
Abstract
Background
Effective breastfeeding technique is vital for neonatal nutrition and well-being. Suboptimal breastfeeding technique might contribute to early neonatal morbidity. A structured breastfeeding counseling, provided to the mother within 24 h of childbirth, might lead to significant improvement in breastfeeding technique, as assessed using the LATCH score.
Objective
To evaluate the impact of structured breastfeeding counseling, which combines education, demonstration, hands-on support, and emotional encouragement within the first 24 h, on breastfeeding technique.
Methodology
This cross-sectional observational study was conducted at a tertiary care hospital in North India. The breastfeeding technique of 310 mothers was assessed within the first 24 h postpartum and after structured breastfeeding counseling, using the LATCH score. The pre- and post-counseling LATCH scores were compared. Descriptive statistics and paired t-test were used to evaluate score changes.
Results
Post-counseling, 97.1% of mothers achieved a LATCH score >8 compared to 3.9% pre-counseling, which was statistically significant (p < .0001).
Conclusion
Structured breastfeeding counseling, provided within 24 h of birth, significantly improves breastfeeding technique.
Introduction
Breastfeeding is universally acknowledged as the optimal method of infant feeding due to its unparalleled nutritional, immunological, and psychological benefits. The World Health Organization (WHO) recommends initiating breastfeeding within the first hour of birth and continuing exclusive breastfeeding for the first 6 months of life, followed by continued breastfeeding with appropriate complementary foods for up to 2 years or beyond.1, 2
Human breast milk is a dynamic, bioactive fluid that evolves with the infant’s age and health needs. It provides the ideal balance of macronutrients, micronutrients, growth factors, enzymes, and immunological components that promote infant survival and long-term health. 3 It contains secretory immunoglobulin A, lactoferrin, lysozymes, cytokines, and human milk oligosaccharides, which support gut maturation and immune development.4, 5 These components have been shown to reduce the incidence of diarrhea, pneumonia, necrotizing enterocolitis, and sudden infant death syndrome.6, 7
Beyond infectious disease prevention, breastfeeding contributes to neurodevelopment and emotional bonding. Numerous cohort studies have demonstrated a positive correlation between breastfeeding duration and improved cognitive performance in childhood and adolescence. 8 Furthermore, breastfeeding fosters maternal–infant bonding through oxytocin-mediated neuroendocrine mechanisms. 9
It also contributes to better maternal health by reducing postpartum hemorrhage and decreasing the risk of breast and ovarian cancers.10, 11 At a population level, increased breastfeeding rates correlate with reduced healthcare costs and improved public health outcomes, including reduced infant and under-five mortality rates. Increased breastfeeding practices may contribute to environmental sustainability by reducing the ecological impact associated with commercial formula manufacturing and distribution. 12
Despite overwhelming evidence, global breastfeeding indicators fall short of WHO targets. According to the 2022 UNICEF global nutrition report, only 44% of infants worldwide were exclusively breastfed during the first 6 months—far from the global nutrition target of 70% by 2030. 13 NFHS-5 data (2019–2021) from India revealed that only 42.6% of newborns were breastfed within the first hour, and 63.7% were exclusively breastfed up to 6 months. 14
One of the major contributors to early breastfeeding discontinuation is ineffective breastfeeding technique, particularly poor infant positioning and latching. 15 These issues may result in nipple pain, breast engorgement, and undue maternal anxiety, ultimately leading to supplementation using formula milk and/or early cessation of breastfeeding.16, 17 Importantly, these technical challenges are often correctable with early, structured lactation support.
Various tools have been developed to objectively assess the quality of breastfeeding. The LATCH score, developed by Jensen et al., is one of the earliest and most widely used tools. It evaluates five domains: Latch, Audible swallowing, Type of nipple, Comfort, and Hold (positioning), with scores ranging from 0 to 2 in each category. 18 The Bristol Breastfeeding Assessment Tool, a newer scale, focuses solely on infant behavior—positioning, attachment, sucking, and swallowing—and excludes maternal variables, thereby offering a more infant-centric approach. 19 Most studies have focused on the reliability of these tools, with fewer evaluating their role in guiding or evaluating counseling outcomes.
Lactation counseling, especially when delivered within the first 24–48 h postpartum, plays a transformative role in establishing effective breastfeeding. A Cochrane review found that structured breastfeeding support significantly increased exclusive breastfeeding rates at 4–6 weeks and up to 6 months postpartum. 20 Structured lactation support strengthens mothers’ confidence in breastfeeding and assists in correcting common feeding and attachment difficulties. 21
Despite these advantages, structured breastfeeding counseling is not uniformly implemented in most of the public and private sector facilities, especially in resource-limited, developing countries. This study was undertaken in response to these gaps, aiming to assess the impact of structured lactation counseling, conducted within 24 h of childbirth, on breastfeeding technique using a validated scoring system. By integrating clinical assessment tools with real-time counseling, this study aims to inform standardized protocols for early breastfeeding support and establish a basis for policy-level integration in neonatal care pathways.
Materials and Methods
Study Design and Setting
This was a quasi-experimental study, conducted at a tertiary care teaching hospital in North India. The study received approval from the institutional ethics committee. Informed consent was obtained from mothers before enrollment.
Participants
All women in their immediate postpartum period, who had delivered neonates at >34 weeks of gestation and initiated breastfeeding within 24 h of childbirth, were enrolled in this study, irrespective of the mode of delivery. Women with multiple gestation or whose neonates had major congenital anomalies, those requiring intensive care unit admission, or those receiving formula feeds prior to initial assessment were excluded.
Methodology
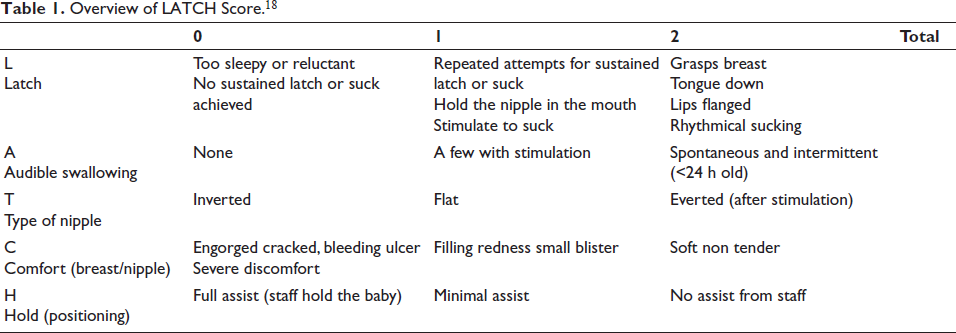
All women enrolled in this study had received counseling related to breastfeeding at least once during their antenatal period from the obstetrics team and at least once in the immediate pre-partum period from the pediatrics team. Breastfeeding support was also provided for the initiation of breastfeeding by the pediatric resident as well as the nursing staff attending the delivery, as a standard of care to all these mothers. The first breastfeeding assessment was done for all the enrolled mother–baby dyads, within 24 h of birth, at least 6 h after the initiation of breastfeeding, using the LATCH score. LATCH score evaluates five components—Latch, Audible swallowing, Type of nipple, Comfort, and Hold, each of the components being given a score of 0, 1, or 2 with a maximum total score out of 10, as shown in Table 1. LATCH score <8 indicates ineffective breastfeeding. 22
Overview of LATCH Score. 18
The first LATCH scoring was followed by a structured breastfeeding counseling, administered within the first 24 h of childbirth, by one of the investigators, adhering to the following key steps:
Initial assessment and building rapport: The mother was greeted warmly to create a supportive environment. Her knowledge, concerns, and previous experiences with breastfeeding were assessed. Education on the importance of breastfeeding: The benefits of breastfeeding, for the baby, as well as the mother, were explained in detail. Demonstration of proper latch and positioning: The signs of good positioning and attachment while breastfeeding were explained to the mother, using videos. Hands-on support: The mother was assisted in positioning the baby at the breast. The latch was observed, and real-time feedback was provided. Any issues with latch or positioning were identified and corrected. Guidance on feeding cues and frequency: The mother was taught to recognize early hunger cues (sucking fingers, lip smacking, rooting). Feeding on demand was encouraged, typically 8–12 times in 24 h for newborns. Information on maintaining milk supply: The mother was advised to do frequent breastfeeding, including nighttime feeding and skin-to-skin contact with the baby. She was also advised not to use pacifiers or bottle feeding. Addressing common challenges: Issues such as nipple pain, sore nipples, retracted nipples, or poor latch, if present, were addressed, and practical solutions were provided. Any fears, concerns, or misconceptions regarding breastfeeding put forth by the mothers were discussed and addressed. Encouragement and emotional support: The mother was praised for her efforts to effectively breastfeed her baby to reinforce her confidence. The family members were also counseled to support the mother and to encourage and assist her with breastfeeding.
Breastfeeding re-assessment was done, using the LATCH score, at 72 h after childbirth, or at discharge, whichever was earlier, to determine the effect of the structured breastfeeding counseling. Selection bias was minimized by enrolling consecutive deliveries and standardizing counseling. Measurement bias was minimized by using validated tools and training all assessors in uniform methodology. For analysis, LATCH scores were categorized as “ineffective” breastfeeding if the score was less than 8 out of 10.
Sample Size Calculation
The sample size was calculated based on the prevalence of ineffective breastfeeding (72%) reported by Rapheal et al. 22 Using the formula n = z2 × pq/d2, the sample size was determined to be 310, with a 95% confidence level and a 5% margin of error.
Statistical Analysis
Data were analyzed using IBM SPSS version 26. Descriptive statistics were used to summarize participant characteristics. The paired LATCH score differences were tested for normality using the Shapiro–Wilk test, and the data satisfied the assumption of normal distribution for the paired differences. Paired t-tests were used to compare pre- and post-counseling scores. A P value <.05 was considered statistically significant.
Results
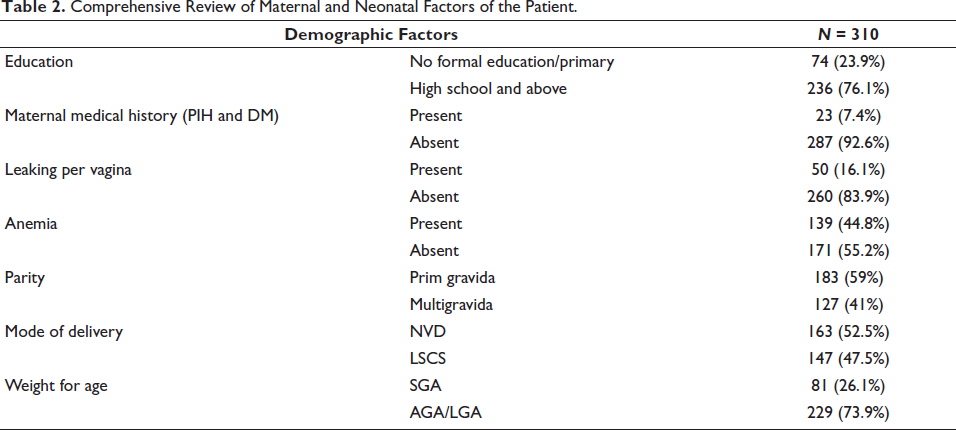
A total of 310 women in their immediate postpartum period were enrolled in this study. The age of the enrolled subjects varied between 19 and 34 years, with a mean age of 24 years. The birth weight of the enrolled 310 neonates varied between 2.01 and 3.67 kg, with a mean birth weight of 2.82 kg. The baseline characteristics of the enrolled subjects, including their educational status, maternal medical history, and parity, details regarding leaking per vagina and history of anemia, mode of delivery, and weight of the baby, are shown in Table 2.
Comprehensive Review of Maternal and Neonatal Factors of the Patient.
Breastfeeding assessment, performed using the LATCH score within the first 24 h after birth, revealed that only 3.9% of the mothers had a LATCH score greater than 8 out of 10. However, after the structured breastfeeding counseling, the proportion of women with LATCH score >8/10 increased to 97.1%. Structured breastfeeding counseling produced a very large improvement in breastfeeding technique, with a paired Cohen’s d effect size of 2.88, as shown in Table 3. A comparison of LATCH score within 24 h and after counseling, using paired t-test, revealed a statistically significant difference (P value of <.0001), as shown in Table 3.
Comparison between LATCH Scores Before and After Counseling.

An analysis of each component of the LATCH score before and after structured breastfeeding counseling was also done to gain better insight into the breastfeeding technique-related issues faced by the women in the immediate postpartum period.
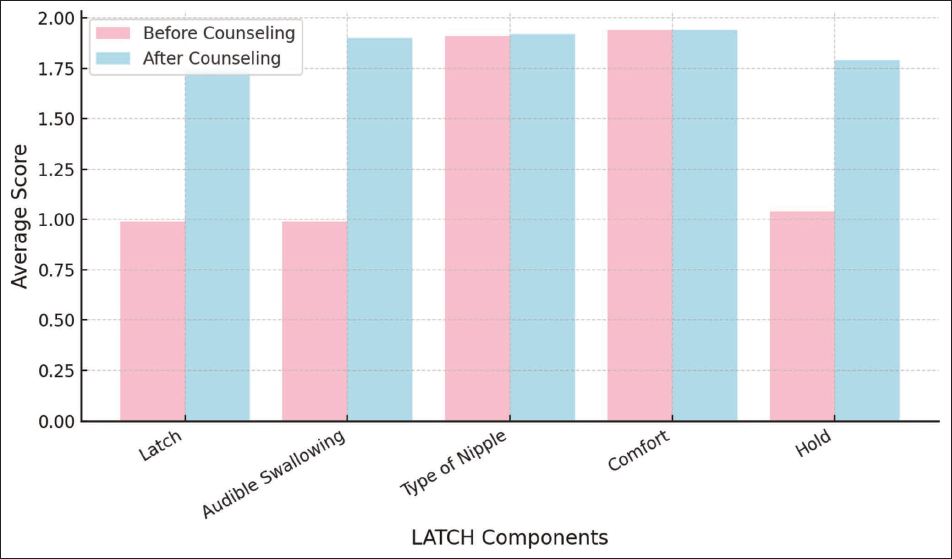
The components of “How well the baby latches onto the breast (L)” and “how much the baby swallows audibly (A)” were the most ineffective with an average score of 0.99 out of 2, before the structured breastfeeding counseling. The component of “How comfortable the mother is while feeding (C)” was the most effective with an average score of 1.94 out of 2. With counseling, there was a statistically significant improvement in latch (L), audible swallowing (A), and hold (H) components of the LATCH score, as shown in Figure 1.
Comparison of LATCH Component Scores Before and After Counseling.
Discussion
Principal Findings
This study demonstrated a marked improvement in breastfeeding techniques following structured breastfeeding counseling delivered within the first 24 h postpartum. The percentage of mothers with effective LATCH scores (≥8) rose from 3.9% pre-counseling to 97.1% post-counseling. These results underscore the substantial impact of early breastfeeding support and reinforce the value of standardized assessment tools in identifying and correcting ineffective feeding practices.
Interpretation in the Context of Existing Literature
Our findings are in agreement with those of Rapheal et al. and Boora et al., who also reported significant improvement in breastfeeding effectiveness following structured lactation counseling during the early postpartum period. However, the baseline proportion of mothers with effective breastfeeding in our study (3.9%) was considerably lower than that reported by Rapheal et al. (28%), possibly reflecting differences in maternal education, prior breastfeeding exposure, counseling practices, or population characteristics across study settings. Despite these differences in baseline scores, all three studies demonstrated marked post-counseling improvement in LATCH scores, highlighting the effectiveness of early structured breastfeeding support in correcting positioning and latching difficulties and improving breastfeeding outcomes.22, 23
The detailed component-wise analysis of the LATCH score in our study revealed that the most problematic domains pre-counseling were Latch and audible swallowing. Identifying the problem areas and stressing upon them during breastfeeding counseling is critical to successful breastfeeding and is closely linked with effective milk transfer, maternal comfort, and neonatal satisfaction. The significant post-counseling improvement in these domains demonstrates the responsiveness of these tools to intervention and validates the effectiveness of structured breastfeeding counseling in addressing technical barriers to effective breastfeeding.
Strengths
This study presents several strengths:
Structured intervention: The use of structured breastfeeding counseling as a low-cost, easily implementable intervention reflects the real-world feasibility of this intervention. Fairly large sample size: With 310 women being recruited in the immediate postpartum period, this study is adequately powered to detect statistically and clinically meaningful differences. Pre- and post-intervention assessment for all babies: This allows for clear attribution of observed changes to the counseling intervention, minimizing confounding factors. Focus on early postpartum period: The first 24 h are a golden window for breastfeeding initiation, and interventions during this time are crucial for long-term success of breastfeeding, one of the most promising interventions in improving neonatal and child health and decreasing mortality rates.
Additional Implications
In addition to demonstrating the effectiveness of structured breastfeeding counseling, our findings have significant clinical, educational, and public health implications:
Clinical practice: Incorporating structured breastfeeding assessments using validated tools like LATCH score and structured breastfeeding counseling into routine postnatal care can help identify at-risk mother–baby dyads before discharge, allowing for timely intervention. This is particularly important in settings with short hospital stays, where breastfeeding difficulties may otherwise go unnoticed. Training of healthcare workers: The study highlights the need for incorporating breastfeeding counseling and scoring tool training into medical, nursing, and midwifery curricula. Consistent use of breastfeeding assessment tools like LATCH score by trained professionals can standardize care and reduce inter-practitioner variability. Public health policy: The findings support calls to expand Baby-Friendly Hospital Initiative protocols across all delivery centers, with structured counseling and scoring tools forming essential components of lactation support. Digital health integration: The standardization provided by scoring tools opens the possibility of integrating breastfeeding assessments into electronic health records or digital apps, thereby allowing for real-time feedback and tracking over time.
Limitations
Despite its strengths, the study has limitations that merit discussion:
Single-center study: The research was conducted at a tertiary care teaching hospital in North India, which may limit the generalizability of findings to rural or lower-level facilities where resources and staffing may differ significantly. Short-term outcome focus: Assessments were limited to the first 72 h postpartum. While this period is critical for initiation, longer-term follow-up is essential to determine sustained impacts on breastfeeding exclusivity and duration. No maternal satisfaction or confidence metrics: The study did not measure maternal perceptions of breastfeeding or confidence levels, which are known predictors of breastfeeding continuation. Confounding factors: Apart from the change in the breastfeeding pattern due to the structured breastfeeding counseling, there could also have been some natural progression of maternal comfort and infant feeding over time. Incorporation of a control group, which did not receive the structured breastfeeding counseling, could help underscore the improvement in the breastfeeding technique, as a result of this intervention, and could help us better distinguish it from natural postpartum adaptation. Additionally, the same team of investigators was involved in both counseling and outcome assessment in the present study. This could have introduced observer bias.
Generalizability
Our findings are likely applicable to urban, hospital-based maternity units in similar low- and middle-income countries where structured lactation counseling is emerging but not yet universally implemented. The use of tools like the LATCH score can be adapted to different settings with appropriate training and language translation.
Implications for Future Research
Further multicentric studies are needed to explore the scalability and impact of structured breastfeeding counseling and assessment using the LATCH score across diverse healthcare environments. Future studies should include a controlled or randomized design to better distinguish the independent impact of structured breastfeeding counseling from normal postpartum progression, as well as structured maternal feedback using validated self-efficacy or satisfaction tools. Long-term follow-up could be done to explore its long-term impact on breastfeeding exclusivity and duration.
Conclusion
Breastfeeding is a vital public health priority, and counseling plays a pivotal role in overcoming the barriers to successful breastfeeding. This study highlights the effectiveness of structured counseling and the utility of the LATCH score as a reliable tool for breastfeeding assessment. By integrating these strategies into routine postnatal care, healthcare systems can ensure optimal breastfeeding practices, improving health outcomes for both mothers and infants.
Footnotes
Author’s Contribution
Conceptualization: Meenakshi Bothra; Data collection: Akshita; Statistical analysis: Aditi Mishra; Manuscript drafting: Meenakshi Bothra; Critical revision and final approval: Bindu T. Nair.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
The study received approval from the institutional ethics committee, Ref.No.SU/SMS&R/76-A/2023/78 on 28th April 2023. Informed consent was obtained from mothers before enrolment. Patient confidentiality was strictly maintained. Participation in the study did not affect the standard of care provided.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.