submitted.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Not applicable.