
Abstract
Background
Survival of preterm babies has improved and the focus now is on intact survival. Early detection of developmental delay is crucial so that diagnostic-specific early intervention can be commenced to optimize neuroplasticity.
Objective
Primary: To assess the neurodevelopmental outcome by measuring preterm infants’ mean composite score for cognition, language, and motor skills. Secondary: To calculate the degree of developmental delay.
Study design
A Cohort Study.
Participants
Preterm neonates.
Intervention
Bayley-III assessment done between 18 and 42 months.
Results
Seventy preterm neonates were assessed between 18 and 42 months of age. They were divided into two groups based on gestational age. Mean composite score for cognition (<30 weeks = 79.84 ± 7.88 and >30 weeks = 86.32 ± 9.28; 95%CI: 81.16–85.55), language (<30 weeks = 79.16 ± 11.55 and >30 weeks = 89.37 ± 11.61; 95%CI: 81.90–87.70), and mean Motor scores (<30 weeks 81.69 ± 17.82 and >30 weeks = 89.84 ± 10.46; 95%CI: 82.59–89.63) were statistically significant. There was more than half the standard deviation deficit of composite scores between the two groups. Eighty-one percent had a moderate delay in cognition in the <30 weeks group as compared to 65.8% in >30 weeks. Similarly, for language and motor scores, 43.8% and 31.3% had a moderate delay in <30 weeks as compared to 39.5% and 42.1% for >30 weeks, respectively.
Conclusion
Higher composite scores were observed among infants >30 weeks gestation. There was more than half a standard deviation deficit in composite scores among those <30 weeks of gestational age. The most affected was the language component.
Abbreviations
ELBW: Extremely low birth weight
VLBW: Very low birth weight
NICU: Neonatal Intensive Care Unit
Introduction
Advances in foetal medicine, perinatal practices, and neonatal care have led to improved survival of high-risk infants, especially the extremely preterm infants in India. However, survival without morbidity remains a challenge. The level of care available at the location of delivery is an extremely important consideration while caring for babies born at <35 weeks. During the past two decades, countries with active perinatal care at extremely low gestation have reported improved outcomes for infants born around 22–25 weeks. Despite these improvements, survival without neurodevelopmental impairment at 2–2.5 years was 20% in the USA for infants born at 22–24 weeks gestation, and 34% and 42% in England 1 and Sweden, 2 respectively, for infants born at 22–26 weeks gestation.
However, infants born moderately preterm represent a larger proportion of preterm births accounting for more children with motor, cognitive, or behavioural deficits and learning disabilities.3, 4 This population has been poorly investigated. Knowledge of specific developmental domains affected at preschool age could lead to targeted intervention and prevention of later disabilities, in a timely intervention has a positive influence on cognitive outcomes in infancy.5, 6
To improve long-term neurodevelopmental outcomes for these infants, it is important to identify the early markers of risk for these later ‘high prevalence, low severity’ deficits of cognitive functioning. We aimed to assess the neurodevelopmental outcome of these preterm infants discharged from our NICU using the Bayley Scale of Infant and Development III (BSID-III).
Methods
The study was conducted at a tertiary care Hospital between 2017 and 2019.
All preterm neonates who were admitted to NICU were eligible for the study. The infants were categorized into two groups. Group 1 included newborns who were <30 weeks of gestation at birth and Group 2 consisted of newborns who were >30 weeks of gestation at birth. Infants were enrolled after obtaining informed written consent from both or either parent.
The case records were used to collect demographic data, the course in the NICU, complications, and status. A single observer to avoid inter-observer variability completed a Neurodevelopmental assessment using Bayley Scales of Infant development. The BSID-III assessment was done by administering standardized test tasks to a child and comparing the resulting test score to the test score distribution of a norm group. The hospital ethics committee approved the study.
For sample size calculation, we hypothesized that there would be a likelihood of ½ standard deviation deficit in measured composite score in cognition, language, and motor skills in neonates <30 weeks when compared to neonates >30 weeks at birth. Most of the available studies have taken one standard deviation difference. One standard deviation suggests a score difference of 15. We have taken half standard deviation deficit (a score difference of 7.5) considering the Flynn effect and to detect mild delays, which might go unnoticed.
Statistical Analysis
Descriptive and inferential statistical analyses were used. Results on continuous measurements are presented on mean ± SD (Min-Max) and results on categorical measurements are presented in Number (%). Significance was assessed at a 5% level of significance. Student t-test (two-tailed, independent) was used to find the significance of study parameters on a continuous scale between two groups (Intergroup analysis) on metric parameters. Leven’s test for homogeneity of variance was performed to assess the homogeneity of variance. Chi-square/Fisher Exact test was used to find the significance of study parameters on a categorical scale between two or more groups, the non-parametric setting for Qualitative data analysis. Fisher Exact test was used when cell samples were small. The Statistical software namely SPSS 18.0 and R environment ver.3.2.2 were used for the analysis.
Results
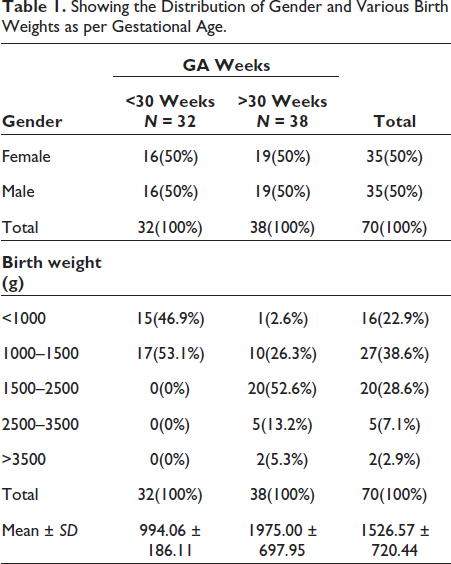
During the study period, a total of 70 ex-preterm babies were assessed who were between 18 and 42 months of corrected age. Thirty-two babies were <30 weeks which constituted 45.7% and 38 babies were >30 weeks, which was 54.3%. There was an equal distribution of males and females among the two groups. The demographic details as per gestation, birth weight and corrected age at the time of assessment are shown in Tables 1 and 2.
Showing the Distribution of Gender and Various Birth Weights as per Gestational Age.
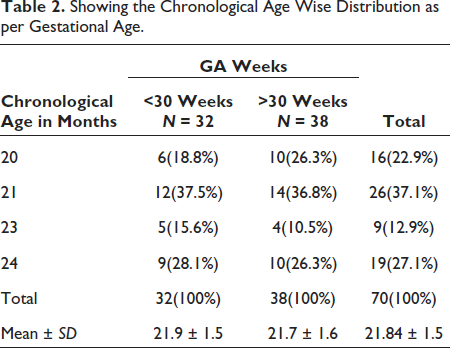
Showing the Chronological Age Wise Distribution as per Gestational Age.
The mean composite score for cognition was 79.84 ± 7.88 and 86.32 ± 9.28, respectively, in Groups 1 and 2 with a 95%CI of 81.16–85.55, which was statistically significant. The mean language score was 79.16 ± 11.55 and 89.37 ± 11.61, respectively, with a 95%CI of 81.90–87.70, which was statistically significant. The mean motor scores were 81.69 ± 17.82 and 89.84 ± 10.46 with a 95%CI of 82.59–89.63, which was statistically significant. There was more than half the standard deviation deficit of the composite scores of <30 weeks as compared to >30 weeks (Table 3).
Showing the Composite Score as well as Individual Domain Scores Depending Upon the Severity Obtained by BSID-III—Comparison in Two Groups.
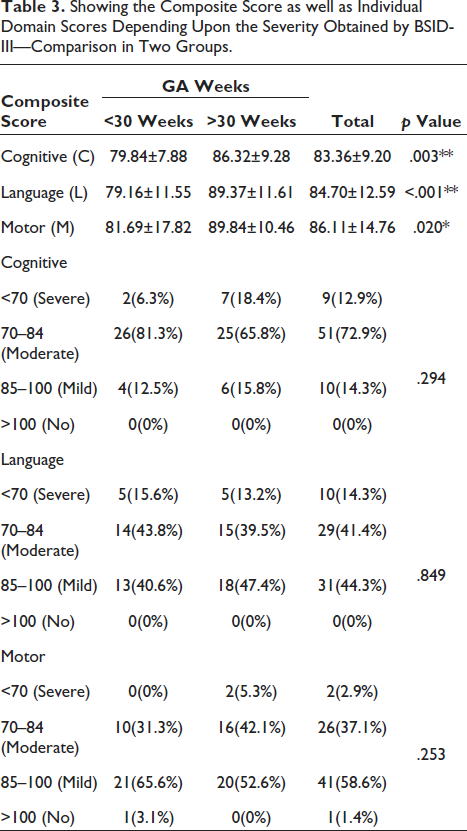
Composite scores were divided into <70, 70–84, 85–100, >100 to assess the severity of the delay. Using the Chi-Square/Fisher Exact Test, 81.3% had a moderate delay in cognition in the <30 weeks group as compared to 65.8% in >30 weeks. As for language scores, 43.8% had a moderate delay in <30 weeks as compared to 39.5% for >30 weeks. Regarding motor skills, 31.3% had a moderate delay in <30 weeks gestation and 42.1% in >30 weeks. However, none of these were statistically significant.
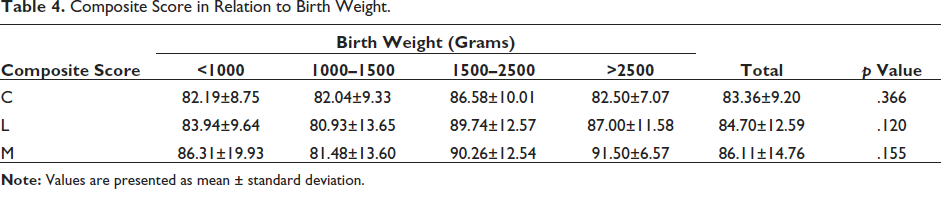
Mean composite score for cognition using the ANOVA test was 82.19 ± 8.75 and 82.04 ± 9.33 for ELBW and VLBW, respectively. Mean composite score for language was 83.94 ± 9.64 and 80.93 ± 13.65, respectively, for ELBW and VLBW, respectively. Mean composite motor scores for ELBW and VLBW, were 86.31 ± 19.93 and 81.48 ± 13.60, respectively. There was no statistically significant difference between the composite scores with respect to birth weight (Table 4).
Composite Score in Relation to Birth Weight.
Mean composite score for cognition using the ANOVA test was 87.14 ± 5.67 and 83.47 ± 9.53 for SGA and AGA, respectively. Mean composite score for language was 76.14 ± 2.27 and 84.88 ± 12.99 for SGA and AGA, respectively. Mean composite motor scores were 86.71 ± 12.71 and 85.71 ± 15.52 for SGA and AGA, respectively. There was a statistically significant difference between the language composite scores with respect to gestational weight, lowest score obtained in SGA babies with a mean of 76.14 ± 2.27 (Table 5).
Composite Score in Relation to SGA/AGA/LGA.

Discussion
Understanding neurodevelopmental patterns are necessary since sensitive identification of cognitive, language, and motor delay is required for early interventions. Previous research has revealed that preterm infants demonstrate cognitive, language, and motor delays during the first postnatal year and into adolescence. 7 In our study, the mean composite score for cognition, language, motor skills were significantly higher in >30 weeks gestation infants. Our findings support our research hypothesis that there was more than half the standard deviation deficit of the composite scores in <30 weeks as compared to >30 weeks. The greatest deficit was in language followed by motor composite scores. There was no significant difference between the composite scores concerning gender.
ELBW infants had lower cognitive scores, whereas VLBW infants had lower language scores. A severe cognitive delay was observed among >30 weeks of gestational age infants. Severe language delay was observed mostly in <30 weeks gestation while the majority of >30 weeks gestation had a mild delay in language. A severe motor delay was seen mostly in >30 weeks gestation and the mild motor delay was common among <30 weeks gestational age infants. Among the SGA babies, composite language score was the most affected. AGA and LGA babies had their cognitive scores most affected. The mean composite score for cognition, language, motor skills was significantly higher in >30 weeks gestation. The greatest deficit was for language followed by motor composite scores. The difference was least for the cognitive composite score.
Bayley-III Cognitive Index consists of a greater number of items with simpler and more graded tasks, so it is easier for a child to gain a higher score. A similar study by Sung-Ho Ahn et al. 8 and Bode et al. 9 also had better mean composite cognitive scores among in >28 weeks gestation at birth at two years of age. This may be due to later age at assessment and this study included only extreme preterm. Lower the gestation, lower was the composite scores, which is also the case in our study. ELBW infants had a better mean composite score for language and motor skills with a lower mean composite score for cognition compared to VLBW. Anderson et al. 10 found in their study, one-third of the ELBW group exhibited cognitive delay, and even higher proportions had language and motor delay. Mansson and Stjernqvist 11 found a higher mean composite score for cognition, language, motor skills among ELBW infants. Most of the ELBWs in our study were sick at birth with sepsis and hemodynamic instability, which could explain their later poor cognition as compared to other studies.
The Bayley-III may identify fewer infants with language impairment because it separates the receptive and expressive subscales, so a child can reach a higher score by bypassing all the receptive items even if the production is compromised. VLBWs had the lowest language composite score while Cognitive and motor scores were affected to a lesser extent. Fernandes et al. 12 also found greater language delay (29.3%), with a low proportion of abnormal motor and cognitive scores (6.9%) for both outcomes similar to our study. Ballot DE et al. 6 showed that in VLBW infants, language scores decreased significantly after one year. According to Sung-Ho Ahn et al. 8 VLBWs were significantly related to lower cognitive, language, and motor composite scores.
In our study, severe delay in cognitive and motor composite scores was higher among >30 weeks. This may be because these babies were very sick at birth, with sepsis, longer duration of ventilation, longer hospital stay. Severe language delay was commonly noted in <30 weeks. Lower gestation was associated with poor language development. Anderson et al. 9 found 1%, 2% and 3% severe delays in cognition, language, motor skills in extreme preterm. Sung Ho Ahn et al. 8 most commonly found a severe cognitive delay in <28 weeks, severe language delay was more common among >28 weeks gestation, whereas they found an equal number of severe motor delay in both groups. However, none were statistically significant. The majority of the babies in our study had a moderate delay in cognition, mild to moderate delay in language, mild motor delay. Cognition was affected due to the degree of sickness.
There are many strengths of this study. The sample size was adequate. The most recent developmental tool available was used which avoided the Flynn effect. BSID-III enabled a better evaluation of the three principal domains of development. Antenatal details including accurate determination of gestational age, the reason for prematurity, neonatal morbidities were available. It was a single-person assessment with no inter-observer variability. The age range at the time of assessment was not wide. Another important strength of this study was the importance of a follow-up program for NICU graduates to help care providers and parents in planning interventional programs. There is a paucity of data on BSID III in Indian literature. We believe that our study has advanced this under-researched topic.
Our study had some limitations. Since this was a retrospective cohort, we were not able to assess the growth and neurodevelopment of these infants sequentially from birth. Also, some of the antenatal details and neonatal course were not available. As this study was conducted at a private hospital, generalization to public sector hospitals may be limited.
Conclusion
Our study showed a significantly better composite score among infants >30 weeks gestation at the time of birth. There was more than half the standard deviation deficit in composite score among <30 weeks gestational age infants. Most affected was language. The lowest scores were obtained among VLBW infants. Motor scores were significantly affected in this population. ELBW infants had better language and motor scores as compared to VLBW infants. However, the cognitive score was mostly affected in this population. SGA babies had poor language development and better cognitive development.
Key messages
Preterm babies are known to have some form of developmental delay. Bayley scale of Infant and Toddler development is one of the scales used for neurodevelopmental outcomes of preterm infants worldwide.
This is the first report of long-term follow-up of preterm using Bayley scales in India.
Different domains such as cognitive and language are affected in preterm babies based on the gestation.
Footnotes
Acknowledgement
I thank my teachers who were instrumental in guiding me to do this study from start till completion. I thank my wife and family who supported me during this time period.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the hospital’s institutional Ethics Committee. There are no ethical concerns.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Guidelines on patient consent has been met. Informed consent was taken from the parents of newborns.