
Abstract
Background
Preterm neonates admitted to neonatal intensive care units (NICUs) frequently encounter challenges with breast milk feeding, which compromises their nutrition and immunity. This study aimed to improve colostrum availability for administration from a baseline of 10%-50% among preterm infants using some low-cost, quality improvement (QI) interventions.
Methods
A quasi-experimental pre- and post-test QI study was conducted between June 2023 and May 2024 in a Level III NICU in Northern India. After the initial baseline assessment, interventions including lactation counseling, posters, breast pumps, wrist tags, and tailored educational materials were cyclically implemented in four phases after an initial baseline phase. The study followed four Plan-Do-Study-Act (PDSA) cycles, including a sustenance phase involving a total of 432 participants. Key outcomes were colostrum expression within 6 h and exclusive breastfeeding rates at discharge.
Results
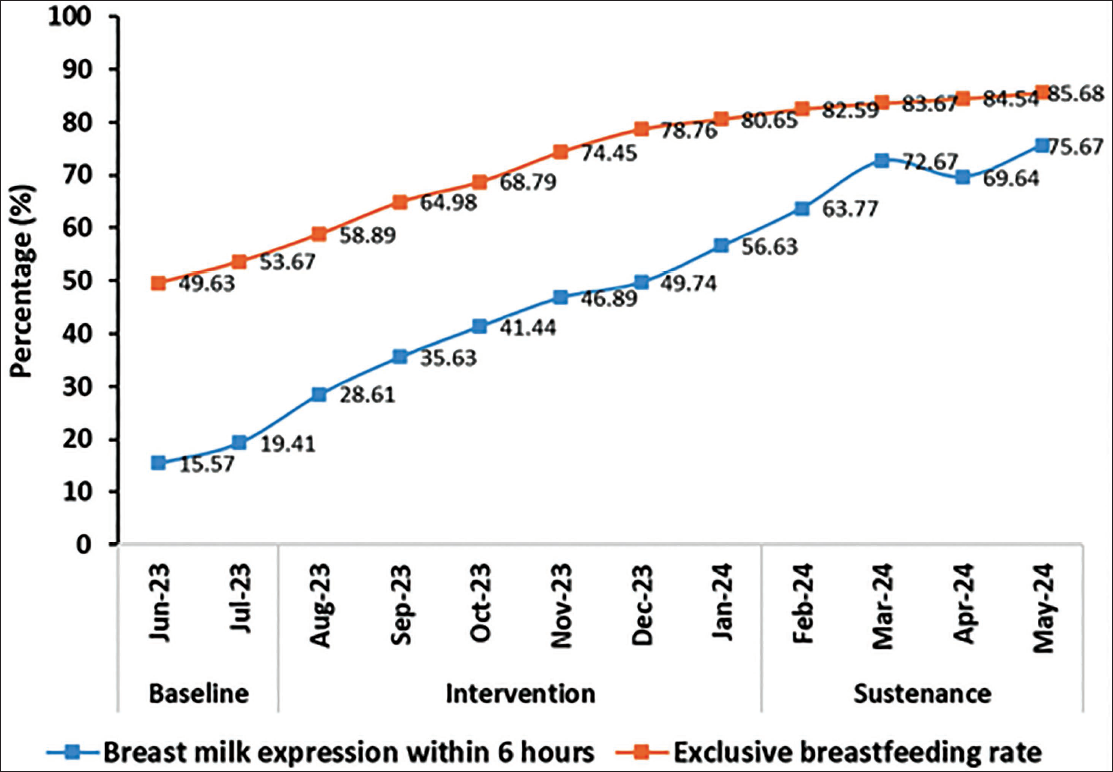
The overall frequency of colostrum expression within the first 6 h increased significantly from 15.57% to 56.63% (P < .001) post-intervention, was further sustained at 75.67% during the sustainability phase, and the exclusive breastfeeding rates at discharge improved from 49.63% to 85.68% (P < .001). Subgroup analyzes further showed the absence of any disparities in outcomes based on either mode of delivery or maternal background, being rural or urban, highlighting the interventions’ adaptability and effectiveness.
Conclusion
Structured, low-cost QI strategies for proper implementation can significantly enhance early colostrum expression and exclusive breastfeeding rates in NICU settings. These findings highlight the need for such cost-effective interventions to improve neonatal outcomes in diverse healthcare setups, thereby providing a practical framework for improving neonatal outcomes in resource-limited environments.
Keywords
Introduction
Colostrum, the first milk produced after delivery, is often described as “liquid gold” because of its rich nutrient and antibody content. It plays a vital role in supporting infant development and immunity, especially in premature infants. 1 Preterm infants, born before 37 weeks of gestation, are susceptible to infections, underdeveloped organs, and various morbidities that put them at higher risk than full-term infants. 2 Colostrum contains concentrated immunoglobulins, growth factors, and bioactive molecules that directly support immune and digestive system development. These components are especially important for meeting the biological needs of preterm infants. 3 However, despite such a vital role, colostrum administration rates in neonatal intensive care units (NICUs) remain low due to various challenges, including delays in maternal milk expression, lack of awareness among caregivers, and structural or logistic barriers within the hospital setting.1, 4
In recent years, there has been a rising focus on using quality improvement (QI) strategies in NICUs to bridge such gaps and promote early colostrum feeding for preterm neonates. 5 QI methodologies, like the Plan-Do-Study-Act (PDSA) cycle, offer structured approaches to identify, address, and overcome barriers to care practices, improving outcomes for both infants and caregivers. These strategies have shown promising results in various healthcare settings, where small, iterative changes yield quantified improvements in clinical practices and patient outcomes.6–8
This study aimed at implementing and assessing a QI initiative to increase the use of colostrum in preterm infants in a NICU setting. At baseline, only 10% of preterm infants received colostrum, and our aim was to increase this percentage to 50% through increasing early colostrum expression (within 6 h) and to ensure greater colostrum receipt by preterm neonates by using a few low-cost targeted interventions that included staff education, maternal support, and workflow adjustments.
We aimed to create a supportive environment for the administration of colostrum by focusing on caregiver education and logistical improvements, which would benefit the susceptible population of preterm infants by providing early immune support and promoting healthier short- and long-term outcomes. 9 These results can be applied as a prototype for other NICUs that intend to implement the systematic change of practice in order to improve the rate of colostrum utilization, thereby ultimately supporting better health outcomes in preterm neonates and paving the way for further research and improvement in neonatal care. This QI study was designed and reported in accordance with the SQUIRE 2.0 (Standards for QI Reporting Excellence) guidelines to ensure methodological transparency and reproducibility.
Material and Methods
Setting and Population
This QI study was conducted in the Level III NICU attached to a tertiary care teaching hospital in Northern India, focusing on preterm infants born before 37 weeks of gestation. The study population included preterm infants eligible to receive colostrum and their mothers who were physically able to express breast milk. Infants with specific medical contraindications to receiving colostrum (e.g., severe congenital malformations, suspected or proven inborn errors of metabolism, or necrotizing enterocolitis (NEC) stages II/III) were excluded.
Study Design
The study adhered to the SQUIRE 2.0 guidelines for the design, implementation, and reporting of QI interventions in healthcare settings. The study followed a QI model using the PDSA cycle framework. This approach allowed for iterative changes and rapid assessment of interventions, enabling the team to adjust strategies as necessary to maximize the effectiveness of colostrum administration in the NICU.
The study was conducted in five phases, with a new group of newborns included in each phase. A total of 432 newborns were included in the study. Phase 1 (June-July 2023)—baseline; Phase 2 (August-September 2023) breastfeeding counseling; Phase 3 (October-November 2023) posters were introduced, along with measures to improve the availability of expressed breast milk to support infant feeding. Phase 4 (December 2023-January 2024) posters and tags, and Phase 5 (February-May 2024) was the sustainability phase.
Baseline Assessment and Identification of Barriers
Baseline data were first collected to understand the present rates of usage of colostrum, reasons for underutilization, and challenges that both mothers and healthcare providers face in the NICU. Some of the commonly reported barriers include a lack of awareness regarding the importance of colostrum, inconsistent support of mothers for expressing milk, and logistical challenges related to collection and administration. During the baseline phase, electric breast pumps were available, but their use remained inconsistent. This was mainly due to limited maternal awareness, inadequate lactation counseling, variable pump availability, and delays in initiating milk expression. No structured pumping protocols or expression support were in place during this phase.
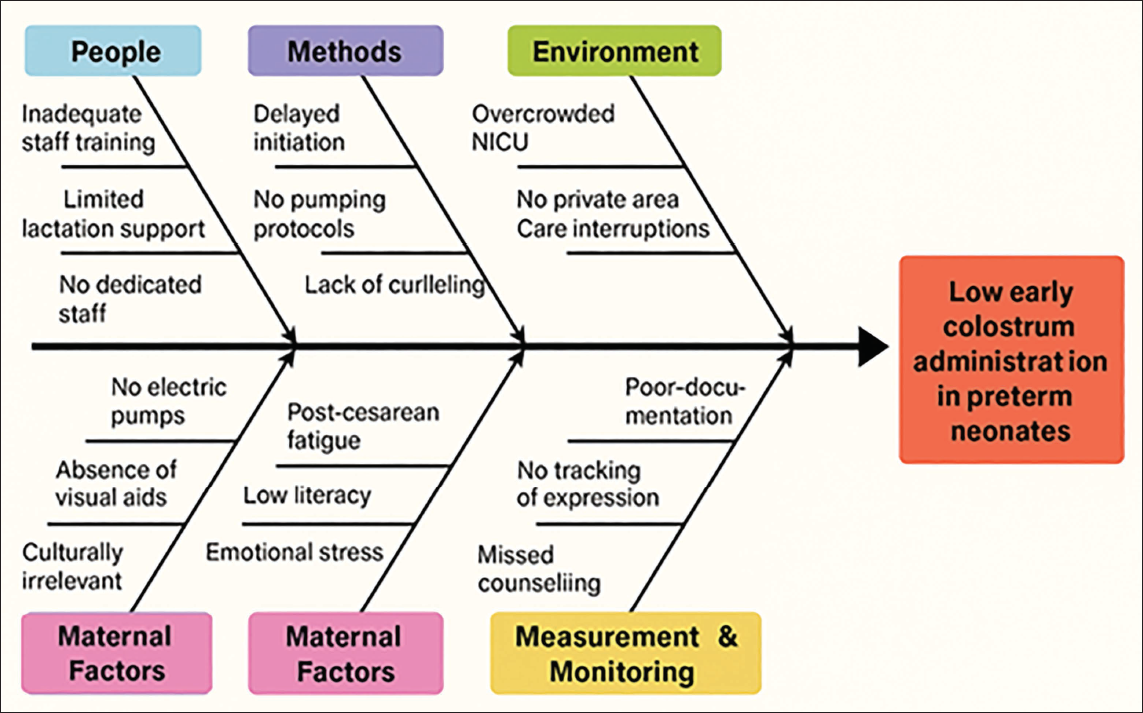
A detailed root cause analysis was conducted using a fishbone (Ishikawa) diagram (Figure 1) to systematically explore the multifactorial reasons for low early colostrum administration in preterm neonates. The causes were categorized under six domains: (a) People—including inadequate staff training, inconsistent maternal support, and lack of designated lactation personnel; (b) Methods—such as delayed initiation of expression, absence of structured pumping protocols, and lack of timely counseling; (c) Environment—including overcrowded NICU layout, lack of private expression areas, and interruptions in care routines; (d) Materials—referring to initial unavailability of electric breast pumps, absence of visual communication tools, and culturally irrelevant education media; (e) Maternal factors—including post-cesarean fatigue, low literacy, emotional stress, and cultural hesitation; and (f) Measurement and monitoring—lack of documentation systems for milk expression frequency, volume, and missed counseling. This analysis provided the foundation for designing the sequential PDSA cycles and tailoring interventions to address each barrier comprehensively.
Intervention Strategies
A set of interventions was designed to address these barriers, focusing on three primary areas: staff education, maternal support, and workflow adjustments. Each intervention was implemented and tested within a PDSA cycle to monitor its effectiveness and make necessary adjustments. For very small volumes of expressed colostrum, oral mucosal swabbing was performed using sterile applicators. This was done 2-3 times daily, depending on colostrum availability and infant readiness for feeds. NICU nurses performed the procedure under aseptic precautions. This method was employed especially for infants not yet ready for enteral feeds. For slightly larger volumes, colostrum was administered via low-volume oral syringes, ensuring minimal wastage and direct absorption. Swabbing was performed by trained NICU nurses under aseptic precautions during routine care hours. It was carried out 2-3 times daily, depending on the availability of colostrum and infant feeding readiness. Swabbing was done gently on the buccal mucosa using sterile applicators, and mothers were encouraged to observe or participate when feasible. No adverse effects or mucosal injuries were noted during the swabbing process, confirming its safety and feasibility in the NICU setting. Not all change ideas initially proposed yielded successful or sustainable outcomes. For instance, in the early phases, we attempted to use peer support models involving previously lactating mothers to motivate current NICU mothers; however, due to low participation and logistic constraints (e.g., timing of visits, privacy concerns), this approach was not feasible and was discontinued. Similarly, initial educational posters in English did not resonate well with all caregivers, prompting redesigns in local languages with pictorial formats. In the breast pump sharing system, initial scheduling conflicts and non-availability during peak hours led to revised timing slots and the addition of manual pumps. These learnings were critical in refining subsequent interventions, reinforcing the iterative nature of PDSA cycles.
While designing the interventions, several maternal factors were considered to ensure feasibility and acceptance. These included mode of delivery (especially post-operative discomfort after C-sections), maternal fatigue, literacy level, language preference, and emotional readiness. Educational materials were translated into local languages with pictorial guides for low-literacy mothers. Flexible counseling times were provided to accommodate maternal recovery, and expression support was intensified for mothers facing post-operative barriers. Psychosocial sensitivity was emphasized throughout, reinforcing a mother-centered approach.
PDSA Cycles
The sequence of the PDSA cycles was determined based on feasibility and the readiness of implementation components. Establishing regular milk expression practices was considered the most immediate and logistically manageable intervention, as it required minimal resources and allowed for early engagement with mothers. Comprehensive educational sessions were planned after basic practices were initiated to maximize receptivity and reinforce behaviors already being adopted. Moreover, educational material development and staff scheduling required preparatory time. This stepwise escalation allowed each intervention to build upon the previous, optimizing cumulative impact and sustainability.
PDSA Cycle 1: Regularization of Milk Expression
The change idea was to express milk by breast pump at regular 3-h intervals from the day of delivery. The research team studied whether this change idea would enable the mothers to establish and sustain a milk supply.
Plan (P1): A structured schedule was provided to mothers, emphasizing the physiological basis of regular pumping for establishing milk supply. Educational videos were shown, and live demonstrations were conducted for enrolled mothers.
Do (D1): A buddy system was implemented whereby a NICU nurse, designated as the “NICU Buddy” and trained in lactation support, provided real-time, hands on assistance to mothers to ensure correct milk expression and pumping techniques.
Study (S1): We monitored compliance through pumping logs and assessed milk volume per session.
Act (A1): Further refinement was to be based on barriers identified, such as timing clashes with medical rounds or fatigue.
As lactation improved, this cycle was accepted.
PDSA Cycle 2: Professional Health Education
The change idea was to initiate professional health education encompassing the key aspects of breastfeeding to mothers of preterm and very low birth weight (VLBW) babies to provide adequate milk.
Plan (P2): The development of a tailored curriculum for mothers, including:
Benefits of colostrum. Proper hand-expression techniques. Use of breast pumps. Skin-to-skin contact’s role in lactation.
Do (D2): We conducted group sessions with role-play and Q&A. Distribution of some take-home materials, like posters, infographics, and wrist tags. Posters highlighting the importance of colostrum and the benefits of early milk expression for both mother and baby were displayed in the waiting areas of antenatal care (ANC) visits, outpatient department (OPD), NICU, and labor operating theater (OT) complex. This was done to raise awareness among mothers and their families and to support them in the process.
Study (S2): Use of pre- and post-session quizzes to assess understanding. The research team studied whether this change idea would enable mothers to improve the technique of expressing milk through manual and breast pumps.
Act (A2): Adaptation of revision sessions to address frequently misunderstood topics.
As lactation improved, this cycle was accepted.
PDSA Cycle 3: Breastfeeding Guidelines
The change idea was to establish breastfeeding guidelines for timely pumping and milk expression, promote skin-to-skin contact, express milk since day 1 of delivery, and improve breast milk storage techniques.
Plan (P3): To create and disseminate user-friendly guidelines in the form of laminated cards or photographs of these cards on their mobile phones. Key addressed areas were:
Timely initiation of pumping. Skin-to-skin contact duration (e.g., 4-8 h per day). Regarding safe storage and handling of expressed breast milk by mothers and healthcare workers.
Do (D3): To train NICU staff to demonstrate these steps during routine care and mothers’ visiting times.
Study (S3): The team studied whether this change idea would enable the mothers to express more milk. We aggregated focus groups with mothers to gather feedback on guideline usability.
Act (A3): We updated guidelines to address practical challenges like milk storage space constraints and transport issues.
As lactation improved, this cycle was accepted.
Cycle 4: Sustainability/Sustenance Phase
During the four-and-a-half months of intervention and the five-and-a-half months of sustenance phases, all strategies that increased rates of exclusive breastfeeding at discharge and early breast milk expression were promoted.
Plan (P4): To incorporate all interventions into routine NICU workflows. Also, to assign specific responsibilities (e.g., lactation counselors for daily rounds).
Do (D4): We developed a digital tracking system (e.g., WhatsApp messages for pumping reminders and milk volume tracking). The milk bank registry was evaluated by the investigator periodically.
Study (S4): We analyzed long-term adherence rates and identified drop-offs by the continuum of contact.
Act (A4): The team integrated thus acquired feedback into hospital policy to ensure sustainability.
In addition, the frequency of the main outcome and adherence to the various QI interventions were continuously assessed.
Standardization of Intervention Tools and Implementation Steps
We standardized tools by developing culturally sensitive educational materials in Hindi. These included visual aids and step-by-step pictorial guides to support mothers with low literacy. Digital and physical diaries were introduced to help track expression frequency. Digital and physical diaries were being created to track milk expression, and user-friendly electric breast pumps were provided by the hospital milk bank on a sharing basis to reduce maternal fatigue and enhance compliance.
Private spaces in the NICU were allocated and earmarked for milk expression, equipped with comfortable seating, breast pumps, and hygiene supplies. Each intervention was pilot-tested on a small cohort to refine our strategies, and feedback was actively sought from mothers, ground force nurses, and NICU residents, with findings documented and shared with all the study investigators.
Data Collection and Monitoring
Throughout the study, data were collected on several key metrics, including the percentage of preterm infants receiving colostrum, time to initial colostrum administration, and feedback from staff and mothers on the intervention processes. This data were analyzed after each PDSA cycle to evaluate the impact of each intervention and to identify areas needing further improvement. Milk expression data were recorded in terms of the frequency of expression sessions per 24-h period, as documented in maternal pumping diaries. Milk volume per session was not uniformly recorded due to practical constraints during routine NICU care and hence was not included in the outcome analysis. To ensure data quality and completeness, data collection was performed by trained NICU nurses and supervised daily by a designated study coordinator. All logs (expression diaries, counseling checklists, and swabbing records) were reviewed weekly by the principal investigator. Data entry was double-checked, and discrepancies were resolved through cross-verification with nursing documentation and patient charts. These steps ensured consistent documentation throughout the study phases. Baseline data were collected by the same QI team members who later implemented the interventions. This ensured consistency in data definitions, accuracy in documentation, and continuity in monitoring. All data collectors were trained prior to initiation and followed standardized data recording formats throughout the study.
Analysis of PDSA Cycles
Four PDSA cycles were completed over the 6 months of the study. Each was built on understanding and learning from information and data acquired in the earlier cycle, driving improvements in the efficacy of interventions for educational materials for mothers, maternal support, and workflow improvements to continuously improve barriers as they surfaced.
Sample Size Calculation
We performed a sample size calculation to ensure 90% power and a 5% alpha error for detecting a 40% hike in colostrum use among preterm infants. Assuming a baseline colostrum administration rate of 10% and an anticipated post-intervention rate of 50%, the effect size was calculated using the formula for comparing two proportions. Using a Z-score of 1.96 for a 5% significance level and 1.28 for 90% power, the required sample size was estimated to be around 224 participants per group and a total of 448 participants. The PDSA approach was facilitated by dividing the total sample size into five phases in sequence, which will distribute the distribution among 80 participants for the baseline and 92 participants each across the remaining four intervention cycles, which are implemented in a synchronized manner to allow phased review and further necessary adjustments to interventions. Although the calculated sample size was 448, due to logistical constraints and exclusions, 432 participants were included in the final analysis.
Statistical Analysis
All analyzes were performed on the study cohort of 432 preterm neonates. Descriptive statistics were used to summarize maternal and neonatal characteristics. Continuous variables such as gestational age, birth weight, and daily frequency of breast milk expression were expressed as mean ± standard deviation (SD), and comparisons across phases were made using one-way analysis of variance (ANOVA) with post hoc testing. Maternal age was reported as median interquartile range (IQR) and compared across groups using the Kruskal–Wallis test. Categorical variables, including mode of delivery, place of residence, comorbidities, and colostrum expression rates, were expressed as numbers and percentages. These were compared using the chi-square test or Fisher’s exact test, as appropriate.
The primary outcome was the proportion of mothers expressing colostrum within 6 h. Secondary outcomes included the mean daily frequency of breast milk expression and exclusive breastfeeding rates at discharge. Comparisons between study phases were performed using one-way ANOVA, as each phase comprised independent participant cohorts, and chi-square tests for categorical outcomes. For subgroup analyzes, stratified comparisons were made for mode of delivery (cesarean vs. vaginal) and maternal background (urban vs. rural). All analyzes were two-tailed, and a P value < .05 was considered statistically significant. Statistical analyzes were performed using Statistical Package for the Social Sciences (SPSS) version 21 (IBM Corp., Armonk, NY, USA).
Ethical Considerations
The study was conducted following ethical standards, with approvals from the hospital’s ethical committee. Participation by mothers was voluntary, with informed consent sought to participate in the educational and support components. Data collected during the study were completely anonymized so as to ensure participant confidentiality.
Results
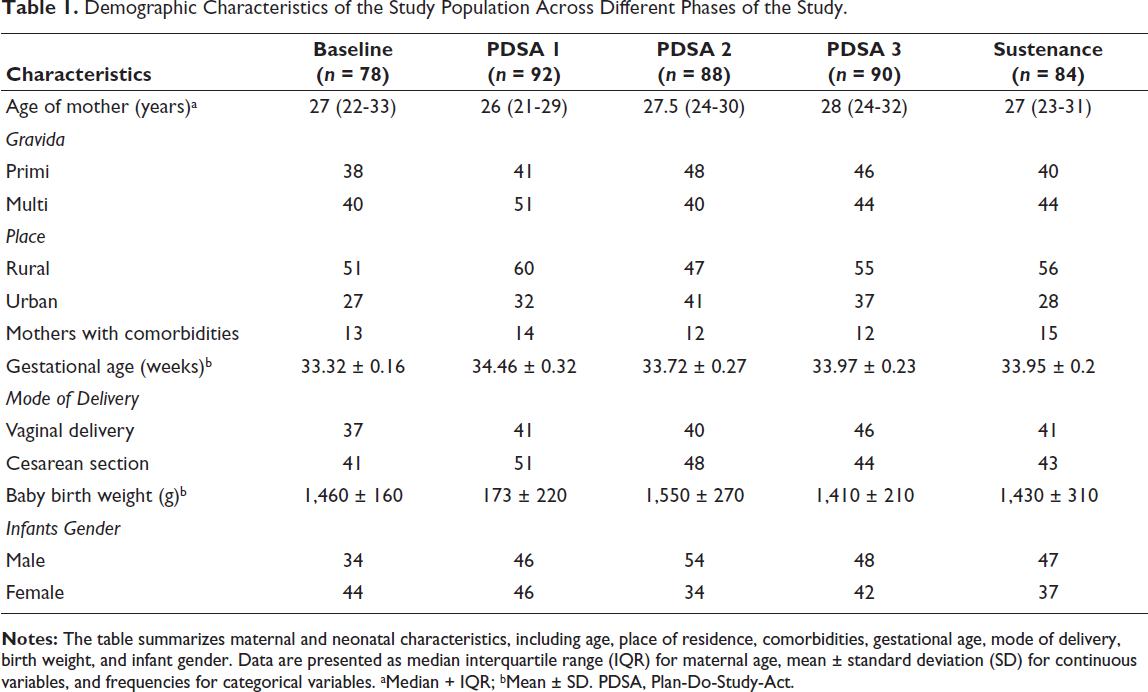
In our study, we included 78 preterm neonates during the baseline phase, with an average gestational age of 33.3 ± 1.6 weeks and a mean birth weight of 1,460 ± 160 g (mean ± SD). By the end of the sustenance phase, 84 neonates got enrolled, with an average gestational age of 33.9 ± 0.5 weeks. The two groups were statistically comparable in birth weight and gestational age (Table 1).
Demographic Characteristics of the Study Population Across Different Phases of the Study.
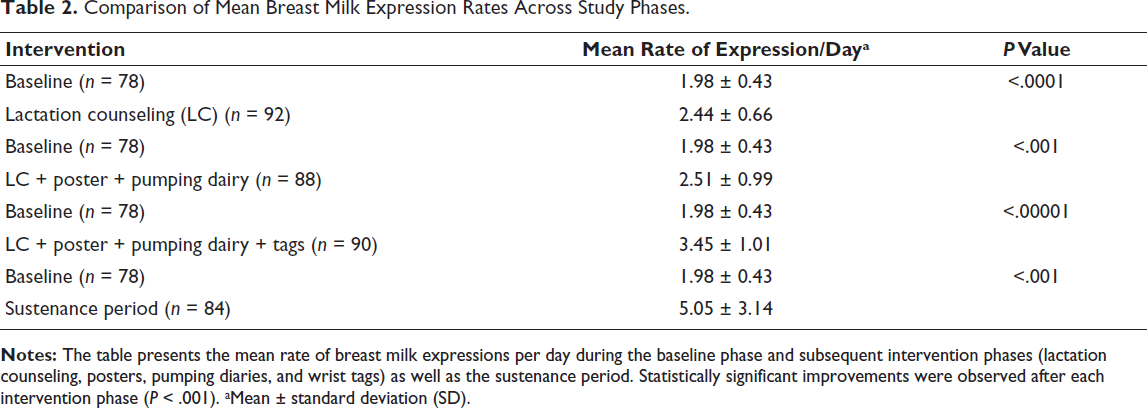
A progressive improvement was observed in the mean daily frequency of breast milk expression, defined as the average number of pumping or breastfeeding sessions per 24-h period as recorded in maternal pumping diaries. This frequency increased significantly from 1.98 ± 0.86 sessions/day at baseline to 5.05 ± 3.29 sessions/day during the sustenance phase (P < .001). Statistically significant gains were observed after each PDSA cycle, highlighting the cumulative impact of lactation counseling, posters, expression diaries, and motivational wrist tags (Table 2; Figure 2). Milk volume per session was not recorded and hence not analyzed. The interventions brought about a remarkable improvement in breast milk expression within the first 6 h, increasing from just 15.57% at baseline to 56.63% by the end of the intervention phase (P < .001) (Table 2). Importantly, during the sustainability phase, the rate was maintained and further improved to 75.67%, demonstrating the durability of the intervention impact. Similarly, exclusive breastfeeding rates at discharge saw a significant rise from 49.63% to 85.68% (P < .001), maintaining consistency during the sustenance phase (Figure 3).
Comparison of Mean Breast Milk Expression Rates Across Study Phases.
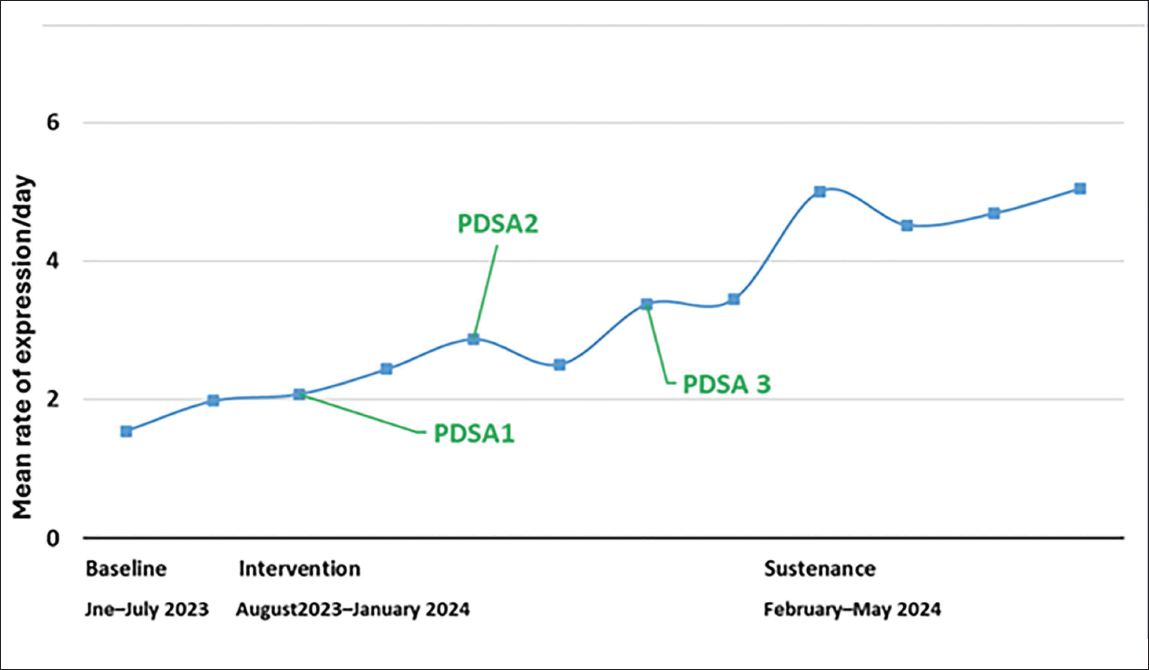
A transient dip in expression frequency was observed immediately after PDSA 2, despite the implementation of posters and pumping diaries. On further analysis, this period coincided with temporary staff reallocation due to a hospital-wide manpower shortage and limited access to expression spaces during NICU infrastructure maintenance work. These operational disruptions were short lived and resolved within 1-2 weeks, after which adherence improved during PDSA 3. This dip highlights the importance of accounting for contextual and logistical factors while interpreting QI run chart trends.
Subgroup analysis was performed to evaluate the adaptability of the interventions with respect to the mode of delivery and sociodemographic background. At baseline, cesarean section mothers faced greater challenges, with only 12% expressing colostrum within 6-12 h, compared to their vaginal delivery counterparts. However, post-intervention, this gap was eventually closed, with cesarean mothers achieving a colostrum expression rate of 54.5%, nearly matching the 58.1% observed in vaginal deliveries (P = .23). Similarly, there were no significant differences in outcomes between mothers from urban and rural backgrounds post-intervention, with both groups achieving similar colostrum expression rates (urban: 56.63%, rural: 56.5%, P = .94).
These results show the effectiveness of our targeted, low-cost interventions in overcoming barriers to colostrum expression and exclusive breastfeeding. The findings showed that our interventions were equally effective and well-received by all mothers, irrespective of their mode of delivery or geographical background, which emphasizes the adaptability of these strategies that we employed.
Discussion
This study showed how low-cost, structured interventions can considerably improve early colostrum expression and rates of exclusive breastfeeding in preterm neonates—a long-standing challenge in NICUs. Parents of ill preterm neonates frequently lacked familiarity with the NICU environment and relied strongly on medical staff for guidance and support at baseline. Such support from peers or health care providers has been shown to be crucial for empowering mothers and improving the babies’ ability to nurse effectively.2, 10, 11
The outcomes of this QI project are a testament to themselves. The proportion of mothers performing expression of colostrum in 6 h significantly increased from 15.57% at baseline to 56.63% at the end of the intervention period, whereas exclusive breastfeeding improved from 49.63% to 85.68%. These results are in line with those of Bagga et al. 2 and Lee et al., 12 who demonstrated that, through structured counseling and focused interventions, there is a marked improvement in the utilization of breast milk. Unlike many QI projects where benefits decline after the intervention stops, our improvements were sustained. Colostrum expression continued to rise during the sustainability phase, indicating strong retention of behavior change. Equally important, this study found that the intervention resulted in equitable outcomes across the sociodemographic groups, as there were no significant differences in the rates of colostrum expression between urban and rural mothers or between cesarean section and vaginal delivery mothers.
Our individualized approaches addressed specific breastfeeding barriers, such as post-operative pain, unawareness, and logistics. For example, the application of wrist tags, posters, and pumping diaries ensured the mother’s consistent milk expression and motivated them to conquer those barriers. Along with this, individualized lactation counseling led to maternal confidence and adherence to the breastfeeding practice. The results agreed with those reported by Rosen-Carole et al., 13 who indicated that lactation counseling increased rates of milk expression without increasing levels of maternal stress.
The other uniqueness of this intervention was its flexibility. The subgroup analysis indicated that the cesarean mothers, who were the lowest at baseline at 12% within 6-12 h, were on par with the vaginal delivery mothers after the intervention at 54.5% and 58.1%, respectively (P = .23). Likewise, the interventions had similar results in both urban and rural background mothers, at 56.63% and 56.5%, respectively (P = .94).
While our findings are encouraging, they also underscore the need for sustained efforts to address breastfeeding barriers. During the later phases of the study, external factors, such as hospital renovations and workforce reductions, caused a slight decline in milk expression frequencies. These challenges highlight the importance of integrating such interventions into routine NICU workflows to ensure long-term sustainability.
Finally, it contributes to a growing body of evidence supporting the use of QI methodologies in neonatal care. According to Bagga et al., 5 expressed breast milk rates increased from 46% to 73% after structured prenatal counseling and indicated that incentives motivated mothers. Kositamongkol et al. 14 have pointed out the motivational effects of providing incentives. The current study did not offer incentives, but wrist tags were effective motivators. In a similar fashion, Takako et al. 8 increased breastfeeding rates by threefold by using Spatz’s 10-step strategy while highlighting the impact of holistic methods on neonate outcomes.
The interventions implemented in this study were low-cost, resource-adaptable, and designed to integrate into existing NICU workflows without significant infrastructural changes. This lends the findings a high degree of external validity, particularly for resource-constrained tertiary NICUs across low- and middle-income countries (LMICs). The use of simple tools—such as pumping schedules, culturally adapted educational posters, and routine nurse-led support—makes this model replicable and scalable to other clinical settings aiming to improve breastfeeding practices in preterm infants.
Limitations
Despite its successes, this study has limitations. The cohort included a few preterm neonates born before 30 weeks of gestation, and long-term outcomes, such as sustained breastfeeding practices and their effects on infant health, were not assessed. Documentation gaps during busy NICU shifts occasionally hampered data accuracy. Future studies should focus on overcoming these challenges and exploring the scalability of these interventions across diverse healthcare settings. This study did not analyze the volume of milk expressed per session, as such data were not systematically documented. This is an important metric for lactation adequacy and should be considered in future QI efforts to complement expression frequency.
Although the interventions showed promising results in enhancing early colostrum expression and exclusive breastfeeding rates, the sustainability phase in this study lasted for only four-and-a-half months (February-May 2024). Given the complexity of behavioral change and institutional adoption, this duration may be insufficient to establish true long-term sustainability. QI literature generally recommends follow-up periods of at least 8-12 months to evaluate the durability of interventions. As this was a time-bound study, we acknowledge the short follow-up as a limitation, and future studies should consider extended post-intervention tracking to assess sustainability over a longer duration.
Another limitation of this study was the absence of predefined balance indicators to assess unintended consequences. Parameters such as neonatal hypothermia rates, sepsis incidence, NICU length of stay, or mortality were not systematically recorded. These are important to ensure that improvement in one domain does not come at the cost of overall clinical care. Future QI initiatives should incorporate balance measures to comprehensively evaluate both benefits and potential risks.
Conclusion
This new study showed that QI initiatives using inexpensive interventions, including lactation counseling, breast pumps, wrist tags, and posters, can improve the initiation of breastfeeding and the exclusive breastfeeding rate at the time of discharge. It is always better to move towards an intensive QI activity. There are multiple barriers related to breastfeeding that need to be minimized in all sections, which would be easy in the event of QI activity. The proportion of mothers performing colostrum expression within 6 h increased significantly from 15.57% to 56.63% (P < .001), and exclusive breastfeeding improved from 49.63% to 85.68% (P < .001). These results reveal how QI strategies can counteract breastfeeding barriers in the context of NICUs. The strategies were effective, cutting across delivery mode and mothers’ background-based disparities. In discussing some of these major barriers, there is much scope for providing a structured solution that can eventually aid neonates in their health status and maternal self-confidence. Strengthening it by further covering the long-run results may yield a better situation in neonates and their mother’s health state as well. Future studies should incorporate longer follow-up periods to assess the sustainability and institutionalization of such interventions in real-world settings.
Footnotes
Authors Contribution
Jyoti More: Conceptualized the study and its design. Conducted data collection and performed preliminary statistical analyzes. Drafted the manuscript, focusing on the introduction, methods, and results sections. Ensured the accuracy and integrity of the data presented in the manuscript.
Sourabh Singh: Supervised the study design and execution. Provided critical feedback and revisions to the manuscript, particularly in the discussion and conclusion sections. Managed the submission process and communication with the journal as the corresponding author. Reviewed and approved the final manuscript for submission.
Arjun Verma: Assisted in literature review and data interpretation. Provided expert input on the (specific domain/topic, e.g., statistical methodology or clinical relevance). Contributed to manuscript editing and alignment with journal guidelines.
Madhu Mathur: Participated in data acquisition and organization. Provided substantial revisions and suggestions for improving the (specific sections, e.g., methodology or results discussion). Verified the references and formatted the manuscript.
Aril Bhatia: Assisted with advanced statistical analyzes and data visualization. Critically reviewed the manuscript for intellectual content and clarity. Contributed to the supplementary materials and appendices (if applicable).
Declaration of Conflicting Interests
The authors declared no conflict of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance for the study was obtained from the Institutional Ethics Committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from the participants for the conduct of the study.
Supplementary Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.