
Abstract
Purpose
Neonates admitted to the neonatal intensive care unit (NICU) frequently need central line placement, which significantly increases their susceptibility to central line-associated bloodstream infections (CLABSIs). This study aimed to improve adherence to CLABSI care maintenance bundles in our NICU with the aim of reducing infection rates.
Methods
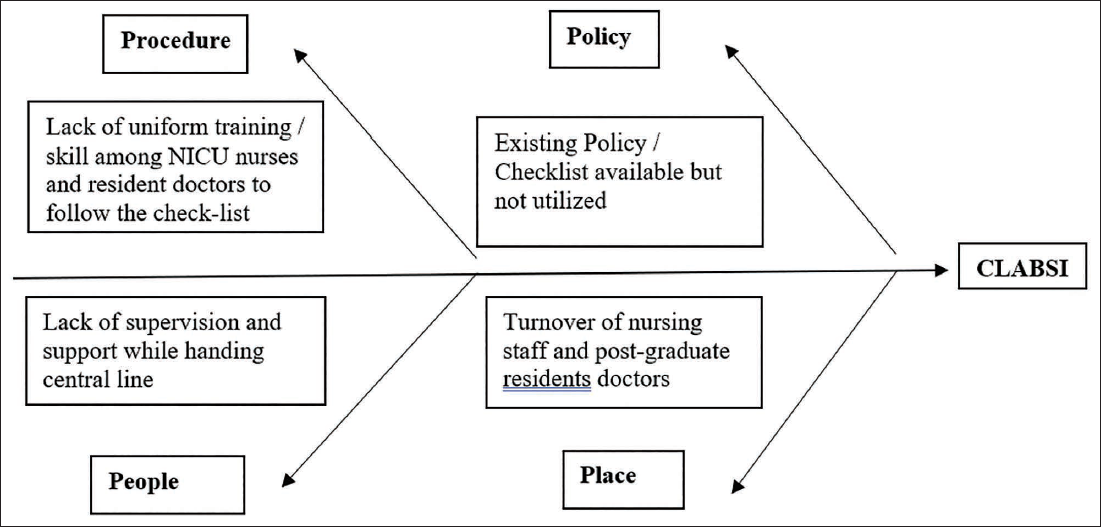
This quality improvement (QI) study was conducted in a tertiary-care NICU. The QI team included a consultant neonatologist, a senior resident, and three experienced staff nurses. A fishbone analysis showed potential barriers, leading to the development of two interventions: training on CLABSI maintenance care bundles, and the decision by doctors in morning rounds about changing the dressing of the central catheter. These interventions were evaluated using two plan-do-study-act (PDSA) cycles.
Results
Initial adherence to CLABSI maintenance care bundles was 65%, with a high CLABSI rate of 13.25 cases per 1,000 central line days in the baseline phase (June-October 2023). After the implementation of the first PDSA cycle (November 2023-January 2024), adherence surged to 97.4%, and CLABSI was reduced to 5.95 cases per 1,000 central line days. At the end of the second PDSA cycle, the CLABSI rate reached 0 per 1,000 central line days with 100% adherence. During the sustenance phase (April-June 2024), adherence was 99.4%, and the CLABSI rate was 4.85 per 1,000 central line days.
Conclusion
Using QI principles, compliance with CLABSI maintenance care bundles improved, and the CLABSI rate per 1,000 central line days was reduced to below five.
Introduction
Central line-associated bloodstream infection (CLABSI) is defined as a laboratory-confirmed bloodstream infection that is not related to an infection from another site, which develops 48 h after the placement of a central line or within 24 h of its removal. 1
Central line catheters are crucial in managing neonates, providing vital venous access that reduces the need for repeated painful peripheral intravenous needle pricks in critically ill newborns. However, their use increases the risk of sepsis among these infants. 2 Neonatal sepsis, especially in preterm and very low birth weight (VLBW) infants, is associated with heightened risks of severe motor impairments and neurodevelopmental delays.3, 4 It also leads to prolonged hospitalization, escalated healthcare costs, and remains a major cause of mortality in this vulnerable population.5, 6 Healthcare professionals have continuously sought effective strategies to reduce the incidence and serious complications of neonatal sepsis to improve outcomes for newborns. 7
The burden of CLABSI can be reduced through evidence-based interventions like hand hygiene, chlorhexidine skin antisepsis, disinfection of catheter hubs, full-barrier precautions during catheter insertion, removal of catheters that are no longer necessary, and careful selection of catheter insertion sites.8–13
It would be best to have no infections. However, it may not be possible to prevent all bloodstream infections in newborns with central lines, and as per the Canadian Nosocomial Infection Surveillance Program, the benchmark for CLABSI in neonatal intensive care units (NICUs) is 1.9 per 1,000 central line days. 14 Retrospective analyses of data from our institute show CLABSI rates between 6 and 14 per 1,000 central line days from 2021 to 2023.
Hospitals have implemented patient safety programs to prevent CLABSI by standardizing central line insertion and maintenance through the use of “care bundles.”15–17 One such program involves establishing a central line team composed of specially trained nurses and physicians who handle all central line insertions, dressing changes, medication administration, and related maintenance following the care bundle protocols. Creating a dedicated line team helps minimize errors and inconsistencies in line care, so that newborns consistently receive the measures to prevent infection. The effectiveness of line teams in reducing CLABSI rates has primarily been assessed concerning the related financial implications.16–19 While this approach proves effective, it may present challenges in implementation within developing countries.
A qualitative process evaluation can help answer key questions and offer important feedback to leaders overseeing the initiative. Central line care bundles, which consist of evidence-based practices aimed at improving patient outcomes by reducing CLABSIs, form the cornerstone of CLABSI prevention.15, 20–22 A recent systematic review and meta-analysis assessing the impact of insertion and maintenance bundles demonstrated a substantial decrease in CLABSI rates across adult, pediatric, and NICU patients. Among 75 NICUs included in the study, the average CLABSI rate dropped by 69%, from 8.4 to 2.6 per 1,000 catheter days. 22 Another systematic review and meta-analysis encompassing 24 studies focused on neonatal intensive care reported a 60% reduction in CLABSI rates following the implementation of care bundles. 15
According to the baseline data collected, adherence to the CLABSI maintenance care bundles and the CLABSI rate in newborns admitted to the NICU at our institute were 65.2% and 13.25 CLABSI per 1,000 central line days, respectively. To reduce the CLABSI rate using a plan-do-study-act (PDSA) cycle, we mainly focused on maintenance bundles. This study was structured into three phases: baseline, PDSA cycles, and sustenance.
Materials and Methods
Definitions
The United States Centers for Disease Control and Prevention (CDC) definition of CLABSIs was utilized in this quality improvement (QI) project. The classification of CLABSIs was performed by the neonatologist in collaboration with the infection control team, following the criteria established by the CDC’s National Healthcare Safety Network (NHSN). 1
Site and Study Design
This QI study was conducted in the NICU of a tertiary-care teaching hospital between June 2023 and June 2024. This study adhered to the Point of Care Quality Improvement (POCQI) learner’s module, and it followed the SQUIRE 2.0 guidelines for reporting.23, 24 The study was approved by the Institutional Ethics Committee, which waived the need for informed consent. The most common isolated organisms are gram-negative, followed by gram-positive organisms. The NICU team and Hospital Infection Control Committee decide on the antibiotic policy based on the culture reports every year.
Unit Capacity and Staffing
The NICU has a total capacity of 20 beds dedicated to intensive care, and additional beds for step-down patients. The unit operates with approximately 80% bed occupancy and a nurse-to-patient ratio of 1:3 for the step-down ward, 1:2 for the NICU, and 1:1 for blood culture-proven sepsis/critical patients. Overall, care was provided by three consultants, nine senior resident doctors, six resident doctors, nursing staff, and housekeeping staff. Based on the need, senior resident doctors inserted the umbilical artery catheter, umbilical venous catheter (UVC), and peripherally inserted central catheter (PICC). Nurses take care of the central catheter and administer drugs and fluids through them. Handwashing adherence of the unit was >95% overall and 100% while handling the central catheter. After handwashing, hands are dried using autoclaved sterile cloth towels. Routinely, after drying the hands, alcohol-based hand rub is used before touching the patient. Resident doctors help in the routine care of newborns by monitoring procedures, attending deliveries, documentation, and so on.
Study Population
This study included critically ill newborns irrespective of gestational age requiring central venous catheter placement, specifically UVCs, umbilical arterial catheters (UACs), and PICCs. The scope of this study was limited to patients admitted to the NICU.
Step 1: Problem Identification, Team Formation, and Writing an Aim Statement (August 2023)
We identified a high CLABSI rate, recorded at 13.25 per 1,000 central line days, as a problem. A team was formed to address this issue. The consultant neonatologist was the leader to direct the meetings and activities. A senior resident doctor doing his Doctorate of Medicine in neonatology was responsible for observing, training, and recording. Three nurses (the nurse in charge, another senior nurse, and an infection control nurse) were involved in communication, real-time documentation of compliance with the checklist, and supervision. The team aimed to decrease the CLABSI rate in the NICU from approximately 13.25 cases per 1,000 central line days to below five over a 9-month period.
Step 2: Analyze the Problem and Measure the Quality of Care (June-October 2023)
The team members identified that the central line insertion care bundle was adhered to properly, but some of the components of the maintenance care bundles of CLABSI (called shortly as the checklist) were not adhered to. To identify causes of non-compliance, 30 observations were conducted during this period for 30 patients. Observations were made in such a way that all nurses taking care of the central line were included. Nurses were unaware that they were observed during this period, without affecting their morals. No interventions were performed during this phase. Observations focused on compliance with CLABSI care bundles and were recorded in real-time by a designated team member. Using fishbone analysis (Figure 1), the team identified some barriers to compliance with the CLABSI care bundle checklist. The indicators identified were adherence to each of the nine components of the checklist, and the outcome was overall adherence to all components of the checklist. To reach the aim, it was decided to achieve an overall adherence of above 95% from the baseline of 65.2%.
Fishbone Diagram.
Step 3: Developing and Testing Changes (Last Week of October 2023)
The key change ideas identified for implementation were training to improve their knowledge and skills. Other consultant neonatologists, resident doctors, and senior residents were also included for training during the PDSA cycles. Thus, everyone remains in the same boat. Weekly assessments and discussions were made during joint meetings led by the consultant neonatologist and which engaged all stakeholders. These meetings ensured continuous communication regarding progress and provided a platform to discuss further changes in ideas for subsequent PDSA cycles.
PDSA Cycle 1 (November 2023-January 2024)
The first intervention was focused on training all staff nurses and doctors regarding CLABSI using a PowerPoint presentation and a video. The presentation included the definition of CLABSI, risk factors, pathogenesis, complications, reasons, prevention strategies, the current baseline CLABSI rate in the NICU, CLABSI checklist, and factors that were poorly adhered to using baseline data. After the presentation, all stakeholders were shown a video on the maintenance care of the central catheter to prevent CLABSI. Training was given for 1 h/day for 3 days to cover all stakeholders. The real-time monitoring of adherence to the CLABSI maintenance care bundles by the study team was performed for 30 patients.
PDSA Cycle 2 (February-March 2024)
During the observations of the previous PDSA cycle, although the indicators improved, there was scope to improve adherence to the change of dressing of the central catheter. In the meeting, it was found that it was required for the doctor to decide and place an order to change the dressing. The nurses did not change the dressing by themselves because of the potential risk of catheter dislodgement. Doctors, with the help of nurses, changed the dressing. As a result, nurses skipped this component of the maintenance care checklist several times. To overcome this, it was decided to carefully look for this component in the morning rounds of doctors and change the dressing accordingly. The real-time monitoring of adherence to the CLABSI maintenance care bundles by the study team was performed for 30 patients.
Sustenance Phase (April-June 2024)
Data collection continued throughout the sustenance phase to evaluate the long-term sustainability of improvements. Daily data were transcribed into an Excel spreadsheet for detailed analysis. No new interventions were introduced during the sustenance phase. The focus remained on maintaining adherence to the indicators.
Sample Size
Being a QI study, at least 30 samples were considered during each phase.
Statistical Analysis
Demographic characteristics were depicted by n (%), mean (standard deviation (SD)), and median (interquartile range (IQR)). Chi-square and one-way analysis of variance (ANOVA) were used to compare adherence (proportion, mean) across all phases. CLABSI rates were compared across each PDSA cycle and the sustenance phase to assess the effectiveness of the interventions implemented during the study.
Results
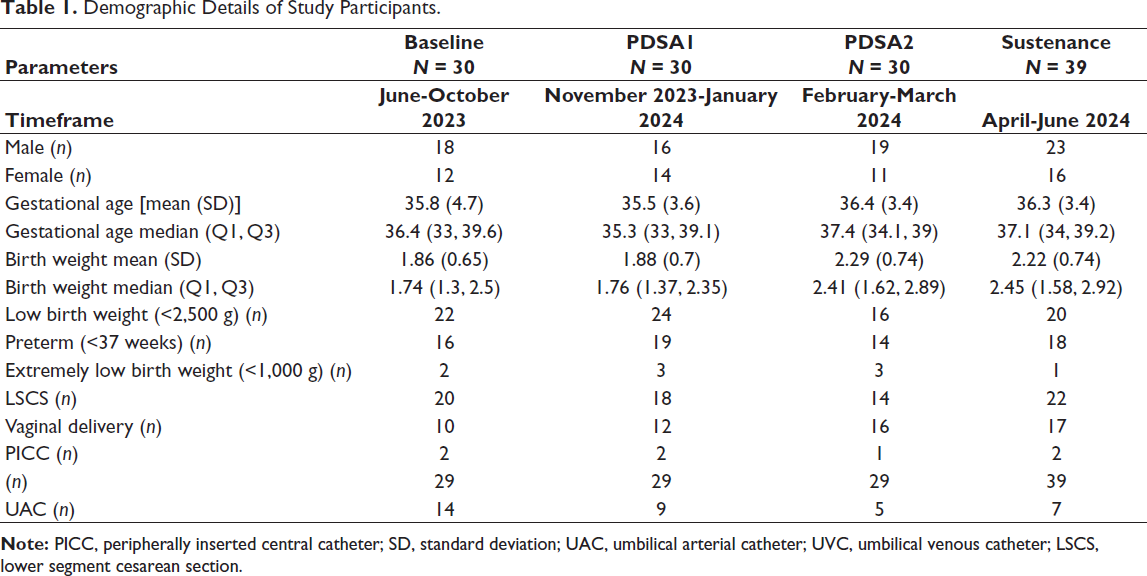
In this QI initiative, a total of 129 neonates were included sequentially over three distinct phases: 30 during the baseline phase, 60 across two PDSA cycles, and 39 during the sustenance phase. The demographic characteristics of these newborns are summarized in Table 1.
Demographic Details of Study Participants.
Baseline Phase (June-October 2023)
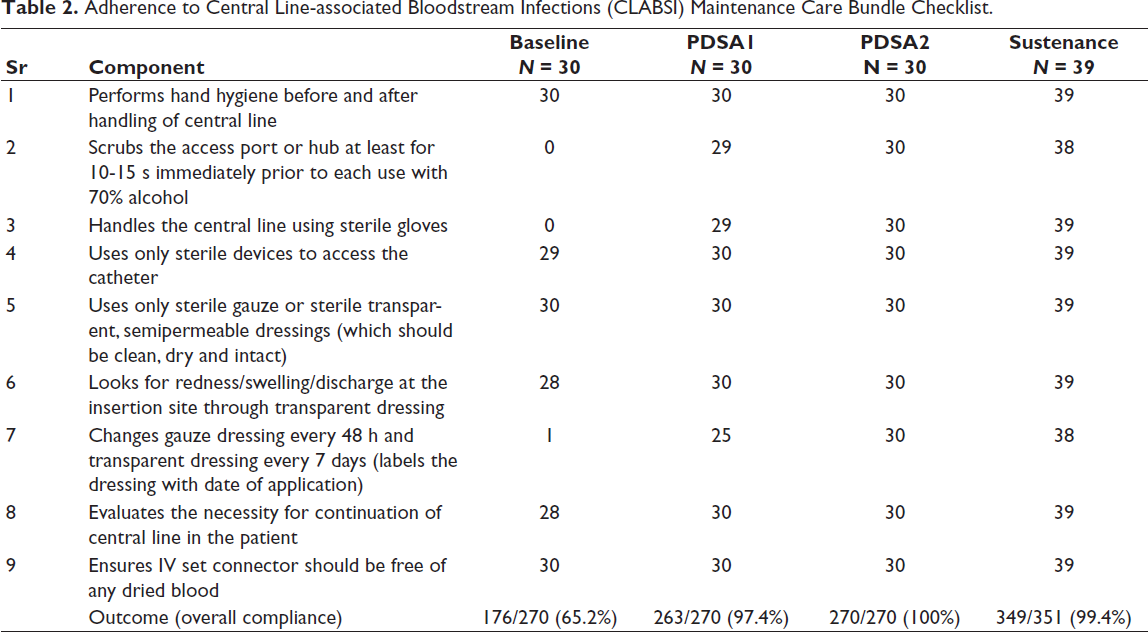
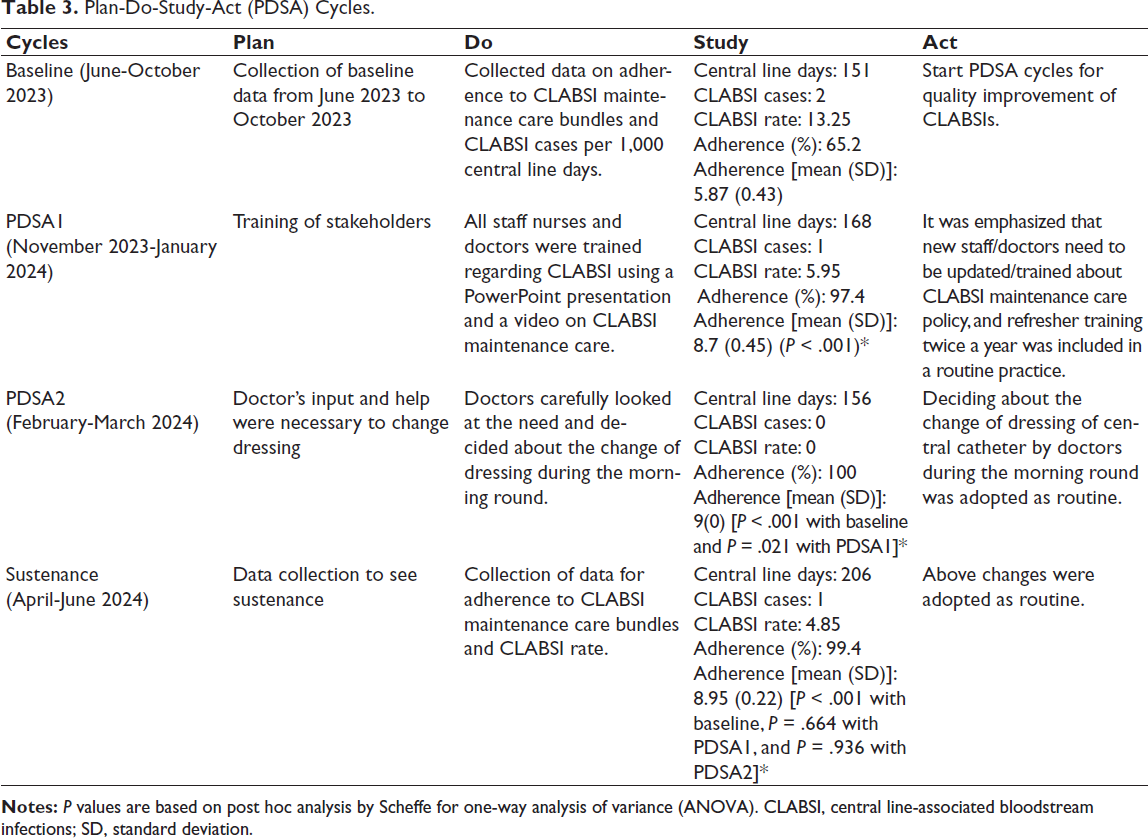
Overall adherence to the CLABSI maintenance care bundle checklist was suboptimal (65.2%). There was almost nil compliance with three components of the checklist: scrubbing the hub, handling the line using sterile gloves, and changing of the dressing (Table 2). As per the Pareto principle, these three components were the major factors responsible for contributing to poor adherence (89 (94.7%) of 94 non-adhered components). This corresponded to a concerningly high CLABSI rate of 13.25 infections per 1,000 central line days, with two infections reported over a total of 151 central line days (Table 3). The mean (SD) value of adherence was 5.87 (0.43) for the total of nine adherence components of the checklist. These findings underscore the urgent need for targeted interventions to enhance compliance with evidence-based maintenance practices.
Adherence to Central Line-associated Bloodstream Infections (CLABSI) Maintenance Care Bundle Checklist.
Plan-Do-Study-Act (PDSA) Cycles.
PDSA Cycle 1 (November 2023-January 2024)
Implementation of training led to dramatic improvements. Adherence to care bundles increased markedly to 97.4%. Correspondingly, the CLABSI rate dropped by more than 50% to 5.95 infections per 1,000 central line days. This reduction was observed over 168 central line days, with only one CLABSI infection reported during this period (Table 3).
PDSA Cycle 2 (February-March 2024)
Building on the successes of the first cycle, intensified efforts of deciding about changing the dressing of the central catheter in the morning round of doctors in the second PDSA cycle led to improvements. Adherence to maintenance care bundles reached 100%, and no case of CLABSI was observed over 156 central line days. Thus, the CLABSI rate reached 0 infections per 1,000 central line days (Table 3).
Sustenance Phase (April-June 2024)
During the sustenance phase, adherence to maintenance care bundles was 99.4%. The CLABSI rate was 4.85 infections per 1,000 central line days, with one infection reported over 206 central line days. Thus, we could sustain the CLABSI rate to achieve the aim of keeping it below five.
One-way ANOVA of the mean adherence as a dependent variable compared with all the phases was significant with the F-value of 670.55, and a corresponding P value was less than .001. The results of post hoc comparisons by Scheffe showed a significant improvement in mean adherence at all PDSA cycles and the sustenance phase as compared to the baseline. Mean adherence at the sustenance phase was comparable with PDSA1 and PDSA2, which helped to reach the aim of CLABSI rate below five (Table 3).
Discussion
This QI study highlights the critical importance of adherence to maintenance care bundle protocols in reducing CLABSI rates among neonates. The implementation of PDSA cycles proved effective in achieving rapid improvements in CLABSI rates, and high adherence to the CLABSI maintenance care bundle could ensure the sustainability of these improvements.
CLABSIs in the NICU can be significantly reduced through the implementation of central line insertion and maintenance bundles. 25 These bundles include essential aseptic techniques, daily assessments of catheter necessity, changes of dressing, and the early discontinuation of central lines when appropriate. Our study observed a remarkable increase in adherence from 65% to nearly 100% during the PDSA cycles, demonstrating the effectiveness of the training of nurses and doctors and the deciding about the need for change in dressing by the doctors in the morning round. The concurrent reduction in CLABSI rates from 13.25 cases per 1,000 central line days to below 5/1,000 central line days proves the transformative impact of adherence to standardized care protocols on patient safety outcomes.
Our findings align with those of other studies conducted in both high-income and low- and middle-income countries (LMICs). For instance, a QI project at the American University of Beirut Medical Center’s NICU reported a 76% reduction in CLABSI rates, from 4.82 to 1.09 per 1,000 central line days, after implementing comprehensive interventions. 26 Similarly, a multi-country study by Rosenthal et al. in El Salvador, Mexico, the Philippines, and Tunisia achieved a 55% reduction in CLABSI rates, from 21.4 to 9.7 per 1,000 central line days, emphasizing the global applicability of such strategies. 27
Notably, Ting et al. highlighted the importance of a structured, multi-step regimen for reducing CLABSIs, with hand hygiene playing a pivotal role in infection control. 28 Barbosa et al. further demonstrated that poor compliance with hand hygiene in NICUs contributes to nosocomial infections, which can be significantly mitigated by alcohol-based hand rubs. In their study, the infection rate declined from 21.5 to 3.2 per 1,000 central line days after intervention, underscoring the critical role of hand hygiene. 29 Similarly, Bowen et al. showed that implementing potentially better practices and raising awareness among NICU staff resulted in over a 50% reduction in infections in premature infants. 20
These practices not only improve patient outcomes but also reduce unnecessary antibiotic use in NICUs, which is a crucial factor in combating antimicrobial resistance. 30
There is further scope for improvement in the CLABSI rate. Many reported and published QI studies in a systematic review and meta-analyses by Payne et al. have shown the sustenance of CLABSI rates below five, and some also achieving near zero, though it was unanswered which care bundle components are effective in different settings. 15
Limitations
The study does not report adjustments for potential confounding variables, such as changes in patient case mix (e.g., gestational age, birth weight), the severity of illness, or concurrent antibiotic stewardship initiatives, which could influence infection rates independently of the care bundle adherence. Despite the promising results, being a single-center study, its interventions need to be tested in multiple settings across regions to strengthen the evidence base.
Conclusion
Use of the CLABSI maintenance care bundle checklist showed a significant reduction in CLABSI rates using a QI approach. Training of stakeholders was one of the key components to achieve the goal, in addition to deciding about the change in dressing during the morning round of doctors. Future studies are called for to reach a nearly zero CLABSI rate.
Clinical Trial Registration
Not applicable as this is a quality improvement study.
Footnotes
Data Availability Statement
Deidentified individual participant data (including data dictionaries) will be made available, in addition to study protocols, the statistical analysis plan, and the informed consent form. The data will be made available upon publication to researchers who provide a methodologically sound proposal for achieving the goals of the approved proposal. The proposals should be submitted to
Declaration of Conflicting Interests
The authors declared no conflict of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
This study was approved by the Institutional Ethics Committee (IEC/BU/147/Faculty/13/297/2023). Informed consent was not required as it was a quality improvement study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.