
Abstract
Background
Preterm neonates are often born with respiratory distress requiring continuous distending pressure respiratory support. Nasal continuous positive airway pressure (CPAP) devices favor a good outcome when initiated early. In our country, most preterm babies are born in healthcare setups that are not equipped to offer CPAP support at birth. The failure to initiate the appropriate treatment in the initial hours could have cascading effects on the outcome. A portable, low-flow driven, non-electrical device, simple continuous positive airway pressure (SIMPAP) [Patent no. 201841018247—Indian PTO] was developed and tested in an earlier in vitro study. The present study was done to compare the efficacy and safety of SIMPAP against bubble CPAP when used as primary support in preterm respiratory distress syndrome (RDS).
Methods
This was a randomized controlled non-inferiority trial conducted among 60 neonates between 28 and 37 weeks of gestation admitted with respiratory distress. The intervention group was initiated on SIMPAP support, and the control group on bubble CPAP. The outcome measured was the change in saturation oxygen pressure index (SOPI) over 6 h.
Results
The SOPI in the CPAP group was 1.150 (1.070-1.408), and in the SIMPAP group was 1.080 (1.060-1.501). The difference between the SOPI measured at recruitment and 6 h in the CPAP group was 0.020 (−0.001 to 0.213) and in the SIMPAP group was 0.010 (0.000-0.030), P = 0.847. SOPI at the end of 72 h was 1.07 (1.05-1.07) and 1.05 (1.05) in the control and intervention groups, respectively. The complications between the two groups were not statistically significant.
Conclusion
The efficacy and safety of SIMPAP are similar to bubble CPAP in the first 6 h and up to 72 h for treating respiratory distress in preterm neonates.
Keywords
Introduction
Every year, 2.5 crore babies are born in India, of which 35 lakh are premature. One-third of these succumb to illness, contributing significantly to infant mortality. 1 Surfactant deficiency leading to atelectasis results in respiratory distress syndrome (RDS), which is a major cause of death in preterm neonates. 2 Continuous positive airway pressure (CPAP) provides constant distending pressure to keep alveoli open, improving distensibility and reducing the work of breathing. 3 Hence, CPAP is the standard initial treatment for RDS, while oxygen alone is no longer recommended. 4 Early initiation of CPAP is critical for outcomes, and typically, CPAP pressures between 5 and 7 cm H2O are used. 5
Saturation oxygen pressure index (SOPI) offers a comprehensive, non-invasive, objective assessment of respiratory illness severity. SOPI of >1.6 is shown to be indicative of severe respiratory pathology leading to CPAP failure. 6
Underutilization of CPAP support in the initial phase of the disease is a well-established fact. A study from our unit showed 88 out of 100 neonates transported to the hospital lacked monitoring, while only 53% received oxygen. 7 Other studies similarly highlight inadequate stabilization during transport. 8 Neonatal outcomes depend largely on the condition at referral. 9 A 2020 Indian survey cited equipment complexity, cost, and lack of trained staff as key barriers for underutilization of CPAP in neonatal care. 10
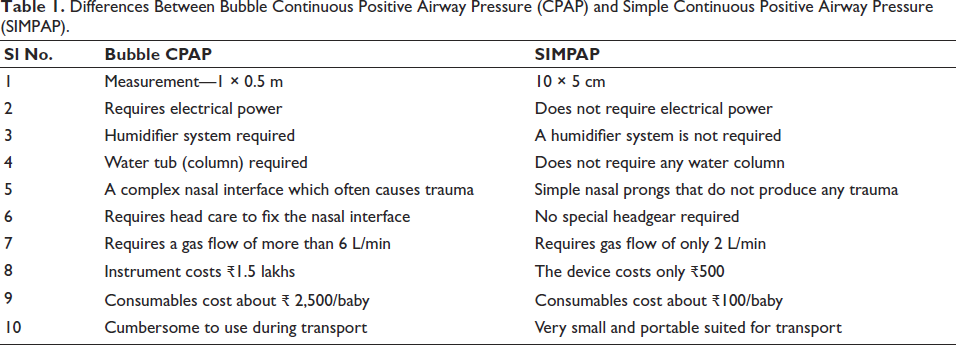
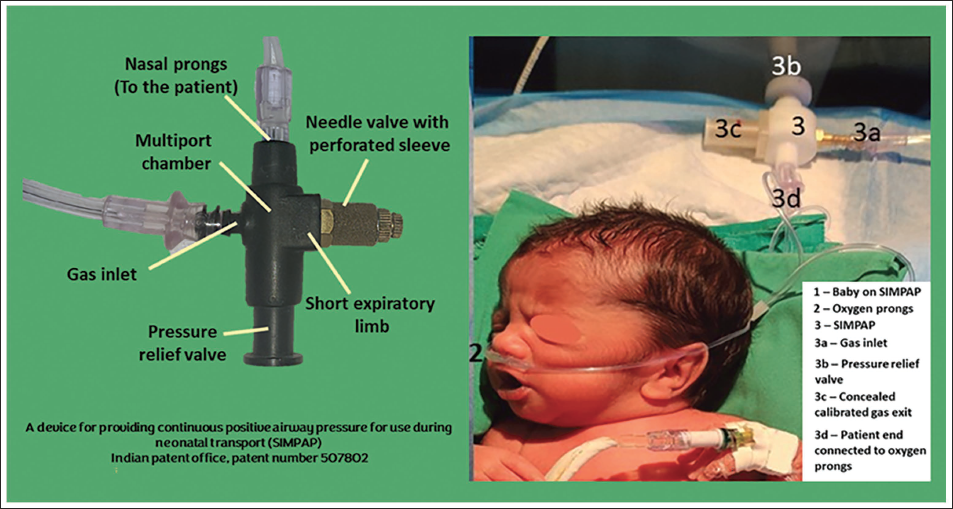
Peripheral centers lack neonatal expertise, necessitating transport to higher centers. Providing CPAP during transport is yet to see the light in many parts of the world. Equipment bulk, need for skilled personnel, and consumable costs hinder early CPAP use. To address these, a novel device, simple continuous positive airway pressure (SIMPAP), was developed by the authors. It delivers CPAP via standard nasal prongs using just 2 L/min gas flow, needing no electricity, humidification, or complex components [Patent no. 201841018247—Indian PTO]. In vitro, it achieved 5-6 cm H2O pressure at the patient end (Figure 1). The differences between traditional bubble CPAP and SIMPAP are listed in Table 1. This study evaluates the in vivo safety and efficacy of SIMPAP versus bubble CPAP.
Differences Between Bubble Continuous Positive Airway Pressure (CPAP) and Simple Continuous Positive Airway Pressure (SIMPAP).
Simple Continuous Positive Airway Pressure (SIMPAP) Device.
Objective
Primary Objective
To compare the change in SOPI from the time of recruitment over 6 h between SIMPAP and bubble CPAP as the initial mode of respiratory support for premature babies.
Secondary Objectives
To compare the change in SOPI between SIMPAP and bubble CPAP as the initial mode of respiratory support for premature babies up to 72 h after initiation of treatment.
To compare the adverse outcomes between SIMPAP and bubble CPAP during the treatment period.
Methodology
Study Design
This was a randomized controlled trial conducted on neonates admitted to the neonatal intensive care unit of a tertiary care hospital. The study was conducted over 6 months.
Inclusion Criteria
Neonates less than 72 h of age and born between 28 and 37 weeks of gestation with respiratory distress (Downes score more than or equal to 3) were included in the study.
Exclusion Criteria
Babies with either of the following were excluded
Congenital diaphragmatic hernia. Severe external congenital anomalies. Cardiac defects. Babies with significant/recurrent apnea needing intubation. Babies with shock, severe hypothermia requiring immediate intubation.
Control
Continuous distending pressure was provided via bubble CPAP (Fisher & Paykel MR850AEU, New Zealand) using a nasal mask. The initial fraction of inspired oxygen (FiO2) was set at 21%, the pressure of 5 cm of H2O, and humidified gas was supplied at 5 L/min. Based on the target saturation, stepwise increments of FiO2 by 5% and CPAP pressures of 1 cm of H2O were done if required.
Intervention
SIMPAP provides a simple, low-cost continuous positive airway pressure of 5-6 cm of water with a gas flow of 2 L/min without the need for humidification of gas. The device consists of a multiport chamber and an exit control valve, which is calibrated to create the required pressure. One of the openings serves as an extremely short expiratory limb that is fitted with a calibrated occlusion. This results in a non-rebreathing system that generates a predetermined pressure against which the baby must exhale. The circuit length is shortened to achieve the required pressure at low gas flow without increasing the resistance of the circuit. A proprietary pressure relief valve has also been installed as a safety measure. 11
Continuous distending pressure was provided via SIMPAP. SIMPAP was initiated at recruitment using snugly fitting nasal prongs attached to the device (Figure 1). Though this device is designed to be suitable for use without humidification, during this study, we have supplied humidified gas as a standard protocol. The initial flow rate was set at 2 L/min and the FiO2 at 21%. Increments in FiO2 by 5% were made to attain the target saturation. The positive end-expiratory pressure (PEEP) was considered to be 5 cm of H2O.
Sample Size
Our pilot study with five cases indicated that the mean difference in SOPI between the two arms was 0.2 with a pooled standard deviation of 0.25. The calculated effect size was 0.8. Considering alpha of 0.05, power of 0.9, and confidence level of 0.95, we needed 27 babies in each arm. We recruited 30 babies in each arm. The sample size was calculated using the online calculator
Randomization and Blinding
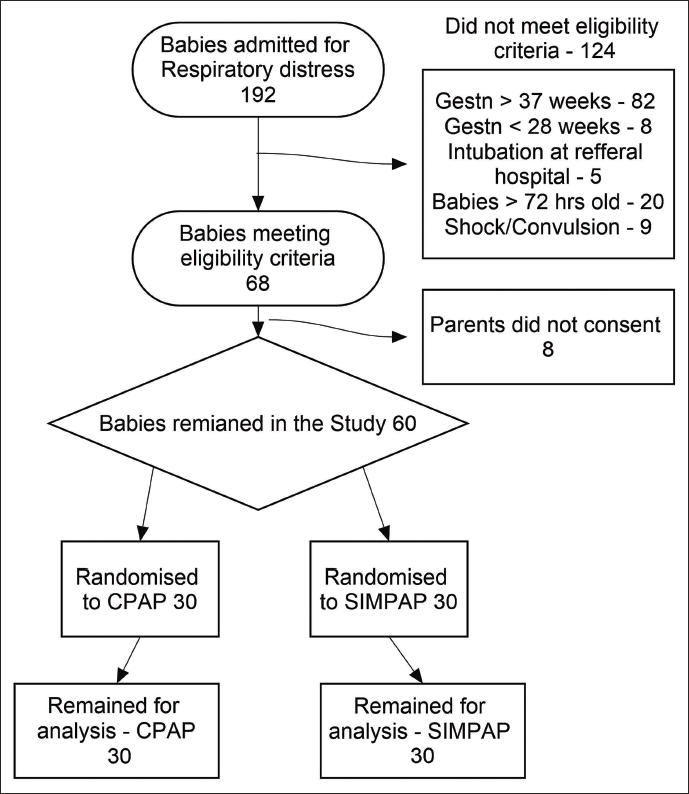
Simple random sampling was adopted for this study. Random numbers were generated in Microsoft Excel. The allocation was concealed in an opaque envelope by one of the authors who was not involved in the clinical assessment of the baby after recruitment and opened by the primary investigator at the time of recruitment (Figure 2). The babies were randomized into two groups, namely SIMPAP (intervention) and CPAP (control), after obtaining informed consent from the parents.
CONSORT Diagram.
Study Measurements
Clinical management was done as per the unit protocol. The SpO2 was monitored with a probe attached to the right upper limb using a multichannel monitor (Philips SureSigns VM4, Philips Medical Systems, China), and SOPI was monitored. A saturation between 90% and 94% was targeted.
Monitoring of CPAP was done by calculating the SOPI. SOPI is a simple, non-invasive, bedside unitless index to monitor the severity of respiratory illness in neonates on CPAP. SOPI was calculated as (PEEP × FiO2)/SpO2. 6 The neonates recruited in the study were followed up for a change in SOPI over 6 h following recruitment. SOPI was estimated every hour for the first 6 h and once in every 6 h till 72 h of age or till the baby got intubated earlier than 72 h. CPAP or SIMPAP failure was diagnosed when SOPI crossed 1.6 and remained so for at least 15 min, thus signaling the need for intubation with surfactant administration.
Carbon dioxide retention was defined as a partial pressure of CO2 (PCO2) of >45 mmHg on arterial blood gas samples. Hemodynamically significant patent ductus arteriosus (HSPDA) was diagnosed when the duct size was >1.5 mm and evidence of flooding of pulmonary circulation was noted as either the left atrium to aortic ratio of >1.6 or the diastolic flow in the left pulmonary artery was >20 cm/s. Probable sepsis was diagnosed when in a clinically suspected sepsis, either the Sepscore was >3 or C-reactive protein (CRP) was >6. 12 Proven sepsis was diagnosed if the blood culture grew any organism. Necrotizing enterocolitis was staged according to Bell’s criteria. 13 The primary endpoint of the study was 6 h from initiation of treatment, and the secondary endpoint was 72 h after initiation of treatment or earlier if intubated.
Ethics
The Institutional Ethics Board approved this study, and informed consent was taken from parents or immediate caregivers. The study was registered under the Clinical Trials Registry of India.
Statistical Analysis
Quantitative variables were summarized. Mean and standard deviation, or median and interquartile range, as per the distribution, were calculated. The primary endpoint was the change in SOPI at 6 h post-treatment; the median SOPI at the study endpoint was compared using the Friedman test. Qualitative data were summarized as proportions, and the relative risk of CPAP failure in both groups was calculated. Means were compared using the Student’s t-test, and the medians were compared when the data were not normally distributed using the Friedman test. Proportions were compared using the chi-square test. Analyse-it for Excel (version 4.3) was used for statistical analysis.
Results
A total of 60 neonates were recruited in this study, among whom 30 were randomized to the SIMPAP group and the remaining 30 to the bubble CPAP group. Both groups were comparable with respect to gestation, birth weight, gender, and initial SOPI. Admission weight and gestational age were normally distributed. Age at recruitment showed a skewed distribution. The difference in gestational age distribution between the groups was not statistically significant (P = 0.87). The baseline characteristics are depicted in Table 2.
Baseline Characteristics.
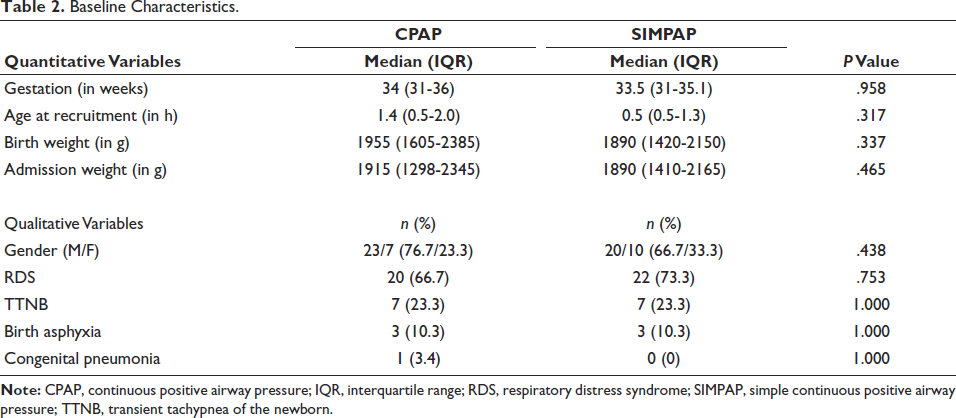
In the CPAP group, the primary indications for respiratory support were RDS in 20 (67%) neonates, congenital pneumonia in 3 (10%), and transient tachypnea of the newborn (TTNB) in 7 (23%). In the SIMPAP group, RDS was noted in 22 (73%) neonates, congenital pneumonia in 1 (3%), and TTNB in 7 (23%). The distribution of diagnoses between the two groups was not statistically significant (P = 0.806).
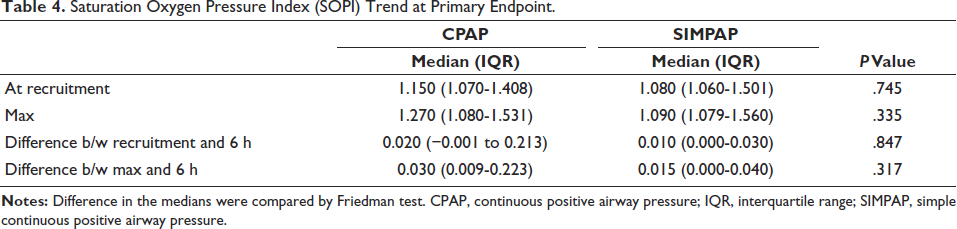
The quantitative outcomes showed a skewed distribution. The median interquartile range (IQR) SOPI in the bubble CPAP group at recruitment was 1.150 (1.070-1.408) and in the SIMPAP group was 1.080 (1.060-1.501). The median (IQR) difference between the SOPI measured at recruitment and 6 h in the CPAP group was 0.020 (−0.001 to 0.213) (Table 3) and in the SIMPAP group was 0.010 (0.000-0.030), P = 0.847 (Figure 3). SOPI at the end of 72 h was 1.07 (1.05-1.07) and 1.05 (1.05) in the control and intervention groups, respectively.
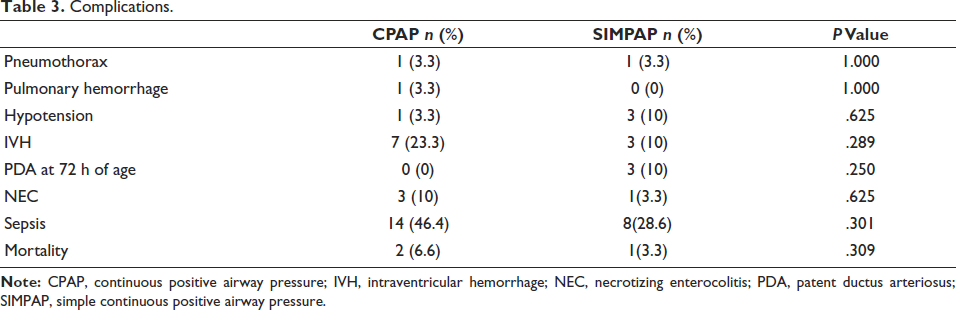
Complications.
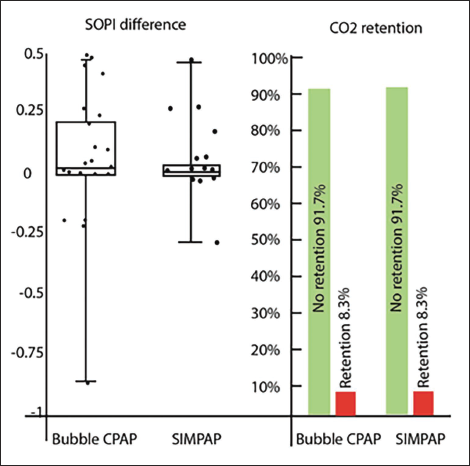
Difference Between Saturation Oxygen Pressure Index (SOPI) at 6 h and CO2 retention in Continuous Positive Airway Pressure (CPAP) and Simple Continuous Positive Airway Pressure (SIMPAP).
Seven neonates (23.3%) in both groups failed the respiratory support they were randomized to, that is, either SIMPAP or bubble CPAP, and required intubation and surfactant administration. The risk ratio (hazard ratio) was 1 (P value = 1.00). The complications like pulmonary hemorrhage, pneumothorax, CO2 retention, and mortality between the two groups were not statistically significant (Table 4). Surfactant was given to 4 (13.3%) babies in the CPAP group and 5 (16.7%) in the SIMPAP group (P value = .968).
Saturation Oxygen Pressure Index (SOPI) Trend at Primary Endpoint.
The user-friendliness of SIMPAP was assessed on the ease of setting up and using, feeding, comfort of the baby while on support, and maintenance of the equipment. Twelve senior nurses participated in the feedback survey and compared the new device, SIMPAP, against their experience of using bubble CPAP. Overall, SIMPAP was considered to be either easy or very easy to use compared to bubble CPAP. A detailed user experience report is provided in Supplementary Material.
Discussion
The main objective of developing SIMPAP was to provide a simple, portable device that does not require electricity or any elaborate setup. The device is designed to work on a low gas flow rate (2 L/min) so that humidification is not needed for short-term use. The patient interface is the regular nasal prongs, which are available commercially. This device does not require any headgear, expensive circuit, or compressor. The device was successfully tested in vitro. 11 The present study is the continuation of the product development cycle, wherein we have studied the device in a clinical environment for safety and efficacy.
The difference in SOPI between recruitment and at the end of 6 h was 0.010 (0.000-0.030) in the SIMPAP group and 0.020 (0.001-0.213) in the CPAP group, which was not statistically significant, suggesting that SIMPAP and bubble CPAP had similar efficacy. The complication rates were comparable. We had initial concerns regarding CO2 retention due to the short expiratory limb. However, at the end of the study, we found there was no CO2 retention in SIMPAP (Figure 3). SIMPAP was similar to bubble CPAP in terms of failure, as the risk ratio (hazard ratio) was 1 (P value = 1.00).
Most of the CPAP devices work on the simple principle of calibrated occlusion of the exit pathway of the gas. 14 However, their build and functioning are complex, making them bulky and sophisticated equipment. They need a constant supply of an air–oxygen mixture at a higher flow rate and a gas humidification system for optimal performance. In addition, the commonly used bubble CPAP needs a water tumbler at the exit end, which has to be kept upright to generate positive pressure in the circuit. The initial high cost of the equipment, expensive consumables, and the need for an uninterrupted power supply preclude the use of CPAP in resource-limited settings. Setting up CPAP for neonates requires highly skilled nursing or respiratory therapy staff who are generally available in dedicated neonatal units only.
There have been a few attempts at building low-cost bubble CPAP by other inventors; however, most of these devices have been tried on lung models and not on real patients. These devices also require high flow rates, which would again need humidification in case used in a clinical setting. Moreover, they appear bulky and cumbersome to use and would probably need a sophisticated interface, unlike the easily available off-the-shelf oxygen prongs that can be used with SIMPAP.15, 16
Limitation
We have done this study based on the results of a small pilot and have not stratified the subjects according to gestational age due to a smaller sample size. A study with a larger sample size, with subjects stratified according to gestational age, is desirable. Another limitation of our study is that SOPI for babies was calculated with a pressure of 5 cm of water, which was the minimum pressure generated in our in vitro studies. However, the pressure delivered could be between 5 and 6 cm of water, which we could not measure.
Conclusion
SIMPAP has similar efficacy as bubble CPAP as primary respiratory support in preterm RDS and other restrictive lung diseases in neonates, in the first 6 h and up to 72 h of initiation of treatment. The complications and failure rate associated with the use of SIMPAP were comparable to those of bubble CPAP.
What is Already Known on this Topic?
CPAP is the primary mode of support for respiratory distress in preterm neonates. Initiating this support at birth and during transport is difficult due to operative complexity. SIMPAP was developed and tested in vitro for providing CPAP support
What this Study Adds?
SIMPAP has similar efficacy as bubble CPAP in a clinical environment
How this Study Might Affect Research, Practice, or Policy?
SIMPAP has the potential to disrupt the way respiratory support is offered to preterm neonates in resource-limited settings.
Footnotes
Authors Contribution
Sushma Krishnegowda, Deepti Thandaveshwar, and Srinivasa Murthy Doreswamy were involved in generating the research question and designing the study. Deepti Thandaveshwar conducted the study. Sushma Krishnegowda did the statistical analysis. Sushma Krishnegowda and Deepti Thandaveshwar prepared the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The Institutional Ethics Board approved this study (JSSMC/IEC/220121/01 NCT/2020-21).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JSS Academy of Higher Education and Research, Mysuru, Karnataka, India (JSSAHER/REG/RES/COV-PRO/351/2020-21 Dated 15.12.2021).
Informed Consent
Written informed consent was taken from the parents of the neonates enrolled in the study.