
Abstract
Background
Neonates, particularly those born preterm, undergo multiple painful procedures in neonatal intensive care units (NICUs). Evidence shows that such exposures are not transient but induce long-lasting neuroimmune and epigenetic changes, creating a phenomenon termed “pain memory,” with effects on brain development and behavior.
Methods
This scoping review was conducted using a PICOT framework. Population: neonates (preterm and term); Intervention: procedural or surgical pain and its management (pharmacological and non-pharmacological); Comparator: infants with lower/no pain exposure or alternative management; Outcomes: (a) biological mechanisms, (b) neurodevelopmental and behavioral sequelae such as anxiety and dysregulation, (c) demographic/sex-specific differences, (d) clinical management strategies; Timeframe: immediate to long-term follow-up. Searches of PubMed, Embase, Web of Science, Scopus, and Cochrane (1990-May 2025) identified 342 records. Following duplicate removal, 270 abstracts were screened, 90 full texts were reviewed, and 30 studies were included. Screening was performed independently by two reviewers, with conflicts resolved by a third adjudicator. Data were charted for design, demographics, interventions, outcomes, and limitations.
Results
Studies have revealed that early nociceptive injury primes microglia and reprograms macrophages through epigenetic pathways. Clinical cohorts showed cumulative pain exposure associated with altered thalamic/cortical development, reduced white-matter integrity, lower cognitive scores, and higher risks of anxiety and behavioral dysregulation. Females exhibited stronger immune-mediated programming, while extremely preterm infants were most vulnerable. Non-pharmacological strategies (skin-to-skin, breastfeeding, sucrose), alongside judicious pharmacological use, reduced acute pain and may influence long-term outcomes.
Conclusions
Neonatal pain memory represents durable biological and behavioral alterations. Multimodal, family-centered approaches should be standard, while future trials must clarify whether early interventions reduce later neurodevelopmental risks and how sex-specific mechanisms can inform personalized care.
Introduction
Neonatal intensive care involves numerous painful procedures, including heel lances, intubation, venipuncture, and chest tube insertion.1, 2 Earlier assumptions that neonates experienced diminished pain responses have been overturned since the 1980s, with studies confirming robust nociceptive activity and adverse stress effects.3, 4 Extremely preterm infants (<32 weeks) may experience hundreds of procedures, often undertreated.2, 5
Evidence now indicates that neonatal pain can imprint on the neural and immune systems, creating “pain memory.” 6 Experimental models show that neonatal surgical injury primes spinal microglia, leading to exaggerated hyperalgesia in adulthood.7, 8 Immune activation produces macrophage epigenetic reprogramming, with more substantial long-term effects in females.9, 10 Human studies parallel these findings, showing that higher procedural pain is associated with altered brain connectivity, reduced thalamic volume, and poorer neurocognitive scores.15–18 Behavioral sequelae include anxiety, attentional deficits, and affective dysregulation. 19
Given these consequences, rigorous neonatal pain management is ethically and clinically imperative. Multimodal approaches integrating pharmacological measures (for major procedures) and non-pharmacological interventions, such as skin-to-skin care, breastfeeding, and sucrose, have strong evidence of efficacy.10, 13, 14 Yet gaps persist regarding their long-term influence on neurodevelopmental outcomes.
This review synthesizes current evidence across four domains: (a) biological mechanisms, (b) neurodevelopmental and behavioral outcomes, (c) demographic/sex differences, and (d) clinical management strategies.
Methods
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) reporting framework to ensure methodological transparency and reproducibility. The research question was defined a priori using the PICOT structure. Population: neonates (both preterm and term). Intervention/exposure: exposure to procedural or surgical pain and the administration of pain management strategies (both pharmacological and non-pharmacological). Comparator: infants with no, minimal, or different pain exposure/management. Outcomes: (a) biological mechanisms underlying pain memory, including neuroimmune and epigenetic processes, (b) neurodevelopmental and behavioral outcomes such as anxiety and dysregulation, (c) demographic and sex-specific differences, and (d) clinical management strategies with attention to long-term effects. Timeframe: outcomes from the immediate postnatal period extending into childhood and adolescence.
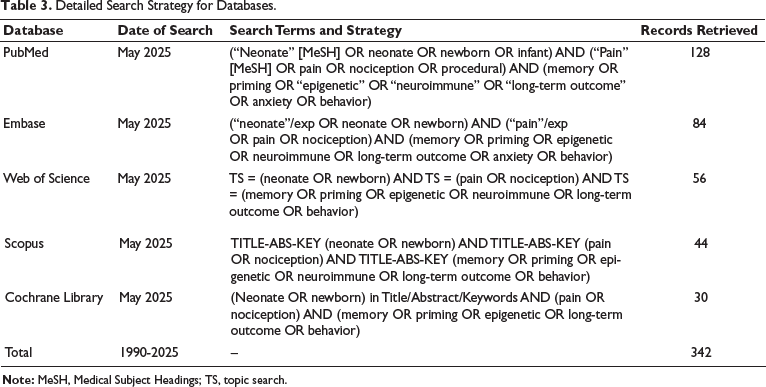
Search strategy: A comprehensive electronic search was performed across PubMed, Embase, Web of Science, Scopus, and the Cochrane Library for the period from 1990 to May 2025. Detailed strategies for each database employed Medical Subject Headings (MeSH) and Emtree terms, synonyms, truncations, and Boolean operators. Search strings were adapted for each database to maximize retrieval (complete search strategy provided in Supplementary Table 2). Reference lists of key reviews and eligible studies were also hand-searched to identify additional records.
Population (P): Neonates, including preterm and term infants, are exposed to procedural or surgical pain. Intervention (I): Exposure to painful procedures and/or pain management strategies (pharmacological and non-pharmacological). Comparator (C): Infants with lower/no pain exposure or different pain management approaches. Outcome (O): Biological mechanisms (neuroimmune, epigenetic), neurodevelopmental/behavioral outcomes (including anxiety and dysregulation), demographic/sex differences, and effectiveness of clinical management strategies. Timeframe (T): Immediate and long-term outcomes assessed during infancy, childhood, and beyond.
Screening and Study Selection
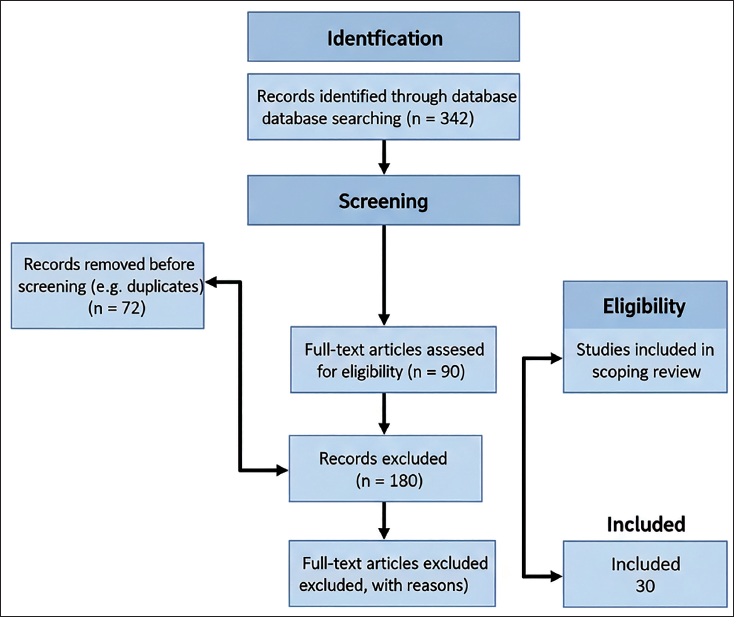
All retrieved records (n = 342) were exported to SciSpace software. After the removal of 72 duplicates, 270 records remained. Titles and abstracts were screened independently by two reviewers. Ninety articles underwent a full-text review. Discrepancies at any stage were resolved through discussion and, when necessary, adjudication by a third reviewer. Reasons for exclusion were documented, and the overall process is depicted in a flow diagram (Figure 1).
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) Flowchart.
Eligibility Criteria
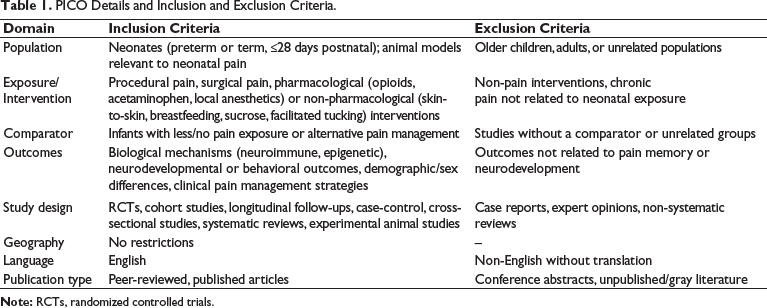
Inclusion and exclusion parameters were defined a priori and summarized in Table 1. Eligible studies included clinical human studies of neonates or infants that assessed procedural pain and outcomes, as well as relevant experimental animal studies investigating the mechanisms of pain memory. Accepted study designs included randomized controlled trials, prospective or retrospective cohorts, longitudinal follow-ups, and mechanistic laboratory studies. No restrictions were applied to geography. Only English-language peer-reviewed articles were included; unpublished data and conference abstracts were excluded. Given the scoping nature, outcomes were mapped rather than pooled, with careful attention to construct validity across mechanistic, imaging, and behavioral domains. Biological mechanisms were operationalized as changes in neuroimmune activity (e.g., microglial priming, macrophage reprogramming, inflammatory mediators), neuronal circuitry or nociceptive processing, and epigenetic modifications linked to stress and pain pathways. Neurodevelopmental outcomes included standardized cognitive and motor assessments at infant and childhood follow-up; behavioral outcomes encompassed internalizing symptoms, attention, affect regulation, and pain sensitivity metrics, including thresholds and cortical responses to stimuli. For management strategies, both immediate analgesic efficacy (pain scores, physiological markers) and any reported long-term outcomes were captured, as well as implementation parameters such as parental involvement and neonatal intensive care unit (NICU) workflow integration.
PICO Details and Inclusion and Exclusion Criteria.
Data Extraction and Charting
Two reviewers independently extracted data using a piloted charting form. Extracted fields included study identification, country/region, year, study design, population characteristics (gestational age, sample size, sex distribution), intervention/exposure details, comparator, outcome domains, significant findings, reported limitations, and authors’ suggested future directions. Disagreements were resolved by consensus.
Risk of Bias and Quality Considerations
Formal risk-of-bias appraisal was not mandated by the PRISMA-ScR framework; however, study-level limitations and potential confounding were abstracted to contextualize findings, particularly regarding illness severity, concurrent sedative/analgesic exposure, and practice variability across NICUs that might influence associations between pain exposure and outcomes. For mechanistic animal studies, considerations include model validity, developmental timing of injury, and translational relevance to human neonatal physiology.
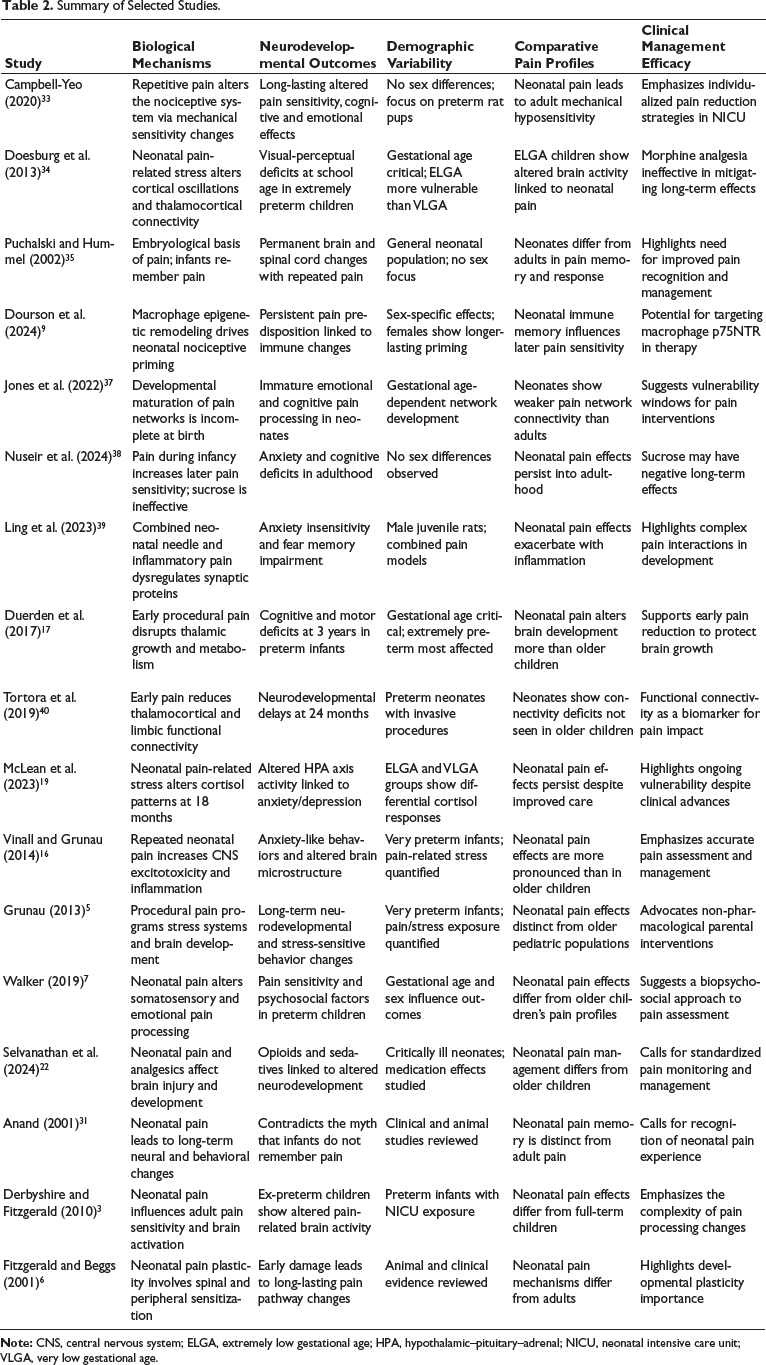
This collaborative team structure ensured rigor, transparency, and minimization of bias at all stages of the review process. No major deviations from the prespecified scope were made; minor refinements included iterative optimization of data-charting fields after pilot extraction to capture sex-stratified results and mechanistic biomarkers more granularly where reported. Anticipated constraints included heterogeneity limiting quantitative synthesis, potential language bias from English-only inclusion, and incomplete adjustment for confounding in observational cohorts—factors that were addressed by structured narrative synthesis and explicit reporting of study limitations in the evidence maps. Table 2 provides summary of studies published on the topic. Table 3 provides the search strategies.
Summary of Selected Studies.
Detailed Search Strategy for Databases.
Results
The search identified 342 records; after removing 72 duplicates, 270 abstracts were screened, 90 full texts were reviewed, and 30 studies met the inclusion criteria for charting and synthesis. Mechanistic studies (predominantly preclinical) consistently demonstrate that early nociceptive injury primes central immune cells—notably microglia—and drives macrophage reprogramming via epigenetic pathways, providing a biologically plausible substrate for durable “pain memory.” Clinical cohorts paralleled these findings: greater cumulative procedural pain exposure in neonates (particularly those born extremely preterm) was associated with region-specific alterations in brain structure and connectivity (including reduced thalamic and cortical volumes and decreased white-matter integrity), lower cognitive scores on follow-up, and increased risks of anxiety and behavioral dysregulation. Sex-specific patterns have emerged, with females showing evidence of stronger immune-mediated programming in several reports. Intervention studies uniformly have showed that non-pharmacological measures (skin-to-skin care, breastfeeding, sucrose, facilitated tucking) and prudent pharmacological strategies reduce acute procedural pain and physiological stress, although direct evidence that these approaches prevent long-term neurodevelopmental sequelae is limited. Overall, the evidence map highlights convergent mechanistic and clinical signals that neonatal pain exposures have persistent biological and behavioral consequences, while also underscoring heterogeneity in study designs, outcomes, and limited long-term interventional data.
Discussion
This scoping review consolidates evidence that neonatal pain is not a fleeting sensory event but is a biologically significant experience with enduring consequences. Convergent findings from animal models and clinical cohorts highlight the existence of “pain memory,” where early nociceptive exposures prime neural and immune systems, imprint epigenetic signatures, and alter behavioral trajectories well into later childhood.6–9, 15–19 Preclinical studies provide strong mechanistic support, showing that neonatal surgical or inflammatory injury activates spinal microglia and primes macrophages, resulting in exaggerated nociceptive responses upon re-exposure in adulthood.7–9 These immune alterations are stabilized by epigenetic reprogramming, including deoxyribonucleic acid (DNA) methylation changes in genes such as SLC6A4 and NR3C1, which are linked to stress dysregulation and anxiety-related behaviors.11, 12 Importantly, sex-specific pathways have been consistently identified: males rely primarily on microglial priming. At the same time, females engage in macrophage-driven and adaptive immune mechanisms, suggesting that interventions may need to be tailored by sex.9, 10, 22
Clinical evidence mirrors these mechanistic insights. Neonates with higher procedural pain exposure show structural brain changes, including reduced thalamic and cortical volumes, disrupted white-matter integrity, and impaired connectivity, which correlates with lower cognitive and motor performance in childhood.15–18 Longitudinal cohorts have link repeated pain exposure with increased risks of anxiety, attentional difficulties, and affective dysregulation. 19 Moreover, altered pain thresholds and heightened cortical responses to innocuous stimuli in ex-preterm children support the persistence of sensitized pain processing beyond infancy.20, 21 Although confounding factors such as illness severity and sedative exposure complicate causal inference, the consistency of evidence across imaging, behavioral, and sensory domains strengthens the case that neonatal pain directly contributes to adverse outcomes.
Demographic factors further shape vulnerability. Extremely preterm infants (<28 weeks) endure the highest procedural burden and exhibit the strongest associations with adverse sequelae.15, 23 Sex differences observed in laboratory studies are reflected clinically, with female preterm infants demonstrating more pronounced disruptions of connectivity after pain exposure. 22 Significantly, environmental influences can mitigate these risks: parental presence and developmental care during hospitalization have been shown to buffer behavioral consequences, underlining the role of family-centered approaches in protecting neurodevelopment. 19
Management strategies are supported by robust evidence for acute pain relief, though their long-term protective effects remain less clear. Non-pharmacological interventions, such as skin-to-skin care, breastfeeding, sucrose administration, facilitated tucking, and parent-led comfort measures, consistently reduce observable pain scores and physiological stress markers.24–28, 33 Pharmacological measures remain essential for invasive procedures; topical local anesthetics and acetaminophen are used for minor and moderate pain, while opioids are reserved for major procedures and postoperative care.29–31 Prolonged opioid exposure, however, has been associated with reduced brain volumes and poorer neurodevelopmental outcomes, mandating cautious use. Novel preclinical evidence suggests that modulation of macrophage p75NTR signaling could prevent nociceptive priming, opening avenues for future immune-targeted therapies. 9
Despite these advances, significant gaps persist. Few interventional studies with long-term follow-up directly evaluate whether improved neonatal pain control reduces later risks of anxiety, dysregulation, or cognitive impairment. Sex-specific mechanisms, although well described in animal models, remain underexplored in clinical cohorts, limiting translation to personalized care. The long-term efficacy of non-pharmacological interventions is inadequately studied, despite their proven short-term benefits. Furthermore, mechanistic biomarkers—such as epigenetic signatures and immune markers—are rarely integrated into longitudinal human research, hindering validation of preclinical findings.
The findings of this review underscore the need for research that moves beyond observational associations and towards targeted interventions with long-term follow-up. Although robust evidence supports the acute efficacy of both pharmacological and non-pharmacological strategies, it remains unclear whether these measures can prevent or attenuate the enduring consequences of neonatal pain memory. Future studies must therefore prioritize prospective, longitudinal interventional trials that evaluate whether standardized multimodal pain management protocols, integrating parent-led non-pharmacological strategies with judicious pharmacological use, translate into measurable improvements in neurocognitive performance, emotional regulation, and behavioral outcomes across childhood. These trials should include structured neuroimaging follow-up, validated behavioral assessments, and integration of biological markers such as DNA methylation and immune profiles, thereby bridging mechanistic insights with clinical outcomes.
Equally critical is the exploration of sex-specific mechanisms in human cohorts. Preclinical data strongly support divergent pathways in males and females, yet most clinical studies do not stratify by sex or are underpowered to detect such differences. Designing trials with prespecified sex-based analyses will be essential for the development of personalized pain management approaches, ensuring that mechanistic discoveries can inform tailored therapeutic strategies.
Non-pharmacological interventions, despite being inexpensive, safe, and highly effective for procedural pain, are inconsistently implemented worldwide. Future implementation research should evaluate barriers to adoption, strategies for training healthcare providers, and the impact of integrating parent-driven measures into standard NICU workflows. Randomized or cluster-randomized implementation trials could establish best practices for ensuring uniform and sustained application of these interventions.
Finally, translational work must extend from preclinical immune and epigenetic discoveries into carefully designed human studies. Emerging evidence suggests that targeting macrophage p75NTR signaling or modulating microglial activity could prevent nociceptive priming. 9 Before clinical translation, however, these approaches require rigorous safety testing, identification of suitable pharmacological agents, and the evaluation of developmental timing to avoid unintended neurodevelopmental effects. Such mechanistic interventions, if proven safe, could represent a paradigm shift from symptomatic pain relief toward preventing the biological embedding of pain memory.
Together, these directions outline a roadmap for advancing neonatal pain research, including rigorous interventional studies, the integration of mechanistic biomarkers, sex-stratified analyses, the systematic implementation of proven strategies, and a careful exploration of novel targeted therapies. Addressing these priorities will allow neonatal care to progress from recognition of pain memory to its prevention, ensuring that vulnerable infants are protected not only from immediate suffering but also from lifelong sequelae.
Limitations
This review has several limitations that warrant acknowledgment. First, although the search strategy was comprehensive and applied across multiple databases with explicit inclusion and exclusion criteria, the synthesis is narrative rather than quantitative due to heterogeneity in study designs, populations, and outcome measures. This precluded meta-analysis and limited the ability to generate pooled effect estimates. Second, many of the human studies included were observational and thus were subject to residual confounding, particularly from illness severity, concurrent treatments, and differences in NICU practices. Third, while animal models offer mechanistic clarity regarding microglial priming, macrophage reprogramming, and epigenetic modifications, their translation to human physiology must be interpreted with caution. Fourth, sex-specific findings are robust in preclinical literature but remain underexplored in clinical cohorts, leading to uncertainty in applying these insights to human care. Finally, although we attempted to capture the most relevant and recent studies, language restrictions to English and exclusion of gray literature may have led to the omission of potentially informative data. These limitations underscore the urgent need for well-designed interventional studies, the integration of mechanistic biomarkers into clinical research, and global collaboration to strengthen the evidence base.
Conclusions
Neonatal pain exposures are not transient experiences but biologically consequential events capable of programming neural, immune, and epigenetic systems. Evidence from animal and clinical studies converges to show that early nociceptive stress leaves lasting imprints on brain development, behavior, and pain sensitivity. Extremely preterm infants and females appear particularly vulnerable, while supportive caregiving can partially mitigate adverse outcomes. Although acute management strategies—especially non-pharmacological interventions and judicious pharmacological use—are effective for procedural pain, their impact on long-term outcomes remains uncertain. Recognition of neonatal pain memory reframes pain management as both an ethical imperative and a determinant of lifelong health. Embedding multimodal, family-centered pain protocols in NICUs is essential. Still, the field must advance further: mechanistic therapies require translation into safe clinical applications, sex-specific strategies must be incorporated into trial design, and longitudinal interventional research is needed to determine whether early mitigation of pain can truly prevent anxiety, behavioral dysregulation, and cognitive impairment in later life. Protecting infants from the imprint of pain memory represents a critical step toward improving neurodevelopmental trajectories and reducing the burden of long-term morbidity.
Footnotes
Authors Contribution
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The authors declared no conflict of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the relevant ethics committee or Institutional Review Board (IRB).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has provided informed consent for the submission of the article to the journal.
Supplementary Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.