
Abstract
Background
Calcinosis cutis involves the deposition of calcium salt in the subcutaneous tissues and skin. This is commonly linked to connective tissue disorders or damaged tissues with normal or abnormal calcium/phosphorus metabolism. Iatrogenic cases are also there though rare.
Case Descriptions
Two male neonates born late preterm presented at 20 days (Case 1) and four weeks (Case 2), with firm linear erythematous swellings over extremities. Both neonates had a neonatal intensive care unit (NICU) stay after the birth for prematurity-related issues. Both were administered intravenous calcium during their NICU stay. There were no swellings at the time of discharge in both neonates.
Radiologically, both cases had calcification around the tibia and fibula (Case 1) and deposits in the right upper limb (Case 2). Both cases had normal calcium profiles and a negative sepsis workup. Both neonates improved clinically and radiologically on conservative management.
Management and Follow-up
Both cases were managed conservatively. Follow-up after three months showed complete resolution in Case 1 and partial resolution in Case 2. Regular monitoring is crucial for assessing progress.
Conclusion
Iatrogenic calcinosis cutis can arise from intravenous calcium administration and is generally self-limiting. Healthcare providers must be aware and careful in following up to manage and monitor this condition effectively.
Introduction
Calcinosis cutis is a rare condition and results from abnormal calcium deposition in the skin and subcutaneous tissues. The first case of calcinosis cutis was reported by Virchow in 1855. 1 The disease is of five subtypes, namely calciphylaxis, dystrophic calcification, iatrogenic calcification, idiopathic calcification, and metastatic calcification. Clinical manifestations can vary from debilitating lesions that may involve large areas of the body to localized nodules. Calcifications can develop in damaged or devitalized tissues, even with normal or abnormal calcium and phosphorus metabolism. These calcifications may result in contractures, muscle atrophy, skin ulceration, and infections. The management depends on the type of calcinosis. 2
Case Description
Case 1: A 20-day-old male preterm neonate was brought to the pediatric outpatient department with swelling over his right leg for the past ten days. He was feeding well, afebrile, and hemodynamically stable. Clinically, there was an erythematous cord-like nontender palpable swelling on the right lower leg extending up to the right foot. The baby had received intravenous calcium during his neonatal intensive care unit (NICU) stay of seven days after birth. Metabolic and septic profiles revealed no abnormality.
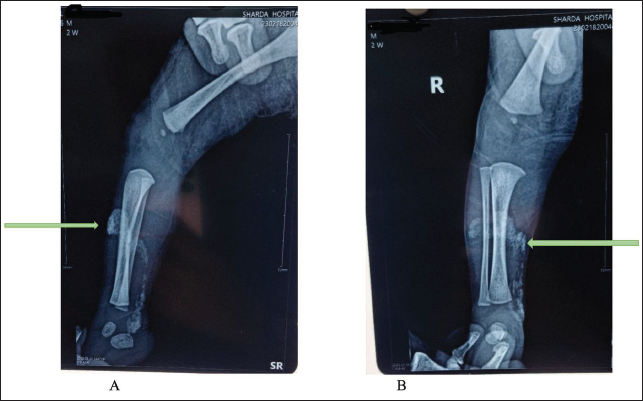
Radiologically, there was a sheet of calcification around both the tibia and fibula extending up to the ankle joint (Figure 1A and B).
(A and B) A Sheet of Hyper-dense Tissue Around the Right Tibia and Fibula (Case 1).
Case 2: A four-week-old male preterm neonate presented with nontender, nonerythematous firm subcutaneous swelling over the right upper limb extending from mid-forearm to mid-upper arm, including cubital fossa. This baby also received intravenous calcium supplementation during his NICU stay. Metabolic and sepsis profiles were normal.
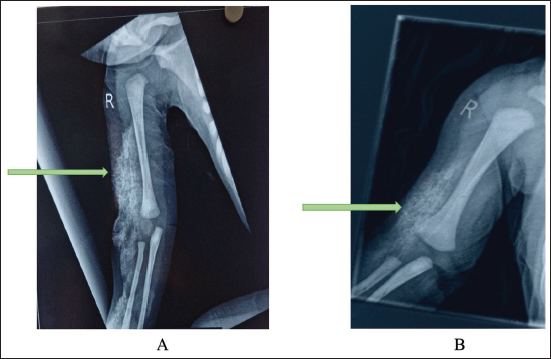
Radiologically, there was a sheet of calcium deposits in the subcutaneous tissues around the humerus and over the radius and ulna with normal bone contours (Figure 2A and B).
(A) Sheets of Calcium Deposit around the Humerus and Both Bones of the Forearm. (B) Partial Resolution of Calcium Deposits (Case 2).
Management
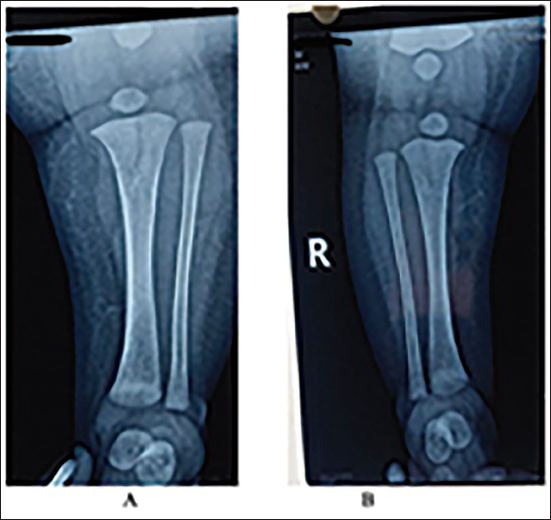
Both cases were managed conservatively. Cases were followed up regularly and showed clinical improvement over three months period. Case 1 had complete resolution of deposits (Figure 3A and B), whereas Case 2 showed partial resolution of calcium deposits (Figure 2).
(A and B) The Complete Resolution of Calcium Deposits (Case 1).
Discussion
Calcinosis cutis lesions are usually asymptomatic and they develop gradually. However, the etiology of the calcification decides the evolution of the lesions. There is usually a history of recent infusion of intravenous calcium in neonates with iatrogenic calcinosis cutis. In most cases, it is due to intravenous administration of solutions containing calcium (calcium gluconate) either prophylactically or as treatment in cases of neonatal hypocalcemia. There is precipitation of calcium salts in the skin and subcutaneous tissue when extravasation of calcium occurs. However, other possibilities like bony lesions, cellulitis and thrombophlebitis, also need to be ruled out. Iatrogenic calcinosis cutis arises secondary to parenteral administration of calcium or phosphate.
In patients showing dystrophic calcification, there might be a trauma that may have led to the initiation of it, or there might be a skin nodule that may have pre-existed, or the patient might have had a pre-existing disease leading to the calcification. In patients with chronic kidney disease, metastatic calcification may be seen in the body. However, idiopathic calcinosis cutis does not occur with either a previous underlying disease or trauma. 3
If the calcium–phosphate product exceeds 70 mg/dL, and there is hypercalcemia and/or hyperphosphatemia, ectopic calcification can occur even when there is no preceding tissue damage. 4
Different theories have been proposed to explain the development of the disease occurrence. The exact pathogenesis of calcinosis cutis is not known. It is postulated that tissue damage along with inflammation causes intravascular activation of clotting factors, release of free fatty acid, and coagulative necrosis. 5 The differential diagnosis of this condition is various autoimmune conditions like systemic lupus erythematosus, dermatomyositis, tumoral calcinosis, and systemic sclerosis. 6
Calcinosis cutis manifests as plaques and nodules which are of various sizes. Initially, the skin appears normal and is soft with no adhesions or pain. Thereafter, the overlying skin adheres to the mass and there is subsequently pain/tenderness redness and swelling. Later, this will secrete a specific calcareous, purulent substance that breaks. The calcium salt that is deposited is mainly amorphous phosphate and also has small amounts of hydroxyapatite and calcium carbonate. 1
Diagnosis and Management
Diagnosis is usually made by plain radiographs. X-rays show extraosseous calcifications in the form of soft tissue swelling and extensive sheets of calcium. This may have a latency period of one to three weeks between calcium administration intravenously and the clinical and radiographical manifestations of iatrogenic calcinosis cutis. 7
Treatment is conservative and consists of observation for complications and pain control.
Further, an increase in calcinosis is prevented by controlling the underlying inflammatory condition. Studies show that the process of calcinosis can be decreased by using drugs like diltiazem, bisphosphonates, and warfarin. 8
Calcium gluconate extravasation injuries can be treated by cold compresses, local injections of sodium cellulose phosphate, sodium thiosulfate or triamcinolone acetonide, and surgical excision with skin grafting if required. 9 Besides, injection ceftriaxone can be also given which has both anti-inflammatory and antimicrobial actions. It binds to calcium and matrix metalloproteinase is inhibited. 10
In most of the cases reported, even without any specific treatment, there is progressive clearing of calcification within eight weeks or resolves completely latest by six months, as in our case. 11
This condition can be prevented by ensuring slow infusion rates, dilution of calcium gluconate infusions, and using a central line for the administration of calcium compounds.
Conclusion
Calcinosis cutis is the condition in which there is accumulation of calcium salts in the skin and underlying subcutaneous tissues. In both cases, it was iatrogenic calcinosis cutis, which may have been triggered by the administration of calcium intravenously. Pediatricians should be mindful of this condition when administering calcium infusions. It is a self-resolving condition and needs careful supervision and follow-up.
Footnotes
Authors’ Contribution
All the authors helped in patient care (establishing clinical diagnosis, planning of investigations, management, and follow-up) and writing of the manuscript. BTN assisted in the management of cases and review of literature. PY drafted the case reports and collected the material under supervision of RKT and BTN.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Being a case report, ethical approval is not mandatory; however, the informed consent was obtained, though no face or identity of subjects is revealed.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.