
Abstract
Background
Intraventricular hemorrhage (IVH) is the most common intracranial bleeding in preterm neonates and is linked to significant long-term neurodevelopmental morbidity. Routine cranial ultrasound (cUSG) screening recommendations, along with data on IVH prevalence and risk factors in India—especially in late preterm infants—are limited.
Objectives
This study aimed to determine IVH prevalence across preterm gestational ages (<37 weeks), identify maternal and neonatal risk factors for IVH, and evaluate IVH burden in late preterms in a tertiary care neonatal intensive care unit in Western Maharashtra.
Methods
In this single-center, prospective observational study from December 2020 to February 2022, 421 preterm neonates admitted within 24 h of birth received cUSG between days 4 and 7 of life. IVH was graded using the Papile classification. Maternal and neonatal data were collected via standardized forms. IVH prevalence was calculated, and univariate and multivariate logistic regression analyses identified independent risk factors. Late preterm infants (34-36 + 6 weeks) were analyzed separately.
Results
Of 421 preterm neonates, overall IVH prevalence was 28.27%, highest in those <28 weeks (62.5%) and birth weight <1,000 g (55.1%). IVH grades were: I (14.7%), II (10.7%), III (2.1%), IV (0.7%); 6.7% had other central nervous system abnormalities. Multivariate analysis showed weight (adjusted OR 2.13; 95% CI 1.27-3.56; P = .004), mechanical ventilation (adjusted OR 2.10; 95% CI 1.15-3.84; P = .016), and early-onset sepsis (adjusted OR 1.81; 95% CI 1.07-3.08; P = .027) as independent predictors. In late preterm neonates (n = 233), IVH prevalence was 19.3%, with birth weight <1,500 g (adjusted OR 5.35; 95% CI 1.90-15.07; P = .002) and mechanical ventilation (adjusted OR 3.21; 95% CI 1.24-8.31; P = .016) as independent risk factors.
Conclusions
IVH is a major complication across preterm ages, affecting nearly one-fifth of late preterm infants. Prevalence in <32 weeks neonates matches that of developed countries. Low birth weight, mechanical ventilation, and early sepsis heighten risk. Routine cUSG screening should include late preterm neonates, and preventing hemodynamic instability and sepsis could reduce IVH and neurodevelopmental issues.
Introduction
According to estimates, approximately 13.4 million neonates were born preterm (less than 37 weeks) worldwide in 2020. Southern Asia and Sub-Saharan Africa accounted for more than half (55.6%) of these preterm births, with each region contributing around 28.7%. Notably, India alone accounted for 13% of the total preterm births globally, highlighting the significant burden of preterm birth in this region. 1 Preterm neonates are at risk of various complications, like respiratory distress syndrome (RDS), bronchopulmonary dysplasia, patent ductus arteriosus (PDA), necrotizing enterocolitis, intracranial bleeding, and others. The most common type of intracranial bleeding in preterm neonates is germinal matrix or intraventricular hemorrhage (GMH-IVH). The prevalence of GMH-IVH varies as per gestational age (GA) and is inversely proportional to GA. The prevalence of IVH in very low birth weight infants in studies from different countries ranged from 15% to 70% among preterm neonates. 2 The neonates with IVH are predisposed to long-term complications, which include intellectual disability, impairment in executive and motor functioning, poor academic skills, and the development of cerebral palsy. 3 Identifying preterm infants who are at high risk of IVH and then neurodevelopmental impairment is critical to plan appropriate follow-up and rehabilitation programs and to reduce the burden of childhood disability.
Cranial ultrasound (cUSG) can detect an IVH with high sensitivity and specificity of 96% and 94%, respectively, 4 and allows early bedside detection of most major intracranial lesions, which are known to be the best predictors of cerebral palsy in preterm infants. The American Academy of Pediatrics suggests that all newborns with a GA of less than 30 weeks should undergo routine cUSG by the seventh or tenth day of life, and newborns with a GA of more than 30 weeks if they have any risk factors for brain injury, like abruptio placentae, received resuscitation, severe acidosis, and others. 5 Similarly, the Canadian Pediatric Society recommends routine cUSG in all preterm neonates less than 32 weeks of gestation and in neonates born between 32 and 37 weeks if they have any risk factors for intracranial hemorrhage (ICH). 6 In India, cUSG was proposed to be done for neonates <32 weeks and for neonates between 32 and 34 weeks with risk factors. 7
Despite its clinical significance, there is a paucity of data on the prevalence of intracranial abnormalities, particularly IVH, in preterm neonates in India. Available studies report a prevalence of IVH ranging from 13.3% to 18%.8-10 However, these studies primarily focused on very preterm neonates, excluding late preterm babies, who are also susceptible to IVH and are not routinely included in standard cUSG screening protocols. Late preterm neonates may still be vulnerable to IVH, particularly in the presence of risk factors such as low birth weight, respiratory distress, and sepsis. This knowledge gap prompted our study, which aimed to determine the prevalence of IVH in preterm neonates, identify risk factors associated with IVH, and assess the disease burden of IVH in late preterm neonates within a tertiary care neonatal intensive care unit (NICU) setting as well.
Methods
This was a single-center, prospective observational study that was conducted over 15 months, between December 2020 and February 2022, in a tertiary-care teaching hospital in Western Maharashtra. The study was started after obtaining institutional ethics committee approval. All preterm neonates (GA <37 weeks) admitted within 24 h of birth to the NICU or the postnatal ward were included in the study. Extramural neonates who were admitted within the first 24 h of life were also included to reflect the real-world patient profile of a tertiary-care referral NICU. Neonates with major congenital anomalies or neonates whose parents refused to give consent were excluded. During the study period, all eligible neonates underwent screening cranium ultrasound (sagittal and coronal views) by a single trained radiologist after obtaining written informed consent. cUSG was performed at the bedside between days 4 and 7 of life by a trained radiologist using a Philips Affiniti 50G ultrasound machine equipped with a curvilinear probe operating at a frequency range of 1-6 MHz. The Papile grading system for IVH was used for grading severity. Screening ultrasounds were performed earlier than scheduled if specific indications were present. If IVH was identified, the screening protocol was extended on an individual basis, taking into account the severity of the IVH. The most severe grade of IVH observed was used to calculate prevalence. Additional follow-up scans were performed only in cases where IVH was detected or when clinically indicated based on the neonate’s condition.
Maternal and neonatal risk factor details were collected from case record forms. Maternal risk factors included gravida status, pregnancy-induced hypertension (PIH), diabetes mellitus, thyroid disorders, toxoplasmosis, other infections, rubella, cytomegalovirus, and herpes simplex virus (TORCH) infections, infertility treatment, and antenatal steroid exposure. Neonatal risk factors included birth weight, GA, RDS, requirement of surfactant therapy, need for respiratory support (continuous positive airway pressure [CPAP] or mechanical ventilation), pneumothorax, persistent pulmonary hypertension, hemodynamically significant PDA, treatment for PDA, early-onset sepsis (suspected or proven), thrombocytopenia, coagulation abnormalities, shock, requirement for fluid boluses, inotropic support, and resuscitation at birth. Resuscitation at birth was defined as the requirement for positive pressure ventilation in the delivery room, including bag-mask ventilation or bag and tube ventilation.
Based on the findings of a previous study, 11 the sample size was calculated using the formula n = Z2pq/d2, where p = 26.9% (expected prevalence), q = 73.1%, Z = 1.96 for 95% confidence interval (CI), and d = 5% allowable error. The minimum required sample size was calculated to be 303. However, we included all eligible neonates during the study period, resulting in a final sample size of 421.
Statistical Analysis
All data were analyzed using Statistical Package for the Social Sciences (SPSS) version 28.0. Continuous variables were summarized with descriptive statistics (means and standard deviations or medians and interquartile ranges as appropriate), and categorical variables were expressed as frequencies and percentages. Univariate logistic regression was performed to estimate crude odds ratios (ORs) with 95% CIs for each potential risk factor. Variables with P < .05 in univariate analysis were entered into a multivariate logistic regression model to calculate adjusted odds ratios with 95% CIs, identifying independent predictors of IVH. All tests were two-tailed, and a P value < .05 was considered statistically significant. Continuous and categorical comparisons maintained a significance threshold of 5%.
Results
A total of 897 neonates were delivered intramurally during the study period, of which 301 (33.5%) were preterm. Also, 504 neonates delivered extramurally were admitted, of which 186 (36.9%) were preterm. A total of 421 neonates were enrolled in the study. The enrollment in the study is shown in Figure 1.
Study Flow.
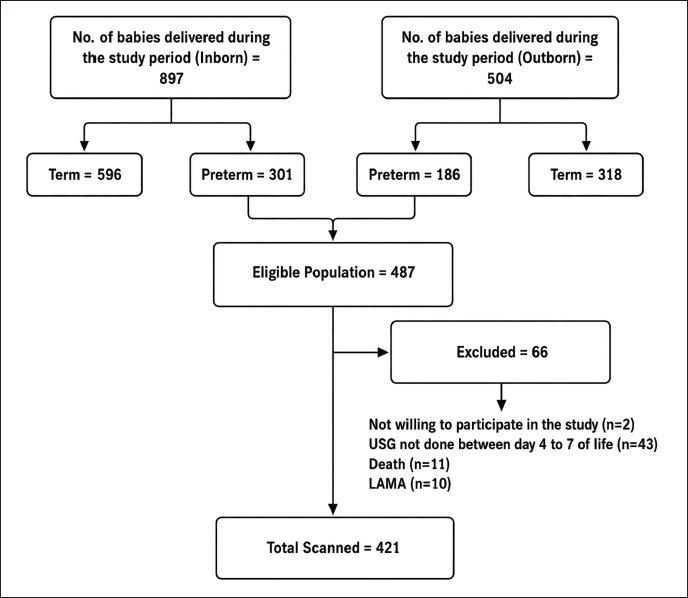
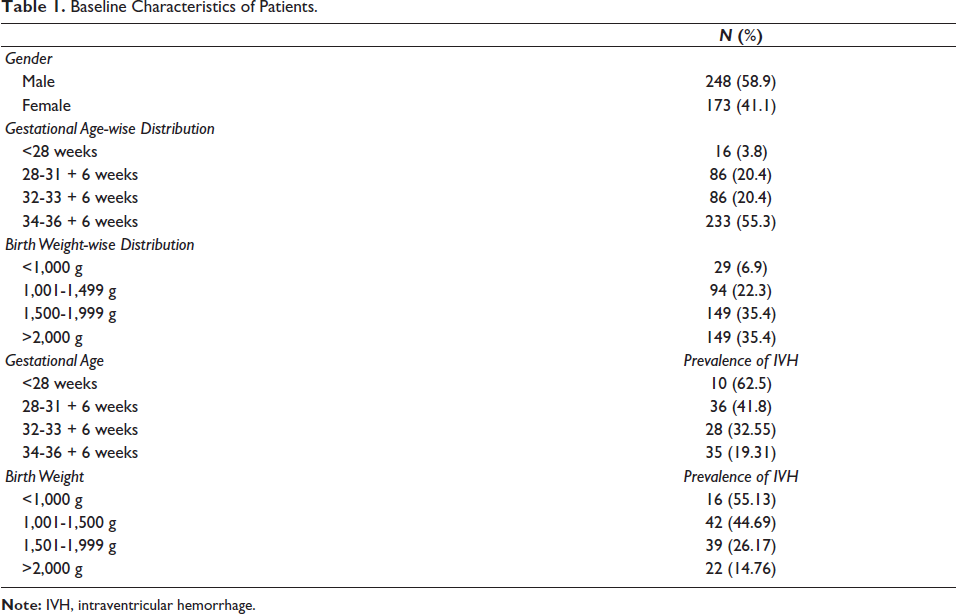
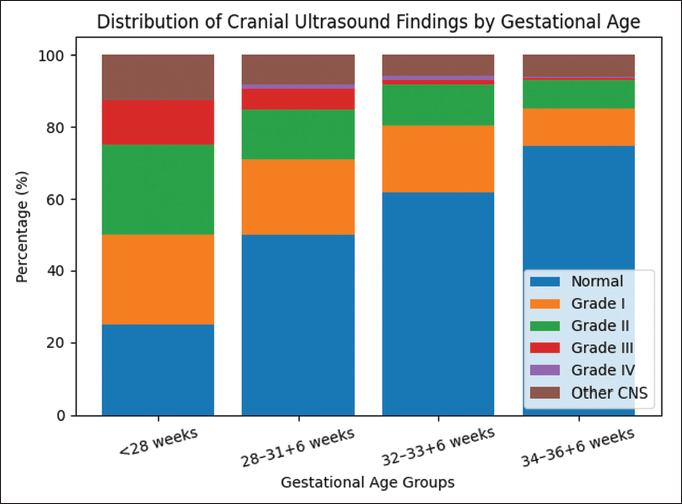
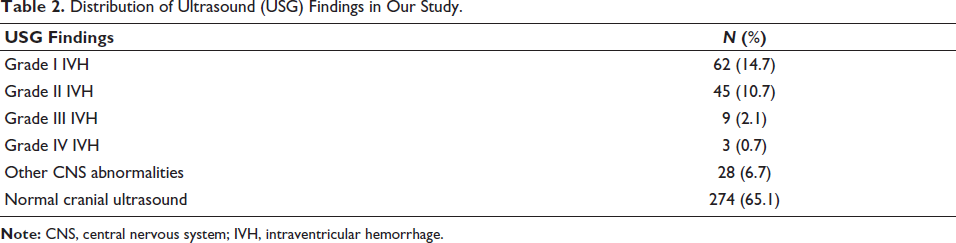
Table 1 shows baseline characteristics and the prevalence of IVH according to GA and weight. The prevalence of IVH in late preterm infants was 19.31%. Table 2 shows the distribution of IVH according to the Papile grading system, with 14.7% of cases having Grade I IVH, 10.7% having Grade II IVH, 2.1% having Grade III IVH, and 0.7% having Grade IV IVH. Additionally, 6.7% of cases had other central nervous system (CNS) abnormalities, while 65.1% had normal cUSG. The majority of neonates with normal cUSG belonged to the late preterm GA group (34-36 + 6 weeks) (Figure 2). The prevalence of IVH was highest in the <28 weeks of GA group (62.5%) and the <1,000 g birth weight group (55.13%). The prevalence of IVH decreased as GA and birth weight increased (Table 3).
Baseline Characteristics of Patients.
Distribution of Cranial Ultrasound Findings by Gestational Age.
Distribution of Ultrasound (USG) Findings in Our Study.
Distribution of Intraventricular Hemorrhage (IVH) as Per Birth Weight and Gestational Age.
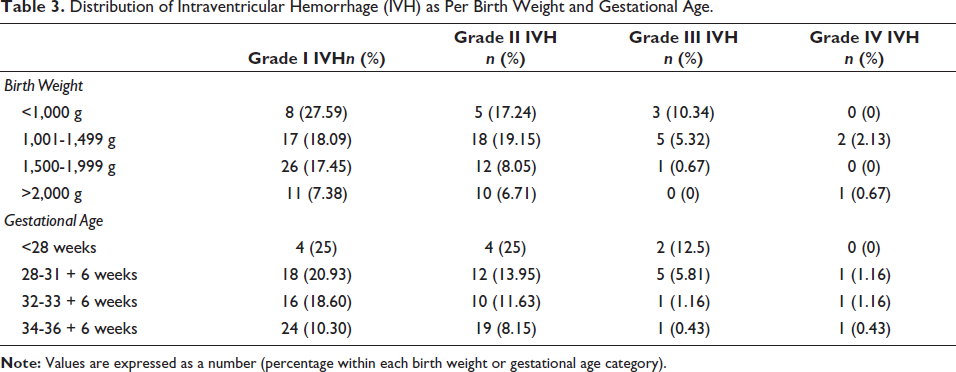
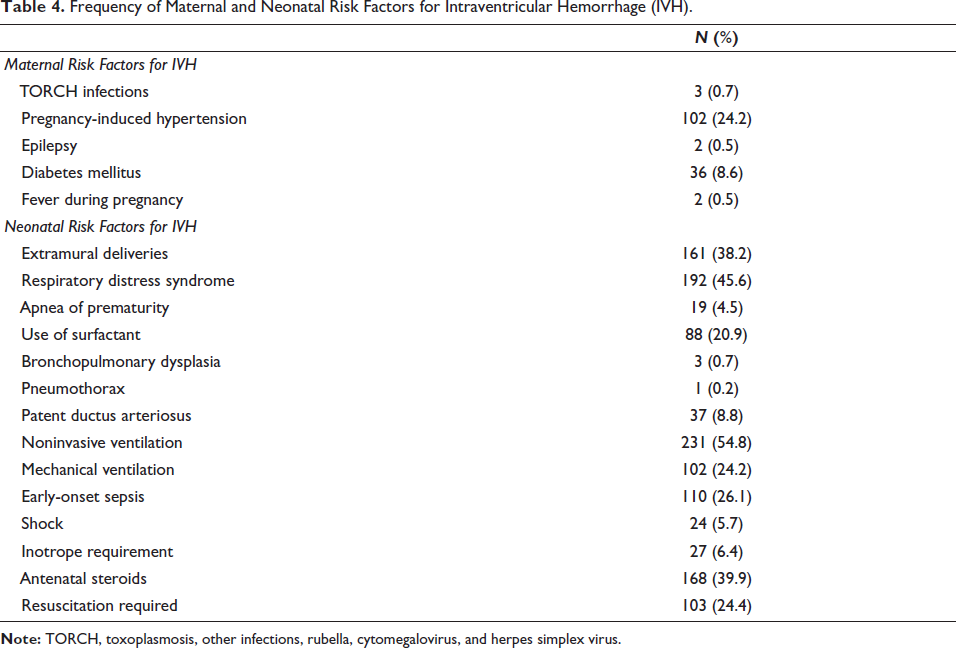
Table 4 shows the frequency of maternal and neonatal risk factors for IVH. Overall, in preterm neonates, on univariate analysis of risk factors, neonates having birth weight <1.5 kg, neonates requiring resuscitation, mechanical ventilation/CPAP, neonates with RDS, PDA, early-onset sepsis, shock, and requiring inotropic support had an increased OR of developing IVH. Other factors, like gender variability, intramural/extramural deliveries, mode of delivery, parity of the mothers, mothers having PIH, TORCH infections, and epilepsy, did not show any relationship with IVH. On multivariate analysis, weight <1.5 kg, neonates requiring ventilation, and early-onset sepsis had increased odds of developing IVH (Table 5). Although multiple variables showed significant associations with IVH on univariate analysis, only variables that remained significant on multivariate analysis were considered independent predictors.
Frequency of Maternal and Neonatal Risk Factors for Intraventricular Hemorrhage (IVH).
Univariate and Multivariate Logistic Regression Analysis of Risk Factors for Intraventricular Hemorrhage (IVH).

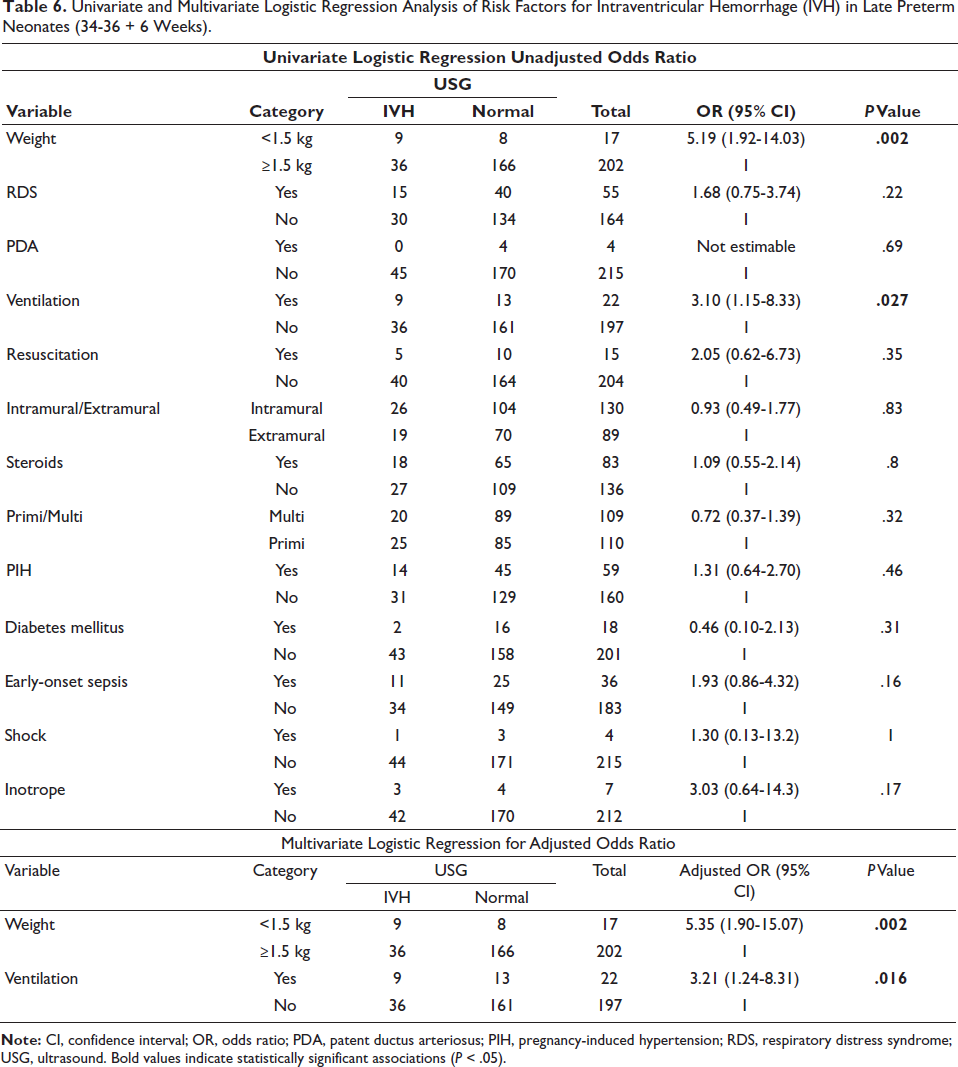
Table 6 shows the univariate and multivariate analyses of late preterm neonates. Our study showed that in late preterm birth, neonates who required ventilation and having a birth weight of <1,500 g had high odds of developing IVH, and on multivariate logistic regression analysis, both birth weight <1,500 g and neonates requiring ventilation were independently associated with increased odds of IVH.
Univariate and Multivariate Logistic Regression Analysis of Risk Factors for Intraventricular Hemorrhage (IVH) in Late Preterm Neonates (34-36 + 6 Weeks).
Discussion
Our study revealed an inverse correlation between GA and the prevalence of IVH, with a significantly higher incidence among extremely low birth weight neonates. Additionally, we identified several key risk factors associated with IVH development, including low birth weight, mechanical ventilation, and early-onset sepsis. Notably, our findings also indicated a substantial prevalence of IVH (19.3%) among late preterm neonates, highlighting the importance of vigilant monitoring in this population.
The prevalence of IVH in our study was 28.27% when ultrasound was done on days 4 and 7, which is consistent with other studies that reported a prevalence between 20% and 59%.12-15 Early ultrasound (on day 1) may miss subtle bleeding (especially lower-grade hemorrhages), because blood may still be in the process of clotting or dispersing, whereas late ultrasound (days 4-7) allows time for hemorrhages to become more apparent and for additional bleeding or progression to occur, thereby improving detection and allowing for more accurate grading. In some cases, what appears as a low-grade hemorrhage on an early scan might later be seen to extend or change in character, while some lesions may resolve over time. So, we have chosen to screen the neonates in the late period.
Our study revealed an inverse relationship between GA and the incidence of IVH, consistent with previous findings. Although extreme preterm neonates comprised only 3.8% of our study population, we observed a significant decrease in IVH incidence with increasing GA. This trend aligns with the results of earlier studies by Egwu et al., 2 Handley et al., 16 Sandler et al., 17 and Kadri et al., 18 which also reported a decline in IVH prevalence with advancing GA. The increased incidence of IVH with decreasing GA can be attributed to the fragile microvasculature of the germinal matrix (GM) and immature cerebral autoregulation in premature neonates. The GM’s involution toward the caudothalamic groove begins in the late second trimester and is nearly complete by 32 weeks of gestation. Before this, fluctuations in cerebral blood flow (CBF) can cause repeated ischemia-reperfusion events. At the same time, sudden increases in CBF can put excessive strain on the fragile GM vessels, leading to hemorrhage. As a result, the risk of IVH increases significantly with decreasing GA. 19 The relationship between IVH prevalence and birth weight mirrors that of GA. Our study found that the incidence of IVH increased significantly with decreasing birth weight, consistent with previous research by Kadri et al. 18 and Macleod et al. 20 This inverse correlation underscores the vulnerability of low birth weight neonates to IVH.
We did not find any relationship between gender and IVH. In a study done by Mohamed and Aly [OR = 1.15 (1.11-1.19)], 21 Cuestas et al. [OR = 3.4 (1.8-6.4)], 22 they have found that male neonates had a high preponderance for the prevalence of IVH. This was attributed to the finding that male gender was associated with a higher incidence of RDS, higher rates of death, and chronic lung disease.
In our study, intramural and extramural deliveries did not show any difference in the prevalence of IVH. Various studies have shown that the incidence of IVH in extramural neonates was higher, ranging from 9% to 23%.23, 24
Both early- and late-onset neonatal sepsis, shock from any cause, and the need for inotropic support have been associated with an increased prevalence of IVH. Hemodynamic instability and the rapid blood pressure fluctuations that occur during shock or as a result of inotropic support may lead to the rupture of fragile cerebral vessels, thereby increasing the risk of IVH. In our study, sepsis was associated with a higher likelihood of developing IVH [OR = 2.82 (1.76-4.54)], and shock similarly showed a significant increase in odds [OR = 3.61 (1.47-8.87)]. These findings align with other studies; for example, Lehner et al. reported that neonates in shock had a significantly higher risk of IVH (P < .01). 25 In a large study by Huang et al. involving 13,605 neonates of less than 37 weeks’ gestation, early-onset sepsis was linked to increased odds of IVH [OR = 2.18 (1.58-2.99)], 26 while Lee et al. found that very low birth weight infants with early-onset sepsis had a heightened risk [OR = 2.10 (1.27-3.48)]. 27 Additionally, Lee et al. demonstrated that neonates receiving inotropic support had an increased odds of IVH [OR = 3.70 (1.16-11.84)], 28 a finding corroborated by Abdul Aziz et al. in a study of 497 infants under 29 weeks’ gestation and with birth weights less than 1,500 g, where inotropic support within the first 72 h was associated with severe IVH [OR = 4.2 (1.9-8.9)]. 29 Similarly, Lee et al. observed that among 1,044 infants born at less than 34 weeks’ gestation, those receiving inotropes had increased odds of developing IVH [OR = 3.70 (1.16-11.84)], 28 and Alotaibi et al. reported that in 640 infants below 33 weeks’ gestation, the use of inotropes elevated the risk of IVH [OR = 2.60 (1.20-5.62)]. 30
In our study, on multivariate analysis, low birth weight, neonates requiring ventilation, and neonates having early-onset sepsis were independently associated as risk factors for IVH. Similar to a recently published meta-analysis by Bao and Huang, 31 while several variables, such as low birth weight, RDS, PDA, resuscitation, sepsis, shock, and inotrope requirement, showed significant associations with IVH on univariate analysis, these did not all remain significant after multivariate adjustment. This suggests that their effects may be interrelated and mediated through overall illness severity and hemodynamic instability.
Although late preterm neonates are traditionally considered at lower risk for IVH, they are not entirely protected. The GM, though undergoing involution, may still persist and remain vulnerable to hemorrhage. Furthermore, late preterm infants frequently encounter clinical stressors such as respiratory distress, sepsis, and hemodynamic instability, which can result in fluctuations in CBF in the setting of still-maturing autoregulatory mechanisms. Our study yielded a notable finding: a significant proportion (19.3%) of late preterm infants developed IVH. So, this contrasts with the traditional view that IVH is rare in this population. Previous studies have reported varying incidence rates of IVH in late preterm infants. For example, a Swedish study by Bonnevier et al. found an overall IVH incidence of 0.1% among 14,030 late preterm singleton infants using medical records from the Perinatal Revision South Quality Register. 32 In contrast, a US-based study by Sandoval Karamian et al. detected ICH using magnetic resonance imaging and reported that 10.7% of late preterm neonates developed ICH, with the majority having IVH. 33 Another study, conducted in Syria by Kadri et al. in 2008, found an even higher incidence of IVH (23.5%) among late preterm neonates. 18 The disparity in IVH incidence rates between developed and low- and middle-income countries (LMICs) is likely multifaceted. Several factors may contribute to these differences, including variations in antenatal care and delivery room practices, and differences in the incidence of RDS and sepsis. The other possibility could be the inconsistent application of cUSG screening protocols for late preterm neonates without risk factors, potentially leading to underdiagnosis and underreporting of IVH in many regions. Given the knowledge gaps and variability in IVH incidence rates, particularly in LMICs, larger prospective studies are warranted to determine the prevalence of IVH in late preterm neonates. The findings of such studies may necessitate updates to existing guidelines for IVH screening. Early detection of IVH is crucial for prioritizing infants who require early intervention, ultimately leading to improved long-term neurological outcomes. Our study’s findings underscore the need for larger studies in India to screen late preterm neonates for IVH detection. This research could inform the development of national guidelines for cUSG screening in neonates, enhancing the standard of care for this vulnerable population.
Despite significant advancements in neonatal care over the past few decades, IVH remains a persistent and major morbidity among preterm infants. A recent comprehensive systematic review of 64 studies involving 9,633 preterm infants found that the prevalence of IVH has remained relatively unchanged since 2007, with a slight decline from 36% to 31%. 34 This stagnation in IVH prevalence may be attributed to improved survival rates of extremely premature neonates, who are at higher risk of developing IVH. Another possible explanation is the inconsistent application of preventative measures aimed at reducing IVH. However, it is essential to acknowledge that even with optimal preventative strategies, IVH may not be entirely avoidable, highlighting the need for continued research to mitigate this complication.
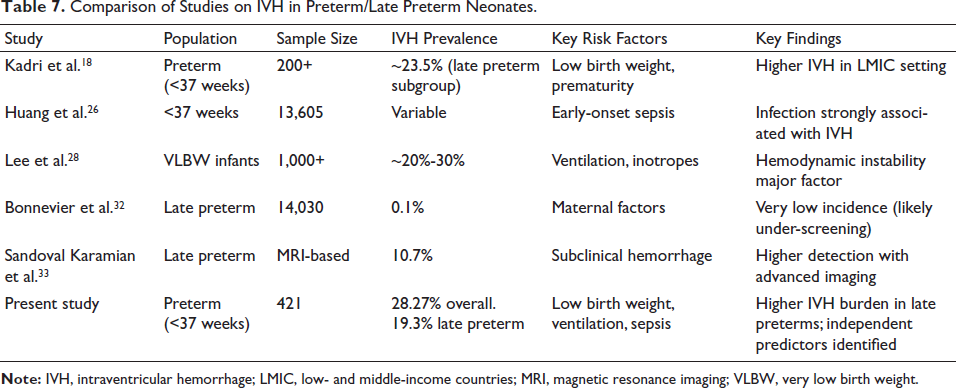
A comparison of our findings with previous studies is summarized in Table 7.
Comparison of Studies on IVH in Preterm/Late Preterm Neonates.
In conclusion, IVH persists as a prevalent complication affecting preterm infants. Due to its multifactorial etiology, eliminating IVH may be challenging. Notably, our findings contradict the long-held assumption that IVH is rare in late preterm infants. Instead, we demonstrate that this population is also vulnerable to developing IVH, highlighting the need for revised guidelines that acknowledge this risk. Routine cUSG screening protocols should be updated to include late preterm infants, ensuring that this cohort receives timely and appropriate evaluation. By expanding screening to this population, we can identify high-risk neonates earlier, facilitating prompt intervention and potentially improving long-term neurological outcomes. As such, it is essential to prioritize the development and implementation of evidence-based guidelines for IVH screening, diagnosis, and management in preterm infants, including those born late preterm.
Limitations
This study has several limitations that should be acknowledged. First, as a single-center study, the findings may not be generalizable to other populations. Additionally, the proportion of extremely premature and extremely low birth weight neonates was relatively low, which may limit the applicability of our findings to these high-risk groups. We did not systematically assess transport-related variables in extramural neonates, which may have influenced the IVH risk. Additionally, the study population included a higher proportion of neonates with a GA of >28 weeks, particularly late preterm infants, which may limit the generalizability of the findings to extremely preterm populations. Furthermore, due to financial constraints, we were unable to perform serial ultrasound scans of the cranium or scans at term-equivalent GA, which may have provided valuable additional insights. Lastly, our study did not include neurological and developmental follow-up, which would have been essential to assess the long-term outcomes of IVH in this population.
Conclusion
Our findings confirm that IVH remains a serious problem in preterm neonates, with a clear inverse association between GA, birth weight, and IVH risk. Notably, the high prevalence of IVH was seen not only in extremely preterm and very low birth weight newborns, but also in late preterm neonates, contrary to the widespread belief that IVH is uncommon in this population. Multivariate analysis found weight, mechanical ventilation, and early-onset sepsis to be independent risk factors for IVH, emphasizing the crucial role of postnatal hemodynamic instability in maintaining cerebral integrity.
These findings underline the importance of thorough and inclusive cUSG screening strategies for late preterm newborns, ensuring early discovery and timely intervention. Given the variation in IVH occurrence across different settings and the long-term morbidity associated with IVH, there is a dire need to examine and revise current screening standards, particularly in LMICs such as India. Implementing comprehensive, evidence-based screening and management measures could play a critical role in reducing the long-term neurological consequences of IVH, hence improving overall outcomes for this vulnerable population.
Authors’ Contributions
BK, NM: Management of the patients; BK, NM: Collected the data, reviewed the literature, and drafted the first version of the manuscript; BK, NM, AK, SL: Conceptualized the study, reviewed the literature, revised the manuscript, and critically reviewed the manuscript. All authors contributed to the drafting of the manuscript and approved the final version of the manuscript; NM: Shall act as guarantor of the article.
The manuscript has been read and approved by all the authors, the requirements for authorship have been met, and each author believes that the manuscript represents honest work.
Footnotes
Declaration of Conflict of Interests
The authors declared no conflict of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Clearance from the ethical committee received (IEC No.: BVDUMC/IEC/49).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the parents/legal guardians of all neonates included in the study prior to enrollment, in accordance with institutional ethical guidelines.