
Abstract
Background
Neonatal hyperbilirubinemia remains a significant clinical concern due to its association with acute bilirubin encephalopathy and long-term neurological sequelae. Double volume exchange transfusion (DVET) is implemented as a life-saving intervention when intensive phototherapy fails or when bilirubin levels reach exchange thresholds. Even though new advances have been made in neonatal care, DVET continues to be performed in tertiary care neonatal intensive care units (NICUs), especially in settings with severe hemolytic disease and cases with late presentations.
Objective
To describe the clinical characteristics, indications, procedural details, outcomes, and complications associated with DVET performed for severe neonatal hyperbilirubinemia in a tertiary care NICU.
Methods
This retrospective case series included all neonates who underwent DVET for severe hyperbilirubinemia in our tertiary care NICU over a period of 6 months. Data collected included demographic characteristics, gestational age, birth weight, hyperbilirubinemia’s etiology, pre- and post-exchange total serum bilirubin levels, procedural details, complications, and short-term outcomes, including neurological status at discharge.
Results
Our case series demonstrated a mean immediate reduction of 45.3% in TSB levels, effectively following DVET. Common etiologies included ABO incompatibility, glucose-6-phosphate dehydrogenase deficiency, Rh alloimmunization, and idiopathic causes. Complications included hypocalcemia, thrombocytopenia, and transient respiratory events. Rebound hyperbilirubinemia requiring repeat exchange occurred in three cases. There was no mortality, and two of the survivors showed persistent neurological abnormalities at discharge.
Conclusion
Double volume exchange transfusion was effective in reducing total serum bilirubin levels in neonates with severe hyperbilirubinemia but was associated with metabolic and hematologic complications.
Keywords
Introduction
Neonatal jaundice affects more than 60% of term infants, and more than 80% of newborns develop visible jaundice during the first week of life.1, 2 Though most of these cases are physiological and self-limiting, severe hyperbilirubinemia can lead to acute bilirubin encephalopathy (ABE) and kernicterus, which further results in permanent neurological sequelae, including choreoathetoid cerebral palsy, auditory neuropathy, and developmental delays. 2
With the widespread availability of LED-based devices for administering intensive phototherapy and improved early detection strategies, such as prenatal screening, anti-D prophylaxis, and early postnatal monitoring, the management of neonatal hyperbilirubinemia has evolved significantly over the past few decades, and the frequency of exchange transfusion has declined significantly in many developed countries. 3 Despite these advances, double volume exchange transfusion (DVET) remains one of the most crucial interventions in low- and middle-income countries where late presentations, severe hemolytic disease, and limited access to intensive phototherapy remain prevalent. DVET also becomes crucial when conservative measures fail or when total serum bilirubin (TSB) levels reach critical thresholds that pose an imminent risk of neurotoxicity. 4
DVET procedure involves replacing approximately twice the infant’s blood volume (typically 160-200 mL/kg) by alternately withdrawing and infusing small aliquots of blood, thus effectively removing bilirubin and antibody-coated red blood cells. 5 The procedure helps in achieving an immediate reduction in TSB levels of approximately 50%-60%, reducing bilirubin and potentially preventing progression of bilirubin neurotoxicity when performed before advanced encephalopathy develops. 6 Recent case series from tertiary NICUs report ABO incompatibility, Rh alloimmunization, glucose-6-phosphate dehydrogenase (G6PD) deficiency, and idiopathic etiologies to be the primary indications for DVET. 7
Despite the life-saving potential of DVET, significant complications are associated with it, some of which include hypocalcemia, thrombocytopenia, hypoglycemia, electrolyte disturbances, apnea, seizures, catheter-related complications, and, in rare cases, mortality. 8 In order to avoid and manage these complications, the procedure requires specialist expertise, meticulous technique, and intensive monitoring.
The following case series aims to describe the clinical characteristics, procedural details, outcomes, and complications associated with DVET performed in cases of neonates affected with severe neonatal hyperbilirubinemia at our tertiary care NICU.
Materials and Methods
Study Design and Setting
This retrospective case series was conducted at a tertiary care NICU with 17 beds, serving as a regional referral center for high-risk neonates. The study included all neonates who underwent DVET for severe hyperbilirubinemia over a period of 6 months. The series was conducted using anonymized patient data after obtaining a waiver from the Institutional Ethics Committee as per institutional policy. Administrative approval for data access was obtained from the Head of Department prior to data collection.
Inclusion Criteria
All neonates (term and preterm) who underwent at least one DVET during the 6-month study period.
Age at admission: 0-28 days.
Documentation of pre-exchange and post-exchange TSB levels.
Exclusion Criteria
Neonates who underwent partial exchange transfusion only.
Incomplete medical records with missing essential data.
Indications for Exchange Transfusion
DVET was performed in accordance with American Academy of Pediatrics (AAP) 2022 guidelines for management of neonatal hyperbilirubinemia. 9
Exchange Transfusion Technique
Exchange transfusion was performed using a push–pull technique through an umbilical venous catheter. Even though isovolumetric techniques may reduce volume fluctuations, the push–pull technique continues to be routinely used in our unit because of its familiarity, requirement of minimal additional equipment, and allows close hemodynamic monitoring when performed by trained personnel under continuous monitoring. A double-volume exchange (160-180 mL/kg) was performed in aliquots of 5-10 mL using crossmatched reconstituted blood prepared from packed red blood cells and fresh frozen plasma in a 2:1 ratio. Each cycle involved withdrawal of blood over 1-2 min followed by infusion of an equal volume of donor blood to maintain hemodynamic stability. The total duration of the procedure ranged from 60 to 90 min. Continuous cardiorespiratory monitoring was maintained throughout the procedure. Blood glucose, serum calcium, and electrolyte levels were monitored during and after exchange transfusion, and prophylactic calcium gluconate was administered as per institutional protocol to prevent citrate toxicity.
Data Collection
Data were extracted from electronic medical records and included demographic, clinical, and laboratory parameters. Gestational age was determined based on first-trimester ultrasound when available or last menstrual period, and confirmed using the modified Ballard score in case a discrepancy existed.
Statistical Analysis
Descriptive statistics were used to summarize the data. Continuous variables were expressed as mean ± standard deviation or median with interquartile range, depending on distribution. Categorical variables were expressed as frequencies and percentages. Pre- and post-exchange TSB levels were compared using a paired t-test.
Results
Patient Characteristics
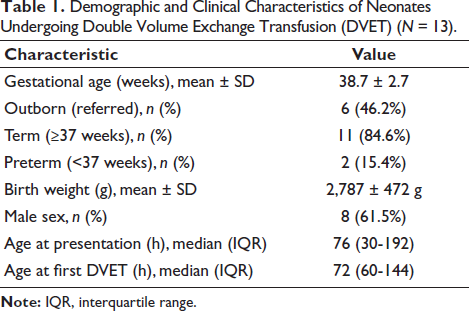
During the study period, a total of 13 neonates underwent DVET for severe hyperbilirubinemia at our tertiary care NICU. The demographic and clinical characteristics of the study population are summarized in Table 1.
Demographic and Clinical Characteristics of Neonates Undergoing Double Volume Exchange Transfusion (DVET) (N = 13).
Etiology of Hyperbilirubinemia
ABO incompatibility was the most common etiology (n = 9), followed by sepsis-associated causes (n = 7) and idiopathic/unknown factors (n = 7). Rh alloimmunization and G6PD deficiency were each identified in three cases. The sepsis-associated group included both culture-proven cases (such as MRSA) and probable clinical sepsis. In cases suspected of immune-mediated hemolysis, ABO incompatibility was diagnosed based on maternal–neonatal blood group mismatch along with clinical and laboratory evidence of hemolysis (including low hemoglobin, elevated reticulocyte count, and peripheral smear findings), with or without a positive direct antiglobulin test, as false-negative results may occur.
Clinical Presentation
Acute bilirubin-induced neurological dysfunction features were present in five neonates at presentation. Among these, three neonates had stage I ABE, and two neonates had stage II ABE. The two infants with persistent neurological abnormalities at discharge belonged to the stage II ABE category at admission.
Laboratory Parameters and Exchange Transfusion Details
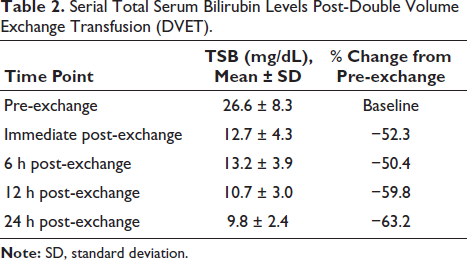
The mean pre-exchange TSB level was 26.6 ± 8.3 mg/dL (range: 5.1-44.6 mg/dL). Following DVET, the mean immediate post-exchange TSB was 12.7 ± 4.3 mg/dL, corresponding to a mean reduction of 45.3% ± 18.9%. The mean pre-exchange hemoglobin was 13.7 ± 2.2 g/dL, which increased to 14.1 ± 1.9 g/dL post-exchange. A total of three neonates required repeat exchange transfusion due to rebound hyperbilirubinemia (Table 2).
Serial Total Serum Bilirubin Levels Post-Double Volume Exchange Transfusion (DVET).
Temporal Pattern of Serum Bilirubin
A mild rise in mean TSB levels was observed at 6 h post-exchange, followed by a subsequent decline at 12 and 24 h. Rebound hyperbilirubinemia (defined as TSB rise >50% of initial reduction at 6 h) occurred in three neonates, necessitating repeat DVET. These infants had underlying hemolytic etiologies, including ABO incompatibility and G6PD deficiency, and presented at a later postnatal age compared to the rest of the cohort.
Complications
The most common complications were thrombocytopenia in 10 cases, respiratory events including apnea and desaturation in 6 cases, and hypocalcemia in 3 cases, which was transient and managed with supplementation. No cases of arrhythmia, hypotension, hypoglycemia, or necrotizing enterocolitis were observed in our cohort.
Outcomes
The median duration of hospital stay was 8.5 days (IQR: 5-15 days). At discharge, 11 neonates had normal neurological examination, while two neonates exhibited persistent abnormal neurological signs in the form of hypotonia, hypertonia, feeding difficulties, or ongoing seizures. All infants were advised to undergo long-term neurodevelopmental follow-up, given the risk of bilirubin-induced neurological dysfunction. There was no mortality in our cohort.
Discussion
This case series describes the continued necessity of DVET in specific clinical scenarios for neonates affected with severe neonatal hyperbilirubinemia at a tertiary care NICU. The series demonstrates that despite the high risks associated with DVET, it remains an effective intervention for reducing TSB levels rapidly, signified by mean reduction of 45.3% immediately post-procedure. Though the procedure is associated with significant metabolic and hematologic complications, most infants in our cohort (n = 11) demonstrated normal neurological examination at discharge.
The etiological distribution in our series is consistent with recent reports from tertiary centers worldwide. 7 ABO incompatibility emerged as the leading cause of severe hyperbilirubinemia in our series, reflecting its higher prevalence compared to Rh alloimmunization in the post-anti-D prophylaxis era. 3 G6PD deficiency in three cases signifies the importance of screening for this enzyme deficiency in populations with high prevalence, particularly in regions where newborn screening is not universal. 10
Despite a comprehensive workup, the significant number of cases with idiopathic etiology in seven patients highlights the limitations of current diagnostic approaches and suggests the potential role of unrecognized genetic or metabolic factors.
Our series is also signified by the high proportion of outborn neonates (n = 6) presenting with delayed referral and clinical signs of acute bilirubin encephalopathy (n = 5). The median age at presentation of 76 h and the presence of ABE signs in a significant subset points out to gaps in early recognition, inadequate availability of phototherapy facilities at peripheral centers, and delayed referral patterns. This observation is consistent with reports from other low- and middle-income countries where late presentation remains a major challenge. 4 Among outborn infants, ABO incompatibility was the most common identifiable etiology. Although some neonates had reportedly received phototherapy prior to referral, detailed documentation regarding duration and adequacy of phototherapy at peripheral centers was unavailable in retrospective records.
For inborn infants, universal predischarge bilirubin screening with risk stratification using the Bhutani hour-specific bilirubin nomogram is essential to identify infants at risk of subsequent severe hyperbilirubinemia before discharge. In contrast, for outborn infants, strengthening peripheral phototherapy services, ensuring early bilirubin measurement, and establishing clear referral pathways when exchange thresholds are approached are critical strategies to prevent late presentation with acute bilirubin encephalopathy.
The study shows that despite the high risks, DVET is effective in achieving rapid reduction in TSB levels, with a mean immediate reduction of 45.3%. The comparable reduction in TSB levels across different etiologies in our cohort likely reflects the intrinsic efficacy of exchange transfusion in removing bilirubin, rather than differences related to the underlying cause of hyperbilirubinemia.
In our series, rebound hyperbilirubinemia was observed in three neonates, all of whom had immune-mediated or enzymatic hemolytic etiologies. These infants presented at a later postnatal age and required repeat exchange transfusion, suggesting ongoing bilirubin production due to underlying hemolysis as a likely contributor to rebound. Rebound occurs due to redistribution of bilirubin from tissue compartments back into plasma and ongoing hemolysis in cases of alloimmune or enzymatic disorders. 11
In consonance with the available literature, the complication profile in our series highlights metabolic and hematologic disturbances as the most frequent adverse events. 8 Hypocalcemia is a well-recognized complication resulting from citrate in anticoagulated blood products binding to ionized calcium. Our protocol of prophylactic calcium gluconate infusion during the procedure likely prevented more severe manifestations of hypocalcemia, though biochemical hypocalcemia remained common.
Thrombocytopenia following exchange transfusion is likely multifactorial due to repeated removal of the infant’s blood, which may contribute to platelet loss and dilutional effects over successive cycles. In addition, the use of stored blood products may be associated with reduced platelet viability, and mechanical factors during repeated withdrawal and infusion may contribute to platelet destruction. Platelet consumption related to underlying illness and catheter-related factors may further contribute to thrombocytopenia in these infants. Further, mean hemoglobin levels increased post-exchange (14.1 vs. 13.7 g/dL), which shows that blood product selection and volume management were appropriate.
Respiratory issues, such as apnea and desaturation episodes, were observed in six neonates, underscoring the vulnerability of sick neonates during the procedure. These events may be associated with metabolic disturbances, handling stress, or the underlying severity of illness. With the declining frequency of exchange transfusion in the era of effective intensive phototherapy, opportunities for hands-on training and procedural experience among neonatal care providers have also reduced, which may contribute to variability in technical performance and complication rates. 3 Among the neonates, two cases were affected with catheter-related bloodstream infections. Therefore, there is a continued need for vigilance in aseptic technique despite standardized protocols.
Two infants in our cohort demonstrated abnormal neurological signs at discharge. Given the small number of affected cases, definitive conclusions regarding the neurological outcomes following DVET cannot be drawn. These findings may reflect bilirubin-induced neurological injury that had already occurred prior to intervention. 12 Infants with abnormal neurological findings had late presentation with clinical ABE, suggesting that timing of intervention rather than procedural efficacy likely influenced outcome.
Our case series findings are broadly consistent with recent reports from tertiary NICUs in various geographical settings. Patra and Mahapatra reported a 52.5% reduction in mean TSB levels following DVET, with comparable complication rates. 7 Further, another multicenter research study emphasized the continued importance of DVET in settings where late presentations occur, and there is limited access to intensive phototherapy. 4 Despite the above, comparison across studies is limited and constrained as there are variations in study populations, inclusion criteria, thresholds for exchange transfusion, and the definition of outcome.
Limitations
This study has several limitations that merit attention. Ours was a single-center retrospective case series, and it might not be suitable to generalize the findings in other settings due to variations in patient populations, resource availability, and practice patterns. Further, the control group was absent from our study, which precludes direct comparison of outcomes with alternative management strategies. Because of the retrospective nature of the study, there is apprehension that data collection was limited to information documented in electronic medical records, which could have led to potential underreporting of certain complications or incomplete capture of clinical details. It was difficult to assess the ultimate impact of DVET on developmental trajectories as long-term neurodevelopmental outcomes beyond hospital discharge were not available for this analysis. The study period may have spanned changes in clinical practice, blood banking protocols, or phototherapy equipment that could influence outcomes. Additionally, the sample size (13 cases) was relatively small, thus limiting the statistical power for subgroup analyses and identification of risk factors for adverse outcomes.
Conclusion
Double volume exchange transfusion was associated with frequent but manageable short-term complications, and neurological signs improved in a subset of infants following the procedure.
Footnotes
Consent for Publication
All necessary consent for publication was obtained by the authors.
Data Availability
All datasets generated and/or analyzed during the current study are available from the corresponding author on request.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Ethics Committee waiver was obtained as per institutional policy.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from all participants.