
Abstract
Background and Rationale
Successful transition to oral feeding is a crucial milestone for preterm infants. Our unit uses a pragmatic 5-point checklist to assess the readiness of preterm infants for oral feeding.
Methods
This prospective observational study included very preterm infants (<32 weeks at birth). They were assessed for readiness at ≥33 weeks postmenstrual age (PMA), and pre-defined physiological stability for oral feed readiness. Oral feeds were started when all parameters of the checklist were satisfied. The proportion of those who succeeded (measured as no apnoea/choking on oral feed for 48 hours) after commencement of transitioning from orogastric to oral feeds was measured, weight gain over 1 week and PMA at attainment of full oral feeds were also analysed.
Results
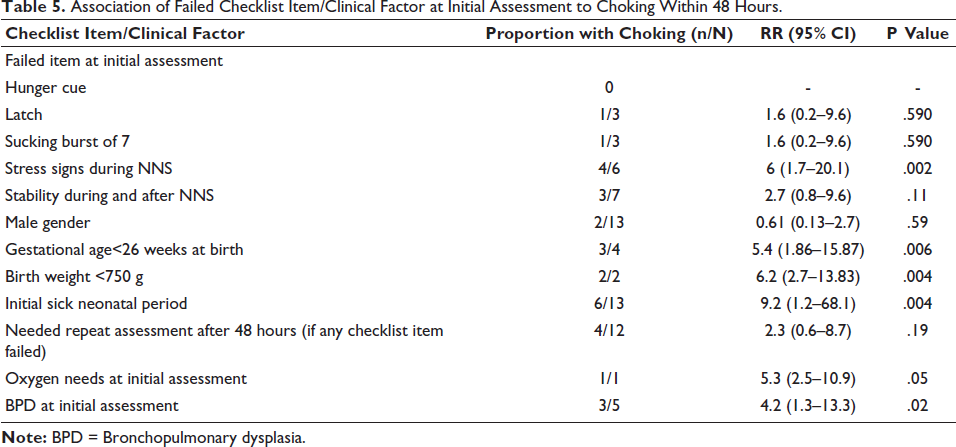
Thirty-three eligible neonates were included, of which 26(78.8%) had no apnoea/choking within the first 48 hours of transition. Twelve infants needed to be reassessed since they ‘failed’ the first time over. The median PMA of attainment of full oral feeds was 34(34,37) weeks, weight gain over 1 week of oral feeds was 145(117,170) g. Among risk factors analysed for choking, stress signs during non-nutritive sucking [RR6(1.7–20.1), P = .002], those with initial sick newborn period (FiO2 need>0.3 beyond 72 hours/any inotrope need)[RR9.2(1.2–68.1), P = .004], and bronchopulmonary dysplasia (BPD) [RR4.2(1.3–13.3)], P = .02] were significant.
Conclusion
The transition to oral feeding of preterm neonates can be assessed by a practicable, easy-to-use scale; it predicted success in 78.8% infants. Those who were initially sick exhibited stress signs on assessment and BPD infants can be transitioned with due caution and monitored for choking events more closely.
Introduction
Successful transition to full oral feeding is an important milestone for preterm infants. It is a major discharge criterion. Initiation or advancement of oral feedings in an infant who is physiologically unstable or developmentally immature may result in poor fluid management or aspiration, behavioural distress, unstable heart rate, hypoxia during feedings, increased energy expenditure, poor weight gain, and even failure to thrive and readmissions.1, 2
On the other hand, undue delay in the transition to oral feeds from gavage feeds can increase the duration of hospitalisation and its associated problems. Inherent functional immaturity of coordinating sucking, swallowing, and breathing is known to improve with increasing postmenstrual maturity. 3 However, the relationship between age alone and functional maturity of oral feeding skills is not always linear. 4 Each infant develops feeding readiness and skills along different timelines that depend on individual morbidities, growth and development patterns. 5 Each infant would be unique, hence transition plans would need to be individualised based on several factors.
Several instruments are described in the literature to assist clinicians in measuring nutritive sucking behaviours and quantify oral feeding performance like The Early Feeding Skills Assessment (EFS), Neonatal Oral-Motor Assessment Scale (NOMAS), Premature Oral Feeding Readiness Assessment Scale (POFRAS), Preterm Infant Breastfeeding Behaviour Scale (PIBBS) etc. Most of these have several items, are complex, time-consuming and need training. Very few studies have objectively assessed their success rate and practicability in the clinical setting. Our unit has been using a 5-point oral feeding readiness assessment checklist (RAC) designed after a literature search, deductive processes, unit discussions for essentiality, relevance of items, checking for overlap in pre-defined domains and feedback from the team. It is primarily based on an intuitive selection of aspects from previously published scales. This study aimed to measure systematically, the proportion of those infants who were assessed as ready by the unit’s checklist (modified from various scales); who succeeded in oral feeding attempts.
Materials and Methods
This prospective observational study was done in a level IIIb (National Neonatology Forum India) accredited unit, over a period of six months.
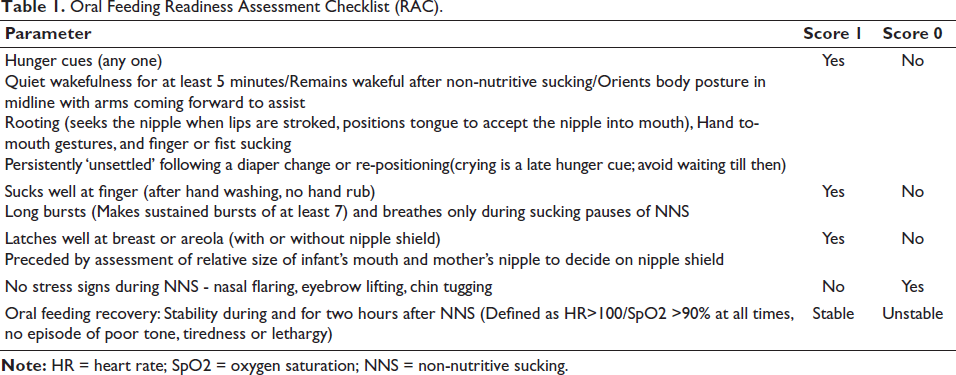
The unit has in place, written protocols for the care of very preterm infants, enteral and parenteral nutrition, oromotor stimulation and early parent participation. 6 The study included preterms delivered at <32 weeks gestation. Instead of using a particular postmenstrual age (PMA) as a criterion for initiation of oral feeding attempts, we administer a pragmatic oral feeding readiness assessment checklist (RAC), modified from various available feeding scales. This is conducted when the infant is at least 33 weeks PMA and hemodynamically stable (all of: (a) Full enteral feeds, (b) Off respiratory supports or high flow nasal canula with <0.3 FiO2 need, (c) No apnoea requiring stimulation for more than 48 hours). The RAC is elucidated in Table 1.
Oral Feeding Readiness Assessment Checklist (RAC).
The initial sick neonatal period was defined as requirement of invasive ventilation with >0.3 FiO2, or inotrope need, beyond 72 hours of life.
Oral feeds were started when all five parameters of the RAC were satisfied (score = 5). A repeat test was done after 48 hours if previous attempt failed. Of those who passed the RAC, proportion of infants with successful transition to oral feeding (no choking within first 48 hours of commencement of oral feeds) after passing the checklist was determined. Escalation of oral feeds was done gradually based on safe, effective swallowing of offered volumes each time, under hemodynamic monitoring. The remainder of the prescribed milk quantity was administered by feeding tube. Once the infant took adequate (prescribed) volumes orally for a whole day-night consistently, the feeding tube was removed and considered as achieved full oral feed at that point. As secondary objectives, weight gain over 1 week after full oral feeds, PMA at attainment of full oral feeds and risk factors associated with unsuccessful transition were assessed. Weight was measured using the scale in the step-down unit (machine with 5 g accuracy).
The sample size was calculated assuming that 90% of the preterm babies would successfully transition to oral feeds after passing the RAC. This presumed proportion was based on the unit’s previous observations. (unpublished). To estimate the expected proportion with 10% absolute precision and 95% confidence, 33 infants needed to be studied. Data collected was tabulated using MS Excel and analysed using SPSS version 20.0. Results on categorical measurements were presented as proportions, continuous measurements were presented as median and inter-quartile range (IQR). The association between the categorical variables were assessed using Fisher’s exact test. A P value <.05 was considered to be statistically significant. Clearance from the Institutional Ethics Committee was obtained. Parental consent was sought for collection of de-identified data. No interventions were planned specific to the study.
Results
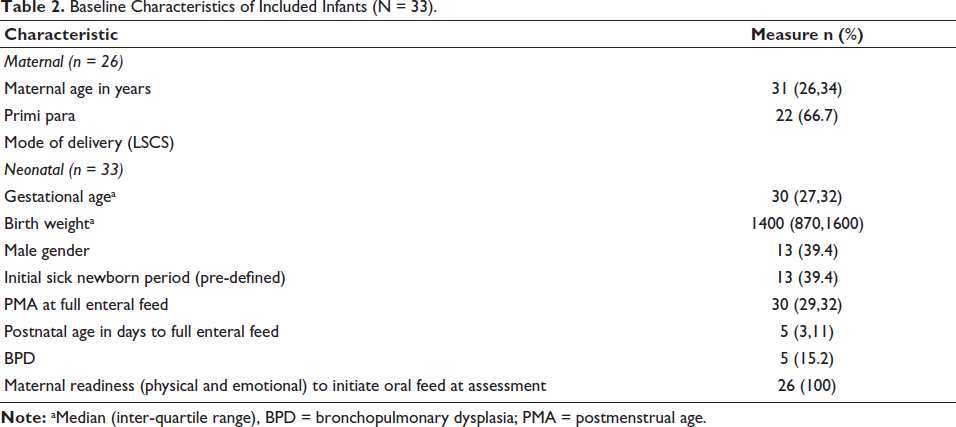
Thirty-three infants who fulfilled the inclusion criteria were enrolled after exclusion (four were excluded: three expired and one was transferred out to another unit before completion of care). Their baseline characteristics are described in Table 2.
Baseline Characteristics of Included Infants (N = 33).
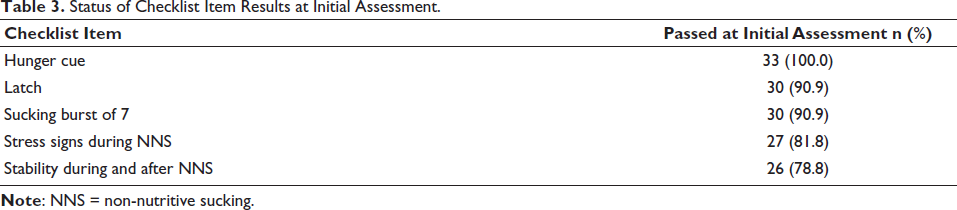
As elucidated in Table 3, all 33 infants had good finger suck on initial assessment.
Status of Checklist Item Results at Initial Assessment.
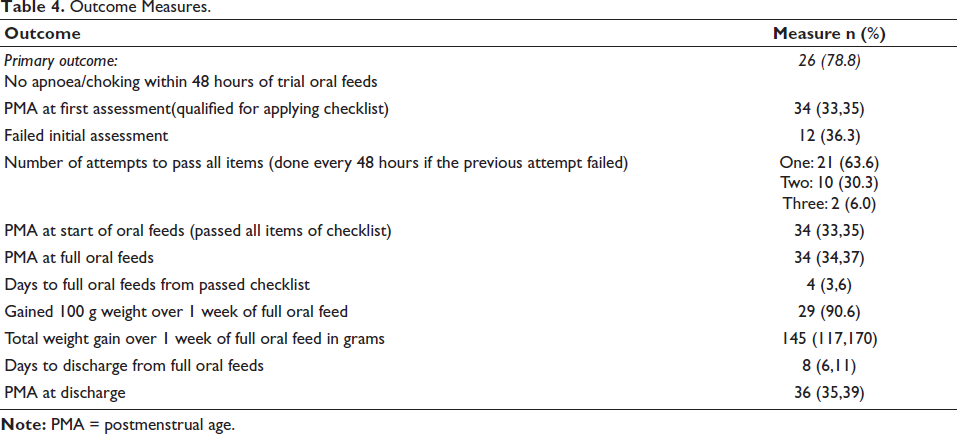
78% of infants who passed the RAC feeding checklist with a score of 5, succeeded in transitioning to oral feeds measured as no apnoea/choking within 48 hours of oral feeding trial. Twelve infants required reassessments for failed first attempt at RAC. Median PMA at start of oral feeding was 34 weeks and a significant percentage (90.6%) had adequate weight gain (Table 4).
Outcome Measures.
Stress signs during NNS, high level of initial sickness and presence of BPD were found to be statistically significant in leading to failure of safe transition to oral feeding after passing feeding checklist (Table 5).
Association of Failed Checklist Item/Clinical Factor at Initial Assessment to Choking Within 48 Hours.
Discussion
More than three-fourths of very preterm infants assessed for oral feeding readiness by the 5-point scale could be safely transitioned from orogastric feeds.
It seems rational to assume that oral feed acceptance without adverse events would depend on factors other than postmenstrual maturity alone. The physiology of mechanisms necessary for feeding would likely depend on clinical course, associated co-morbidities and the then clinical status. Our criteria for first administering the RAC included clinical correlates of these factors. Pineda et al. reported 50% questionable feeding performance even after they were assessed at their term equivalent age using the Neonatal Eating Outcome Assessment score. 7 We institute measures to optimise oromotor maturity from very early in postnatal life. 8
Early parent participation which is an integral strength of our unit is an intuitive practice that can have many intangible benefits. 6 Morag et al. employed the parent-guided responsive feeding for oral transition in infants born <32 weeks gestation 9 ; the authors demonstrated that these infants reached full oral feeding at a median gestation of 34.28 weeks; which is similar to our finding.
Once the safety of oral feeding initiation is reasonably established, demand or cue-based feeding may be more successful than clock hour-based methods. McCormick et al. concluded that cue-based feeding improved infants’ nutrient intake. 10 Crosson, Puckett et al. also reported good weight gain during cue-based feeding. 11 Our study documented a median weight gain of 145g over 1 week of oral feeding when oral feeding was started after an assessment of readiness.
Studies by Rosemary White-Traut et al., Lau C et al., and Dodrill P et al. showed that preterm infants who had high morbidity scores based on POPRAS (The Problem Oriented Perinatal Risk Assessment System) during their initial days had a statistically significant increase in days to full oral feeding which is in agreement to finding in our study.3, 12, 13 Non-Nutritive Sucking assessment scores have been studied as a measure of oral feeding readiness.14, 15 In our study, the presence of stress signs during NNS was a predictor of failure to oral transition.
Studies by Gewolb and Vice 16 and Mizuno et al. 17 support the finding in our study that BPD is a significant medical complication that significantly delays the initiation and advancement of oral feeding in preterm babies.
We admit that we do not have a comparative arm to strengthen the utility of the RAC in assessing safety of trial oral feeds and predicting successful transition. Since the practice is part of unit protocol, it would be incorrect to have another arm. The sample size is small, but the systematic and prospective study design might negate this limitation. The primary outcome fell short of the presumed success of 90% used in the sample size calculation. Recommendations for use of this checklist in practice would require a large validation study. The lack of a gold standard is a deterrent to validation. Moreover, ours is a checklist where all parameters need to be met before oral feeds are commenced, it is not a score with ranges. Hence statistical tests to draw cut-off points for prediction of outcome would not be appropriate. The ease of RAC is its main asset. Our study has some noteworthy strengths. Although choking/apnoea within only 48 hours of start of oral feeds was used as primary outcome measure, we assessed for adequate weight gain over the next 1 week and days to full oral feeding from commencement of transition. These are surrogate markers of successful and safe oral feeding. The mode of oral feeding: direct breastfeeding, paladay, bottle feeding was not separately studied. The unit prefers attempting in that order. The findings can be generalised to similar units.
Conclusion
Using a simple and quick checklist (RAC) is practical; and useful in determining oral feeding readiness in very preterm infants; helping in a safe transition to oral feeding and early discharge. It predicted transition success in 78.8% infants. Success was further supported by adequate weight gain over the next week. Failure of safe oral transition in spite of passing the assessment was associated with initial sickness levels; when stress signs were exhibited on NNS component of RAC; and BPD.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the Institute Ethics Committee (KIMS/IHEC/TP063/2024).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Taken from parents of included infants; study involved only collection of de-identified information. No interventions specific to the study were done.