
Abstract
The aim of this contribution is to determine the communicative efficacy of selected print-based HIV and AIDS information education and communication (IEC) materials (posters, leaflets and brochures) among secondary school teenagers (13–19 years) in Harare. Data were collected over a period of 2 months from six schools, selected using multistage cluster sampling. It incorporated use of a self-administered questionnaire involving a sample of 750 teenagers, and 6 focus group discussions (FGDs), each comprised of 10 purposefully sampled participants. The survey investigated a number of indicators of communicative efficacy, wherein the IEC materials were found to be clear by 38.4 per cent (n = 288), informative by 45.2 per cent (n = 339), credible by 80.5 per cent (n = 604), appealing by 64.7 per cent (n = 485), important by 69.5 per cent (n = 521) and acceptable by 54 per cent (n = 405) of the respondents. The outcomes of the FGDs showed that, although HIV and AIDS IECs were generally believed to be appealing and to significantly increase awareness among teenagers, these were also considered somewhat unclear and inaccessible. Moreover, perceptions were strongly inclined towards use of Shona language, social media and elimination of fear appeals in HIV information. Thus, in addition to adopting young people-centred communication modes, finding an appropriate balance between complex language and efficacy of HIV prevention messages is imperative.
Introduction
The aim of this study is to assess the communicative efficacy of print-based HIV and AIDS information education and communication (IEC) materials that target young people in Zimbabwe, with a view to identify gaps and adequately address the information needs for this group. It focuses on selected posters, leaflets and brochures produced in English, whose aim is to ‘increase awareness, change attitudes and bring about a change in specific behaviours’ (Ministry of Health and Child Welfare (MoHCW) and Zimbabwe National AIDS Council (NAC), 2009, p. 5), in an effort to prevent and manage HIV and AIDS. The significance of HIV and AIDS information is emphasised by Melkote et al. (2014) who postulate that ‘lack of medical cure for AIDS puts the spotlight on prevention efforts’ (p. 85). According to Salam et al. (2016), IECs are an outcome of community field studies carried out to establish and address HIV and AIDS information needs, by communication and advocacy teams within HIV and AIDS organisations. As such, these focus on a specific environment, are peculiar to defined populations and are themed according to perceived information gaps. Echoing Mahapatra’s (2014) concept of IEC evaluation, in this study, the effectiveness of the selected materials would be determined through an assessment of the following communication indicators: clarity, informativeness, credibility, appeal (attractiveness), relevance, acceptability and accessibility. Mahapatra contends that:
The effectiveness of IEC materials largely depends on relevance, appeal, uniformity, simplicity of the content and language, accuracy of information, length of the material, cultural appropriateness, availability and modes of dissemination such as videos, brochures, posters, pamphlets, booklet, new flip book, and interpersonal communication. (Mahapatra, 2014, p. 3)
Given the long years of HIV and AIDS IEC interventions among young people and other groups worldwide, various studies in Africa and abroad have since been carried out to assess their efficacy. In this context, a survey was conducted in Southern Ethiopia (Bekele & Ahmed, 2008) to evaluate the effectiveness of four IEC interventions (pamphlets, interpersonal communication, educational videos and the combination of the three) in reducing HIV and AIDS-related stigma among high school adolescents. Data were entered into EPI Info software, exported to Statistical Package for Social Sciences (SPSS) and interpreted using descriptive statistics. Findings revealed that the four intervention strategies were effective in reducing HIV and AIDS-related stigma among adolescents. In Namibia, Shikongo (2010) explored the perceived impact of radio, television and print-based materials in communicating information on HIV and AIDS prevention to school going and out of school youths. Survey data were processed using SPSS software and interpreted in a descriptive manner. The study established that the respondents had adequate knowledge of HIV and AIDS prevention, indicating the efficacy of IEC.
Delate (2001) conducted a study which assessed youth interpretations of loveLife HIV and AIDS billboards in South Africa. Focus group discussions (FDGs) were conducted in four schools and analysed using the semiotic analysis approach. The findings indicated a limited understanding of loveLife images and language among the youth, which inhibited the comprehension of the billboard messages. Further, Michielsen (2012) assessed the effectiveness of peer-led school-based HIV prevention interventions for adolescents in Rwanda. A longitudinal non-randomised controlled trial study, including eight peer education interventions and six control schools was carried out. A survey was done and the findings indicated that the effectiveness of all eight peer education interventions are generally minimal for various sociocultural reasons. Similarly, findings from a survey conducted in India with a sample of students indicated that the theories and models that underlie HIV and AIDS IEC materials do not consider cultural aspects of the receiving audiences (Rawjee, 2002).
While the task of evaluating health communication campaigns in developing countries is complex (Sood et al., 2014), scholars in Zimbabwe have made strides in assessing HIV and AIDS IEC intervention efforts (see e.g., Chiwara, 2012; Mavunga & Kaguda, 2016; Mpofu, 2013; Mukenge & Chimbarange, 2012). However, up until now, there seem to be no studies that focus on the implementation of IEC among young people. This research gap is worrying given various research outcomes from other countries, indicating that HIV and AIDS IEC materials are potentially insufficiently comprehensive for this group. In Mahapatra’s view ‘In many instances, print-based IEC materials are too lengthy, often repetitive, extremely generic, boring, outdated and even inaccurate at some places’ (2014, p. 1). To this end, this study which evaluates the effectiveness of a sample of print-based HIV and AIDS IECs among teenagers in Zimbabwe is justifiable, as these are perceived to display more communication inadequacies. Thus, while this study strives to make a modest contribution towards the understudied area of IEC implementation, its results will also inform the future design of HIV and AIDS materials for young people, through identifying and proposing ways to resolve the existing communication gaps.
Background
Akin to other sub-Saharan African countries, HIV and AIDS in Zimbabwe is mostly driven by unprotected heterosexual intercourse (Van Dyk, 2000). The first AIDS case was reported in 1985 in Hurungwe, Zimbabwe (Mahomva et al., 2006) and the HIV epidemic peaked in 2001 with an adult prevalence rate of 33.7 per cent, registering the most severe epidemic of the century (UNAIDS, 2001). However, research indicates that since then, Zimbabwe has been experiencing a gradual decline in HIV prevalence in adults, recording approximately 14 per cent in 2017 and 13 per cent in 2016 (Zimbabwe National AIDS Council, 2017). Nevertheless, despite the significant decline of HIV infection rates, HIV prevalence in Zimbabwe remains very high, making it the sixth hardest hit nation worldwide (WHO, 2018).
Teenagers, who according to the United Nations (2010) incorporate young people aged between 13 and 19 years, represent one of the most HIV and AIDS vulnerable groups in Zimbabwe and other countries in sub-Saharan Africa (SSA) (Michielsen, 2012). According to Michielsen, 50 per cent of all new HIV infections worldwide occur in this group, and 80 per cent of these take place in the SSA region. Consequently, the young people in Zimbabwe happen to be the current sources of the budding new HIV epidemic in the country, as postulated by Dr Parirenyatwa the former minister of health and child care in a report on national HIV progress (Herald, 2017). He confirms that the youth represent a knowledge gap in HIV prevention and are the bearers of new HIV infections. Parirenyatwa underscores youth susceptibility when he notes that: ‘We discovered that there are four groups in this country where the HIV rate is still high. Those on the lead of the group are young people, both girls and boys, especially those in colleges and universities’ (Herald, 2017, p. 1). The haunting knowledge gap indicated in young people’s ignorance and the risky sexual behaviours are suggestive of the failure of the previous HIV and AIDS campaigns to sufficiently account for the youth. Alonge (2017) argues that the youth still engage in unprotected sex in most African societies, perhaps due to the one-way nature of mass media campaigns where interaction is barred.
Given the young people’s vulnerability, and that sexual behaviour is the main route of HIV infection, whose curable treatment is not known, changing high-risk sexual behaviour is fundamental in combating the spread of the pandemic (Michielsen, 2012). This study is thus interested in print HIV and AIDS IEC as a form of behaviour change communication. As Komunda (2007, p. 13) posits, in the absence of a known HIV cure, HIV and AIDS education is deemed a ‘social vaccine’, owing to its continuing role in providing information and knowledge that lead to behaviour change and eventual HIV prevention. Thus, while scientists at a global scale continue to grapple with the search for drugs for curing HIV, education remains one of the key pillars for preventing transmission of new HIV infections (Komunda, 2007; World Bank, 2002).
IEC and Its Implementation for HIV and AIDS Prevention in Zimbabwe
Information, Education and Communication is generally described as a process of working with individuals, communities and societies to develop communication strategies that promote positive behaviours, which are appropriate to their settings (UNESCO, 2007). Roger and Storey (1987) agree to IEC being a process. They define it as ‘a set of organised communication activities, designed and implemented to achieve specific objectives among an intended audience within a specific, limited period of time’ (Roger & Storey, 1987, p. 13). This is corroborated by WHO’s (2000), claim that IEC is a broad term comprising a range of approaches, activities and outputs. Given that IEC is a systematic process of communication, ‘he broad steps which need to be taken for the development of an effective IEC programme are as follows: planning; preparatory activities; material development, dissemination and utilization; monitoring and evaluation’ (WHO and NACO, 2006, p. 26).
Broadly, approaches to HIV and AIDS IEC include mass media to inform or establish positive norms among the general population, or the use of interpersonal communication to assist those at risk to assess their own behaviour and develop new personal skills (Arya et al., 2013; WHO, 2000). Khuat et al. (2004) identify sub-categories of HIV and AIDS IEC as print materials used to post information in the public, mass media, giveaway items, which are quickly disseminated and integrated into community life, community awareness events and innovative methods used to reach target groups. In their diversity, HIV and AIDS IECs seek to affect behaviour change or reinforce good behaviour in target audiences, regarding a specified problem within a defined period of time, as well as prevent diseases and promote health. In order to manage this, IEC draws from a number of theories such as diffusion theory, social marketing, behaviour analysis, anthropology and instructive design (Futa, 2008). In addition, these are community-based and tailor-made for specific groups perceived at risk. Hence, IECs are sensitive to cultural, religious, political and economic systems of target communities, enhancing accessibility and ethical soundness (Salam et al., 2016).
Thus far, IECs in Zimbabwe have succeeded in opening a discussion about HIV and AIDS, which was widely an avoided topic in the public sphere, especially in the early years of the pandemic. As Page (2002) rightly argues, there has been heavy silence surrounding the pandemic in the societies. Mashiri et al. (2002) highlight the problems of taboo in HIV and AIDS communication in Zimbabwe, associated with the sexual nature of the disease, and point out that speakers in interpersonal communication settings opt for silence or in some cases substituted offensive words with euphemistic expressions. Thus, through broadcast media, print media and performed local entertainment, vital information on awareness and prevention strategies has been disseminated up to date (John Snow Inc., 2011). Based on their multidimensional and multifaceted nature, it is argued that mass media IEC programmes play a vibrant role as the most effective means to disseminate HIV-related information to young people and other groups, in order to prevent HIV in Zimbabwe. As Khuat et al. (2004) posit, IEC in Africa ‘contributed to 70% of the population of reproductive age having basic knowledge on HIV and AIDS modes of transmission and prevention measures’ (p. 13). The purpose of this study is therefore to explore the communicative efficacy of selected HIV and AIDS IEC materials among high school teenagers in Zimbabwe, who present a knowledge gap that requires urgent remedying.
Materials and Methods
The Study
This study employs the survey method and FDGs to explore the attitudes and perceptions of teenagers regarding the efficacy of selected HIV and AIDS IECs that target young people in Zimbabwe. In order to carry out this study, two posters, two leaflets and two brochures that display HIV and AIDS information were presented to a sample of secondary school students and data were collected, processed and analysed systematically as outlined below.
Materials
A total of two posters, two leaflets and two brochures corresponding to three major campaigns, Voluntary Testing and Counselling, Voluntary Medical Male Circumcision and Sexual Reproductive Health Rights, were selected for this study and presented to a sample of teenagers. As noted by Patton (2001), purposeful sampling is useful as it is not only shaped by the interests and aims of the study but also allows the researcher to select only information-rich cases for study purposes. Poster 1, a PSI Zimbabwe production, promotes voluntary testing and counselling and employs the slogan Get Real Early. The poster is a colourful picture of a cheerful adolescent sports person in company of friends, who seems to be in control of his life as he has decided to get tested for HIV early, and is inviting fellow young people to act likewise. Poster 2 by PSI Zimbabwe similarly conveys an image of a young optimistic bride with a bright future as a result of the decision to get tested early and to preserve herself for marriage. See Appendix A for Posters 1 and 2.
Leaflet 1, produced by International Population Services (PSI) Zimbabwe, presents an image of a teenage boy who is happy after undergoing circumcision. The boy details how his future has been secured by getting circumcised, as this has reduced his chances of getting infected with HIV, and encourages other young boys to get circumcised as an HIV prevention measure. Leaflet 2 is another PSI Zimbabwe production which also promotes the uptake of male circumcision as an HIV prevention strategy, showing a team of courageous youth soccer players, allegorically presented as defenders against HIV by virtue of getting circumcised. The key slogan driving the campaign for circumcision is Defend yourself from HIV. Get Circumcised!. Persuasively, the young players detail the benefits of getting circumcised, who can get circumcised, how to live after circumcision and where to get circumcised. See Appendix B for Leaflets 1 and 2.
Brochure 1 by Southern African AIDS Information and Dissemination Service Organisations (SAfAIDS) is a booklet which presents the picture of a teenager receiving advice about sexual reproductive health issues from a parent. It describes what sexual reproductive health is and provides guidelines on who to talk to and what to talk about concerning this issue, which is described as critical for young people, but sensitive. Brochure 2 also produced by SAfAIDS is a guide for young people, detailing the importance of understanding sexual reproductive health rights. Its main purpose is to remind young people that they have sexual health rights, which may act as their defence from early HIV transmission. See Appendix C for Brochures 1 and 2.
Study Area and Population
The study was conducted from 2 February to the 5 April 2019, in six secondary schools around Harare, the capital city of Zimbabwe. The total number of students in all six schools was approximately 3,000, comprised of teenagers (13–19 years) and belonging to Form 1 up to Form 6 classes.
Sampling
The sample of students who participated in this study was drawn from six schools around Harare. A multistage cluster sampling method was used to establish the study sites (schools), from which the participants of the survey and the focus groups were selected. Cluster sampling, also known as one-stage, is a sampling technique where the total population is divided into externally homogeneous, but internally heterogeneous groups (clusters) of participants, included in the sample (Jackson, 2011). According to Jackson, in multistage cluster sampling, the sample is further reduced by selecting a random sample from the selected cluster. In this study, this involved dividing the population of schools in Harare into representative geographic clusters. A total of six clusters were identified, informed by the types of schools found in Harare: urban government, academy, college, mission, trust and private schools. Within these clusters, one school was randomly selected in order to develop a sample of the study sites where teenage students were accessed. The selection of different types of schools ensured an even distribution of personalities and social backgrounds among the subjects of the study. Thus, these geographically and socially diverse schools produced a heterogeneous sample, which is representative of the characteristics of the wider population of teenage students in Harare. Precisely, as Jackson (2011) rightly observes, cost reduction and increased levels of sampling efficiency in terms of effort and time are the evident strengths of cluster sampling.
A two-stage sampling technique was then employed to select the study subjects. The first sample was for the questionnaire survey respondents, while the second was for the FGD participants. In the first stage, stratified random sampling was employed. This is defined as ‘a probability sampling technique in which the defined target population is divided into groups’ (Kim & Haziza, 2014, p. 374). This technique strives to produce a heterogenous sample, consisting of members of various groups of the population. The total population of the students found in the six schools was divided into six different strata, corresponding to their form levels (Forms 1–6). In this case, sampling involved randomly selecting 25 per cent of pupils in each stratum, producing a total sample of 750 pupils from all schools. This sample was heterogeneous as it included not only both sexes, but also various ages of teenage students, different levels of education and a variety of social backgrounds. This diversity contributed to a fairly representative sample of students in the six schools.
The second stage involved purposeful sampling, where only information-rich subjects were chosen for the FDGs. As posited by Creswell (2014), ‘Focus groups can be used to collect shared understanding from several individuals as well as to get views from specific people’ (p. 384). The sample of focus group participants comprised of 60 Advanced level pupils (10 from each school). A sampling frame for inclusion or exclusion of the subjects was established. The main boundary imposed for selecting the participants for FGDS was that of considering only Advanced level students (Forms 5 and 6). These were selected given their higher level of maturity and understanding of HIV and sexual issues, which was necessary for a fruitful discussion. Further, eligibility for inclusion involved willingness to participate and being accessible within the research clusters during the time of data collection. In addition, personal attributes such as gender, religion or ethnicity were not considered in selecting the participants. Moreover, as suggested by Kim and Haziza (2014) and as per this study, a sampling frame based on a specific location would by design exclude all other locations within the wider population, significantly narrowing down the sample.
Data Collection Instruments
A self-administered questionnaire with closed-ended questions was prepared and used to collect data in schools. It employed closed-ended questions only, considering the fact that the sample of teenagers was likely to find it difficult and non-motivating to respond to open-ended questions. Section A solicited socio-demographic information (age, gender, religion, ethnicity and level of education) of the teenage respondents. Section B evaluated the respondents’ views regarding the communicative efficacy of selected HIV and AIDS IEC materials, and Section C investigated perceptions of the role of IEC materials in increasing HIV and AIDS awareness, correcting misconceptions and modifying behaviours and attitudes. Section D examined the respondents’ preferences of content, language, type of IEC and site.
As noted by Marshall and Rossman (2016), scales are one way of ensuring that questions in a survey are asked fairly and in a balanced manner, and are also valuable for determining the strength of attitude or perception, rather than a simply yes or no response. In this regard, a 5-point Likert scale, whose scoring key ranges from 1 to 5 points, was used to evaluate the respondents’ perceptions in Sections B and C of the questionnaire. 1 indicated strongly disagree, 2 disagree, 3 neutral, 4 agree and 5 strongly agree. The respondents were presented with these attitudinal statements and asked to score each, along the multiple-point scale. Section D employed an alternative-answer questioning technique, which provided a list of possible responses to select from, where each selected response had weight of a single score.
In order to collect field notes from FGDs, a discussion guide with a list of questions was prepared. These questions were semi-structured to address the study’s aim and were arranged from specific to general, all open-ended, to enable effective discussions. Since the subject of HIV and AIDS is intimidating and somehow sensitive, especially for teenagers, an elaborative introduction was included. The introduction contained information of the goals of the discussion, duration and expectations from both participants and the conductor. As Creswell (2014) puts it, when conducting FGDs, the researcher’s intent must be clear and neutrality should be maintained. Five questions were prepared and asked: (a) Do you think HIV and AIDS IEC materials are useful in raising your awareness to HIV and AIDS issues? (b) Do you find the HIV and AIDS messages clear? (c) Do you find HIV and AIDS messages appealing? (d) How accessible are HIV and AIDS materials to you? (e) What are your preferred modes of HIV and AIDS information?
Data Collection Procedure
The researcher visited the selected schools one at a time to conduct the surveys. These were carried out concurrently across all form levels for the duration of 1 h during lunch break. Data collection involved first exposing the subjects to the selected posters, leaflets and brochures (see Appendixes A–C), followed by a distribution of questionnaires which was coordinated and supervised by class teachers in the respective Forms. The questionnaires were distributed immediately after exposure, so as to assess the communicative efficacy of the IECs among the students.
In order to compliment the questionnaire, and to obtain views and in-depth information pertaining to the effectiveness of IEC materials, the FGDs were held as follow-up to the surveys. A total of six face-to-face FDGs were conducted separately over a period of 3 weeks, one in each of the selected school premises, to enable environmental familiarity to the respondents. The individual FGD comprised of 10 participants (five Form 5s and five Form 6s) and the researcher who played the facilitating role. As the study was not gender-specific, heterogenous focus groups comprising of both male and female students were used to allow for diversity of views (Stewart et al., 2007). In all instances, with the participants’ consent, the researcher audiotaped the discussions while taking detailed notes.
The FDGs were initiated with a brief introduction, followed by exposing the participants to the selected HIV and AIDS posters, leaflets and brochures, initiating discussions which lasted for approximately 45 min. These were moderated by the researcher who tape-recorded the sessions, while taking down notes. Krippendorf (2013) notes the importance of tape recording and transcribing verbatim in enhancing accuracy of data. The highlighted questions were posed in a sequential manner, and discussions were developed from the comments and responses made to these questions. Themes of discussions included general views about sources of HIV and AIDS information, clarity and appropriateness of the HIV and AIDS messages, and how these can be improved to suit the participants’ needs. This procedure was observed in all FGDs carried out in the six schools.
Data Processing and Analysis
Data analysis in this study was two-fold, given that there were two sets of data from the questionnaire and FGDs. Questionnaire data were subjected to a standard quantitative data analysis using the 20.0 version of SPSS software, with the assistance of a qualified statistician. Descriptive statistics were used to determine the frequency of different variables. The dependent variables included in the study were clarity, informativeness, credibility, appeal, relevance, acceptability, influence on HIV and AIDS awareness, misconceptions, behaviour, attitudes, gaps requiring improvement, language preferences, mode of delivery and preferred sites. The independent variables incorporated the socio-demographic profiles of the respondents and exposure to HIV and AIDS IEC materials. The results were displayed using tables and graphs, followed by qualitative interpretations.
As for FGDs, data were analysed using the ‘bottom-up’ approach. According to Creswell (2014), ‘This analysis initially consists of developing a general sense of the data, and then coding description and themes about the central phenomenon’ (p. 237). Within this scheme, the voice recordings collected during the FGDs were transcribed to generate textual data, which is more amenable for qualitative interpretations. Themes and patterns, emerging from the participants’ discussions, in which they revealed perceptions regarding the effectiveness of HIV and AIDS IEC materials, were identified. The identified themes were used as categories under which the FGDs data were presented. Only the most important quotes that were relevant to the study’s aim were cited. As Clark and Braun (2013) rightly observe, ‘thematic analysis can be a method that works both to reflect reality and to unpick or unravel the surface of reality’ (p. 81). From an interpretive paradigm, qualitative data were interpreted guided by expectations, communication theories and existing literature, signalling specific conclusions, followed by relevant recommendations.
Ethical Considerations
In order to observe research ethics, permission to carry out the study’s investigations and cooperation for data collection was sought from school authorities in writing. School pupils were briefed concerning the purpose of the study (which was strictly academic), its procedure, the significance of their participation and of providing accurate information. Informed verbal consent was sought from the participants prior to the data collection process in all instances. Moreover, the participants were informed of their right to withdraw from the study at any point they deemed necessary, without any consequences. The survey and FGD activities were also teenage friendly and culturally appropriate. Confidentiality and anonymity of the respondents and their responses were guaranteed. Thus, to protect the FGD participants’ identities, each was assigned an alphanumeric code based on the focus group number (G) and the number of participants (P) in each group. Since there were 6 groups and 10 participants in each, the participants’ codes ranged from G1, P1 to G6, P10.
Questionnaire Results
Socio-demographic Characteristics
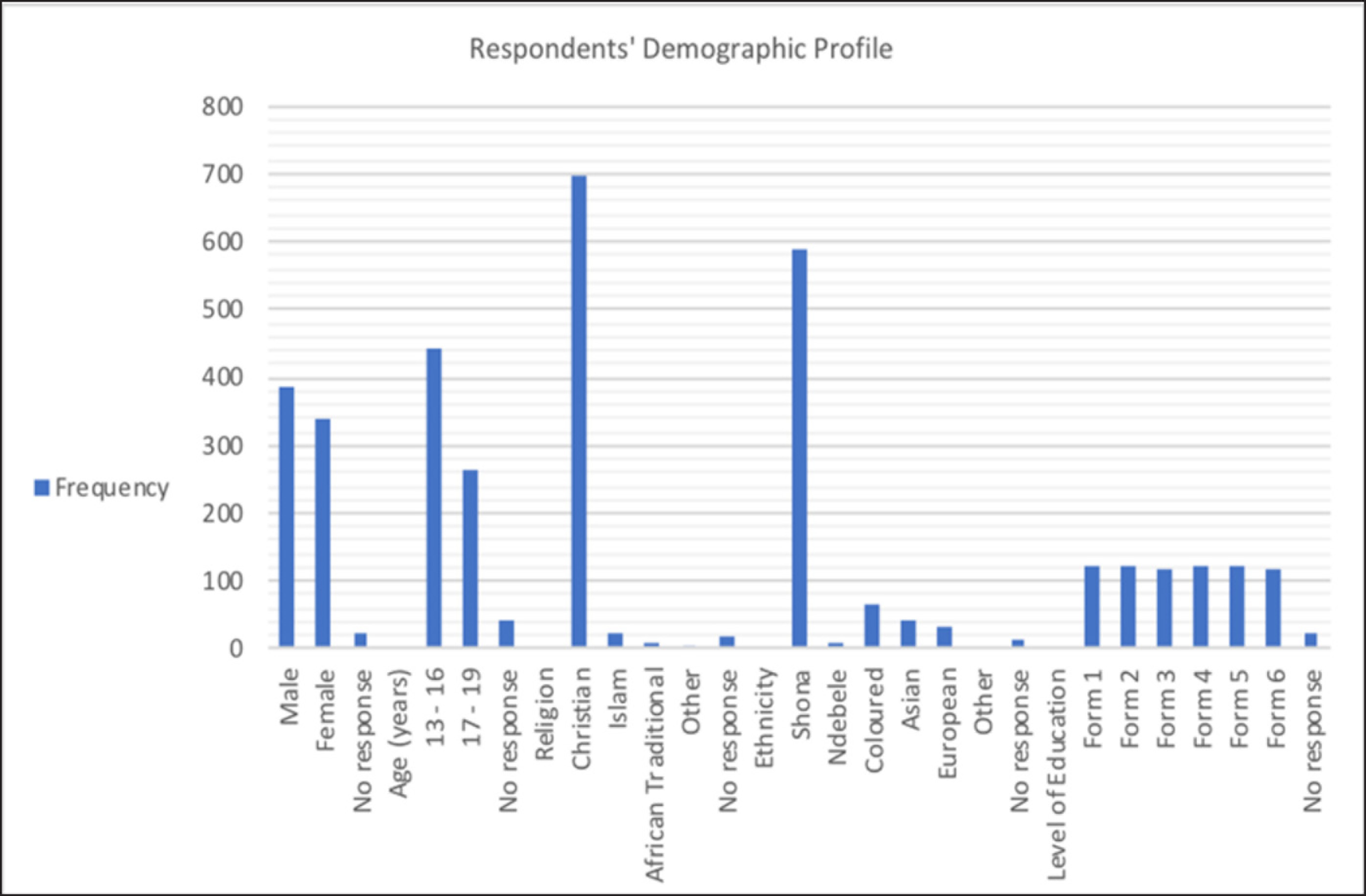
This section analyses the respondents’ demographic characteristics in the order in which they appear in Section A of the questionnaire. These are age, gender, religion, ethnicity and level of education, perceived to be associated with the communicative impact of HIV and AIDS IECs. As posited by Brown et al. (2003), the demographic profile describes the respondents’ personal and social attributes that have a bearing on the results of the research domain. Also, according to Khuat et al. (2004), IECs are developed in cognisance of the target audience’s demographic sociocultural aspects, which are key in measuring their appropriateness. Figure 1 provides a summary of the demographic information of 750 secondary school pupils who constitute the sample of the study. It indicates that the study subjects comprised of secondary school pupils, fairly distributed across six secondary school levels (Forms 1–6). The majority of the respondents were males (n = 388, 52%), Shona-speaking (n = 589, 78.5%), aged between 13 and 16 years (n = 443, 59.1%) and Christians (n = 699, 93.2%) (see Figure 1).
Perceived Communicative Efficacy of HIV/AIDS IEC Materials
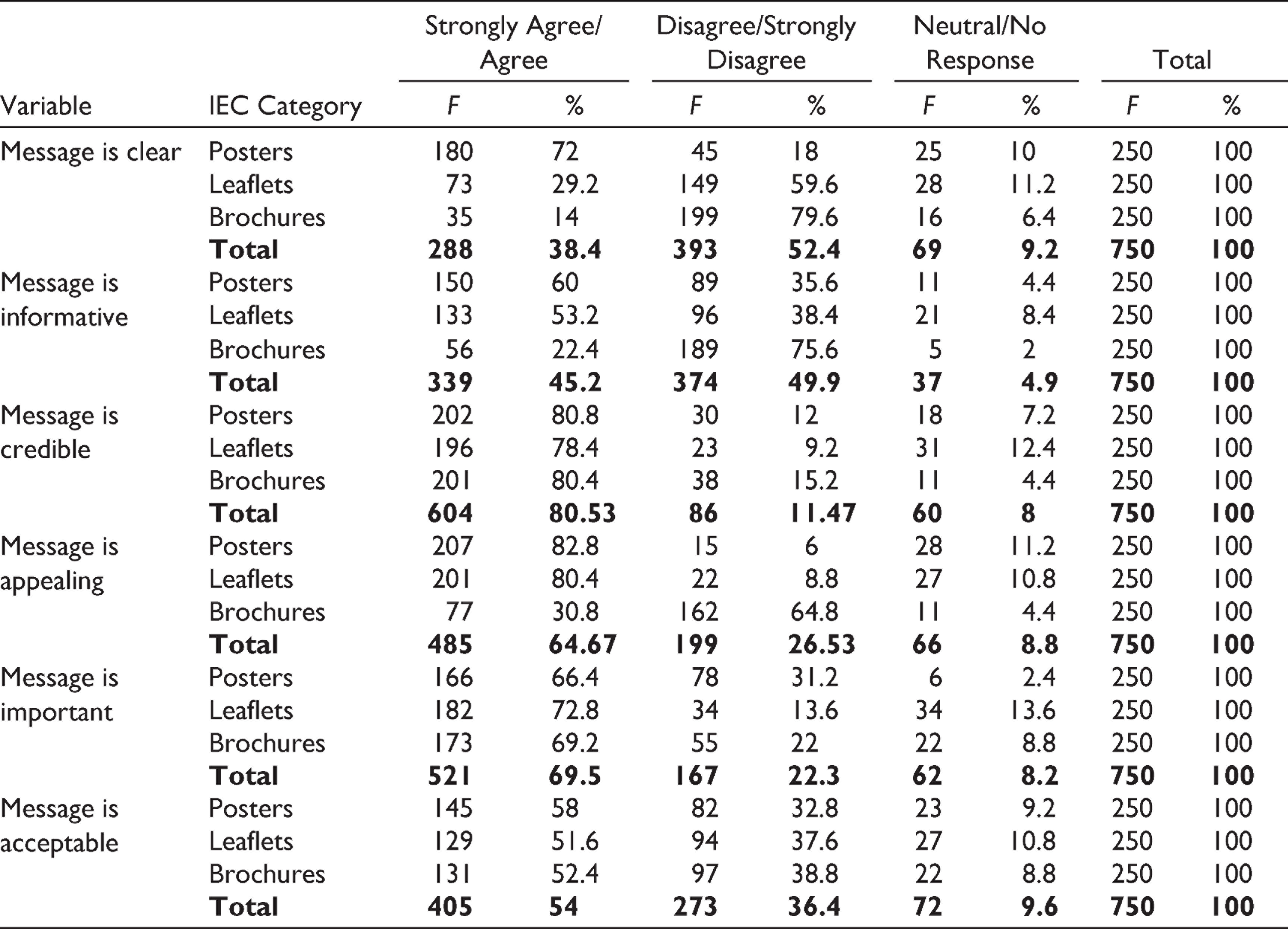
Section B of the questionnaire evaluates the respondents’ views regarding the communicative efficacy of the HIV and AIDS IEC materials. Communicative efficacy is determined by the following communication indicators: clarity, informativeness, credibility, appeal, relevance and acceptability. The summary of responses (see Table 1) indicates that, in terms of language clarity, posters were perceived to be the clearest type of IEC, followed by the leaflets and lastly brochures, which were considered unclear by 79.6 per cent of the respondents. The majority of the respondents believed that all three types of HIV and AIDS IECs were credible. Relative to clarity, most respondents perceived posters and leaflets to be more informative than brochures. Enquiry into message appeal also received a very positive response, particularly in the case of posters and leaflets, although most respondents (64.8%) found the brochures non-appealing. Approximately 70 per cent of all the respondents indicated that all three types of IECs were essential for their information needs. In view of message appropriacy, respondents yielded a positive response. Above 50 per cent of the respondents viewed HIV and AIDS IECs as acceptable. This was an optimistic outcome, given the influence of cultural and religious values on HIV information evaluation (Holtgrave et al., 1995).
Perceived Communicative Efficacy of HIV/AIDS IEC Materials
Perceived Significance of HIV/AIDS IEC Materials
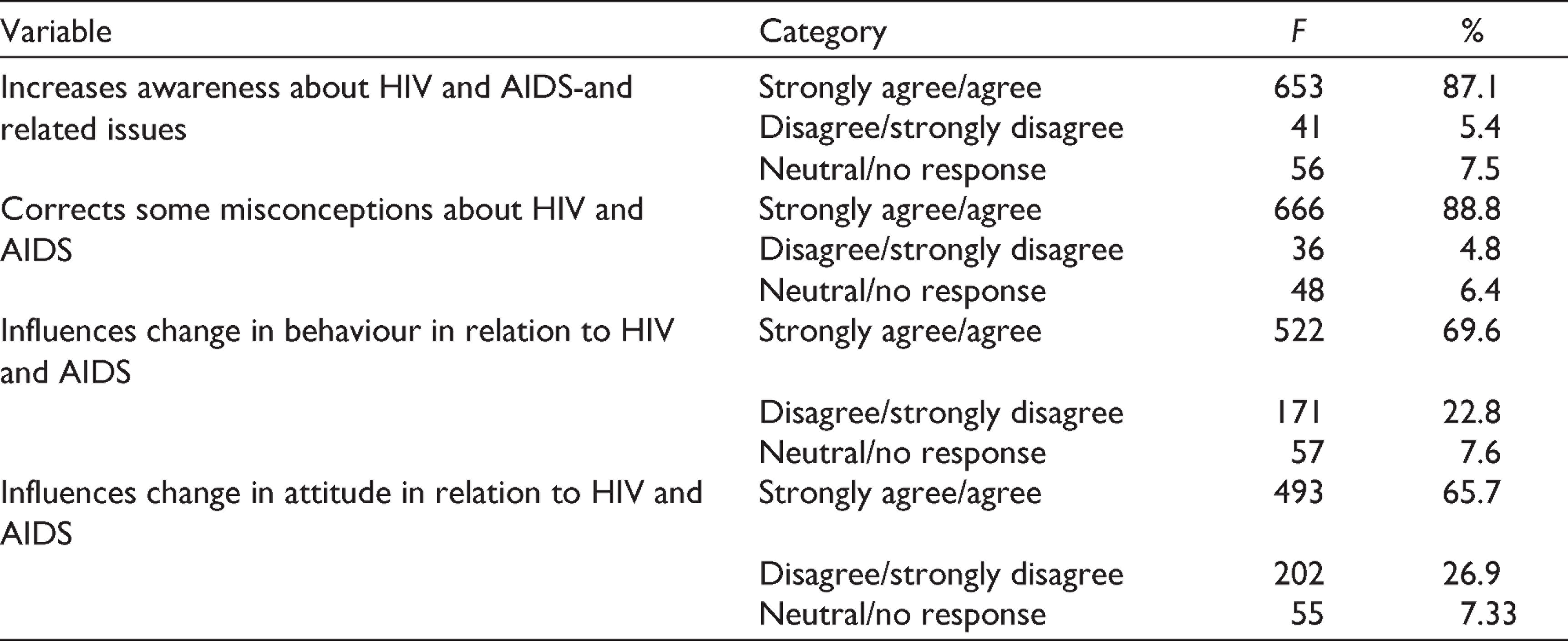
This section focuses on responses to the questions raised in Section C of the questionnaire, which investigate the role of IEC materials in increasing HIV and AIDS awareness, correcting misconceptions and modifying behaviours and attitudes. The evaluation of the significance of HIV and AIDS IECs to the teenage respondents yielded very positive results. IECs were largely believed to increase awareness, to rectify various misconceptions about HIV and AIDS and to impel behaviour and attitude change in relation to HIV and AIDS. See Table 2 for the summary of the results. These results are important as they enlighten on the significance of HIV and AIDS IECs to teenagers, as well as the relevance of these materials in HIV prevention. It concurs with Mahapatra’s (2014) view that, if IECs are planned, designed and administered well, they yield positive communication outcomes on intended audiences.
Perceived Value of the HIV/AIDS IEC Materials
Preferences of Content, Type and Site of HIV/AIDS IEC Materials
This section explores responses from section D of the questionnaire, which focused on the respondents’ preferences of content, language, type of IEC and site. Here respondents had the privilege to select more than one response as demonstrated in Table 3. An investigation into the respondents’ preferences of content, type and site of HIV and AIDS IECs revealed that the majority preferred materials that are produced in Shona language (81%), through social media mode (86%) and disseminated at home (55%). In addition, most of the respondents believed that, in terms of production, HIV and AIDS IECs require further improvement. In this regard, 37 per cent indicated that these materials need a total improvement, while 47 per cent believed that they require a partial improvement. Improvement was mostly pointed in the direction of message content (51%).
Preferences of Content, Type and Site of HIV/AIDS IECs


Results of Focus Group Discussions
Significance of HIV/AIDS IECs in Raising Awareness
The participants of FGDs unanimously responded positively to the question of whether or not HIV and AIDS IECs sufficiently raise audience awareness. These reported that IECs are sources of useful and new information in issues related to HIV and AIDS and sexual reproductive health. It was noted that: ‘nowadays we no longer have aunties to sit down and talk to us about these things, therefore, we strongly rely on these materials’ (G3, P2). However, some of the participants (G1, P9; G1, P10; G3, P3; G4, P7; G5, P3 and G5, P6) expressed concern that some of the messages are difficult to conceptualise, especially if the topic and the concept is new. When probed to elaborate, G4, P7 pointed out that, ‘sometimes the issues discussed are really hard to understand, especially when it’s your first time hearing about them’.
Clarity of HIV/AIDS IEC Materials
Most participants reported that the messages presented in HIV and AIDS materials were clear and comprehensive. They also noted that the language is generally exciting and suitable for their age groups. Commenting on the language, some noted that it is ‘exciting’ (G1, P5), ‘simple’ (G6, P6), ‘inspiring’ (G2, P8) and ‘catchy’ (G3, P9; G4, P4). However, in addition to misgivings about the complexity of some issues discussed in the materials, and indirect references to topics that are new and unknown to them, the participants held strong sentiments of lack of understanding, deriving from use of complex language. These displayed misconceptions and speculations concerning some technical and medical terms and concepts discussed in the materials. In G2, P10’s words: ‘I am not sure if I understand some of the statements in this brochure, it is too scientific for me’. There were several indications of similar concerns about brochures in all FGD sessions held.
Appeal of HIV/AIDS IEC Materials
Focus group discussions revealed that HIV and AIDS IECs are colourful and attractive for the teenage participants. The participants confirmed that they are drawn to reading and seek meaning by the appealing nature of the materials. There was also reference to use of effective images that accompany the messages and complement them. Most participants indicated that the images were not only useful in captivating their attention but also aided understanding and acted as demonstrators, especially for complex matters. Participant G4, P5 indicated that ‘I think that if the pictures were not there, I wouldn’t understand some of these messages, they are really helpful’. In terms of images that aid effective communication of sexual topics, most participants warned that the images should not be too explicit as this will cause public embarrassment.
Accessibility of HIV/AIDS IEC Materials
Th majority of the teenagers who participated in the focus groups noted that HIV and AIDS IECs are generally not accessible to them. When asked if they have ever seen any print HIV and AIDS IECs, G1, P7 revealed that: ‘We do not know where these are found (brochures and leaflets), we usually see some billboards and posters here and there, but not quite’. In agreement G4, P2 indicated that: ‘I only came across an HIV flyer once in a clinic, I find these very scarce’. Thus, relative to accessibility, most participants in this study indicated that they do not have access to HIV and AIDS IECs, and that they are only exposed to those displayed in public notices. Most of them also confirmed that they have no clue of where they can be procured for their reading.
Preferences of HIV/AIDS IEC Materials
The participants indicated the need to use social media for HIV and AIDS communication, as traditional mass media is getting outdated. These mentioned that social media are convenient and accessible to everyone, as these are platforms of communication for the youth. They revealed that social media were the best mode of communication as they permitted interaction and sharing of information with friends. Some noted that social media platforms are exciting and convenient to use. According to G5, P2, ‘Social media is the way to go’. In terms of language, some participants indicated that IEC materials should limit use of intimidating words and images, as the existing ones seem to cause fear and restlessness in young people, especially those that educate about Sexually Transmitted Infection (STIs). For instance, G2, P1 reported that: ‘these messages present some horrifying information and images about HIV and AIDS and illnesses. I sometimes wonder if all that is reality’. In essence, the participants suggested the need to use a simpler and less threatening language in HIV and AIDS IECs targeting young people, in order to enhance effective learning outcomes.
Discussion
Although the effectiveness of mass media IEC has been studied in Zimbabwe (see e.g., Chiwara, 2012; Mavunga & Kaguda, 2016; Mpofu, 2013; Mukenge & Chimbarange, 2012), there is hardly any research evaluating the efficacy of print HIV and AIDS IEC among teenagers. This study contributes to this existing knowledge gap, through an investigation of the communicative efficacy of selected posters, leaflets and brochures among secondary school teenagers. Through a survey and FDGs with a sample of students from schools around Harare, the study established some strengths and weaknesses of HIV and AIDS IEC targeting young people. The overall response was positive, suggesting that these are, to a large extent, effective in raising awareness and influencing behaviour change, necessary for curtailing the imminent spread of HIV in this population.
Clarity is a significant feature of health communication, and according to Khuat et al. (2004), successful IECs are essentially clear in communicating specific messages that are easily remembered. The extent to which young people’s HIV and AIDS IECs are clear is determined by use of simplified language, which is audible to this group. As indicated by the outcome of the study, posters which are less complex and less dense were found clearer than lengthy and detailed brochures, which discuss various biomedical issues in relation to HIV and AIDS. Thus, despite the fact that HIV and AIDS brochures and leaflets provide opportunity for detailed explanations and clarity, aided by images, these appear complex and incomprehensive for teenagers who find them unclear and difficult to understand. This is consistent with the results of Mahapatra’s (2014) study on IEC effectiveness, which concludes that: ‘Existing HIV/AIDS related IEC materials are often insufficiently comprehensive or inadequately designed to local needs and issues. In many instances, print-based IEC materials are too lengthy, often repetitive, extremely generic, boring, outdated and even inaccurate at some places’ (p. 3). This problem is attributable to poor translation of the materials from English (the language in which they are produced) into local languages, as well as the lack of collaboration between HIV and AIDS organisations and the governments, which has resulted in duplication of information and errors (Mahapatra, 2014).
Nevertheless, despite the view of lack of clarity in some types of print HIV and AIDS IECs, the teenagers found the messages informative. The IECs bring to the fore biological and scientific information associated with HIV and AIDS reality, management, treatment and care, which is not covered by the schools’ curricula. Based on their informativeness, IECs are conceivably one of the most indispensable tools for HIV and AIDS communication, in a context where education is deemed ‘social vaccine’ (Komunda, 2007). It is also interesting to note that the teenagers found the HIV and AIDS IECs credible sources of information, since credibility is associated to message acceptance and retention (Taffa, 1998). Taffa posits that, ideally, HIV and AIDS information should have an impact on the cognitive, affective and psychomotor domains of the receiver. In this context, Cherie et al. (2005) emphasise that: ‘This can be realised when the source is credible and the message is understandable, appropriate, timely, practically applicable, accessible and in line with the expectation and interest of the target audience’ (p. 75).
Akin to credibility, message appeal is a prerequisite for successful communication. The outcome that the teenagers in the study found the studied HIV and AIDS IECs captivating and exciting, based on attractive colours and images, is very positive. This guarantees prompt recognition of materials upon exposure, by this group. It is also very significant that the teenagers have a perceived need and high regard for HIV and AIDS IEC materials, which focus on their information needs. Thus far, IECs are deemed the most vibrant sources of accurate and detailed HIV and AIDS information in Zimbabwe (MoHCW and NAC, 2009). As aptly expressed by Mitchell et al. (2001), humans are information seekers; hence, it becomes imperative that the information offered is responsive to their needs. Also, perceptions are driven by relevance to personal interests, needs, wants, concerns and expectations (Khuat et al., 2004; Mitchell et al., 2001). Therefore, Mitchell et al. (2001) conclude that ‘the message should be of immediate, concrete and explicit relevance to the audience for it to be attended and internalized, which is lacking in the current mode of information delivery in the schools’ (p. 421). Moreover, as postulated by Pratheepa and Nithya (2014) ‘IEC become effective only when they are relevant, need based and used by the target audience’ (p. 53).
Given the delicate nature of HIV and AIDS issues in communities, in most cases, acceptance and tolerance of HIV messages are determined by cultural and religious norms of the society (Clarke, 1995; Holtgrave et al., 1995). Thus, according to Clarke (1995), ‘cultural competency’ in HIV and AIDS prevention messages has been regarded as a significant feature of successful intervention programmes. In this study, most of the teenagers acknowledge cultural and religious sensitivity of the HIV and AIDS IECs, which they find non-offensive and accommodative to people’s beliefs and norms. As such, emphasised in these messages are cultural aspects such as the socialising role of elders and avoidance of candid reference to sexual issues that dominate the discourse of these messages, and that are considered taboo in the Zimbabwean context. However, the study subjects expressed concern over the use of fear and intimidation tactics in these messages, especially those addressing STIs that lead to exposure to HIV. Although not necessarily harmful, these seem to alienate the young people who may choose to distance themselves from such kind of communication. Research has since revealed that fear-arousing messages do not promote behavioural change; instead, they produce adverse effects (Sherr, 1990). Thus, there is an urgent need to address this problem, so as to enhance the communicative efficacy of HIV and AIDS IECs targeting young people.
In comparison to other forms of HIV and AIDS IECs, the teenage respondents in the study indicated a very low exposure to print materials, particularly leaflets and brochures, and hence poor knowledge of issues addressed in these materials. This is mostly due to poor distribution of the print IECs, coupled with demotivation to read bulky information. Unlike face-to-face discussions that provide instant exposure and opportunity to ask questions and seek clarification, print HIV and AIDS IEC seem to alienate the young audiences. Thus, there seems to be a wide gap between the perceived lack of access of HIV and AIDS IECs by young people, and the actual access of these materials. Narrowing this gap by ensuring the procurement and uptake of information leading to knowledge gain has supreme importance in reducing the HIV and AIDS burden in young people.
Moreover, considering the fact that effectiveness of communication is partly determined by language use, it is important to address the language issue in HIV and AIDS IECs. Mpofu (2013) and Okaron (2015) point out that, to achieve effective communication, language needs to be clear and unambiguous through use of linguistic and sociocultural repertoire that are familiar to recipients. According to Okaron (2015), ‘… the language used in HIV and AIDS advertisements achieves its role of communicative purpose when the intended audience receives the advertiser’s point with the same meaning that the author of the advertisement had when the advertisement was crafted’ (p. 41). Whereas language is fundamental in communication for HIV and AIDS awareness, it is worrisome that, despite the majority of the respondents’ preference of Shona IECs, those produced in English are dominant.
According to Mpofu’s (2013) study of HIV and AIDS awareness advertising at ZBC/TV, about 65 per cent of these advertisements are in English, and the rest in indigenous languages. Mpofu elaborates that HIV and AIDS information found in indigenous languages (Shona and Ndebele) constitutes mere translations from English and is limited. The existing disproportions are partly an outcome of the fact that HIV and AIDS information is conceptualised and implemented in English, which is the main official language. Kadenge and Nkomo (2011) explain that, owing to the central role of English as the main official language in Zimbabwe, various technical texts that have to do with development are produced in English and later translated into indigenous languages. Thus, in cognisance of this reality, there is need to assign a bigger role to indigenous languages in the production of IECs to enhance their communicative value.
Further, although print media seem to present a credible source of information and play a supportive role by providing durable reference information, these are least preferred forms of communication by teenagers. This may be attributable to the low literacy levels of young people, lack of a reading culture or the virtue of failure by the print materials to accommodate diversity of youth preferences. In this regard, the teenagers in the study prefer to use social media. Social media are emerging as young people’s most preferred sources of information about HIV and AIDS due to factors such as convenience and other benefits associated with their use. Although mass media communications have for a long time been a vital source for creating awareness, social media through interactive platforms are gradually rising to the challenge.
Social media and digital technologies have a great potential for delivery and reception of timely and substantial HIV and AIDS information, at a level that traditional mass media platforms have never attained. Given that there is generally a growth in mobile phone ownership and Internet access in the developing world (Alonge, 2017), and that the world is fast becoming one global village united by communication technologies (Robertson, 2014), the use of social media for HIV and AIDS communication in Zimbabwe would be strategic. Their potential is also discernible in their interactive nature, allowing users to exchange information in a two-way approach. Whereas mass media HIV and AIDS communications mainly rely on one-way channels of message transfer, social media give room for feedback and redirection of information. In fact, social media platforms would provide more visual interactive opportunities that are exciting and motivating for young people.
Umoru (2015) summarises the significance of interactivity of social media in HIV and AIDS communication when he states that the social networking sites have the ability to create ‘an interactive environment where discussions, ideas, feedbacks, instructional strategies, opportunities, practices and new directions can be established’ (p. 3971). As the Media Richness Theory (Daft & Lengel, 1986) postulates, the success of communication depends on the capacity of the medium to engage parties that are interacting. Further, given that ‘HIV education is vaccine’ (Komunda, 2007; Vandemoortele & Delamonica, 2002), interactive platforms are useful in the instructive role and in coaching behavioural change, especially in the case of high-risk groups such as the young people. Here, the users are enabled a chance to learn and address questions based on individual HIV-related experiences, as well as achieve self-advocacy. Accordingly, Robertson (2014) submits that since social media are interactive platforms, they are appropriate for consumption of HIV and AIDS related content amongst the youth.
Conclusions and Recommendations
Although previous research has shown a positive communicative impact of HIV and AIDS IECs, this study reveals that some print HIV and AIDS IECs (leaflets and brochures) present certain communication flaws that require remedying. Despite the fact that they are generally credible and appealing, somehow these lack clarity, making it quite challenging for young people to understand and learn from these messages. In addition to this hurdle, there is the dilemma of inaccessibility of these materials to this population, owing to poor distribution and perhaps poor reading culture among other factors. Young people also find the IECs intimidating as they employ fear-arousing communication tactics, resulting in further alienation. Moreover, HIV and AIDS IECs rely on traditional mass media platforms, which are ineffective for teenagers, who belong to the interactive Generation Z, who heavily rely on social media and its technologies. However, on a positive note, young people’s print HIV and AIDS IECs were found to be relevant and culturally competent, considering that their designs are accommodative to the religious and cultural views of the majority.
Given that print HIV and AIDS IECs, particularly brochures and leaflets, are incomprehensive and limiting for young people, deriving from the complexity of language and topics discussed, it is extremely important to address this problem. It is reasonable to conclude that HIV and AIDS brochures and leaflets would be more appropriate for adult audiences, who are able to explore complex topics. Hence, there is need for simplicity of concepts and language, if print materials are to have a desired communication outcome on young people. This concurs with Mahapatra’s (2014) suggestion that: ‘Availability of nonprint materials or materials in simple language with more graphics for communities with low literacy levels might be useful in raising HIV/AIDS awareness’ (p. 3).
Alternatively, HIV and AIDS IECs may be integrated with other existing prevention programmes so as to compensate for their communicative shortcomings. As asserted by Futterer (2007), despite their significant role in promoting awareness, IEC approaches do have strong limitations. In order to influence behaviour, there should be sufficient audience exposure, and IECs have to be combined with participatory methods, which encourage active community involvement (Futterer, 2007). Thus, instead of focusing on IECs only, to enhance communicative efficacy and to achieve communicative objectives, teenagers need to be exposed to other ongoing programmes which will heighten information sharing and, hence, HIV and AIDS knowledge and awareness. In addition, emulating Mahapatra (2014), in order to enhance the visibility of HIV and AIDS IECs, which seem to be inaccessible to young people, ‘Smaller organizations with limited funds might help in raising awareness by disseminating mutually reinforcing messages through establishment of a centralized resource centre like organizing the drama, theatre and puppetry in the communities’ (p. 3).
It is also important to consider adopting use of social media platforms in communicating HIV and AIDS messages to young people, gradually moving away from traditional mass media. These, as already highlighted, bring about interactivity, experience sharing, feedbacks, convenience, cost-effectiveness, exciting visual learning opportunities, appropriate for the interactive generation of young people, who happen to be the largest users of social media. Diwakar (2016) adds that ‘… the new social media opens up the possibility for the young (13-17 years olds), of being part of the global world’ (p. 161). In addition to social media, other interactive IEC approaches may be employed such as peer educators and FDGs. As the survey results indicate, although print IECs are effective in raising awareness of HIV and AIDS-related issues, and influencing positive behaviour and attitude change, some of them are user unfriendly for young people. In Mahapatra’s (2014) profound view, ‘dissemination of HIV/AIDS related information through internet might be a good option for young people as it offers confidentiality’ (p. 3). He elaborates that; ‘Increasing access to such materials through an organized distribution network and proper utilization of mass media are vital steps in improving overall HIV-related knowledge of a community which in turn will help to build a more positive social environment’ (Mahapatra, 2014, p. 3).
World Health Organization (WHO) and National AIDS Control Organisation (NACO) (2006) summarise the nature of effective IEC materials as: ‘…developed following a systematic assessment of the target audiences and with their participation’ (p. 26). As such, Khuat et al. (2004) make a sound suggestion of the need to conduct a needs assessment before starting an IEC campaign, in order to discover the target audience and the kinds of materials people would respond to. In corroboration, Mahapatra (2014) emphasises that ‘there is a strong need for monitoring and evaluation of IEC materials at regular intervals to incorporate the necessary changes as evident from ongoing research over time’ (p. 4). In view of this, young people should be involved in the design, implementation and evaluation of HIV and AIDS IEC interventions, to enable incorporating their feelings, views, experiences, expectations, concerns and needs in all these stages. This will also promote the designing and implementation of young people-oriented HIV and AIDS IECs, which are effective in achieving their communicative goals.
Limitations
The key limitation of this study has to do with its focus. Owing to the limited space available for this research, the study was restricted to teenagers in urban Harare secondary schools. Thus, it excluded other categories of young people such as those who are out of school, or who fall outside the geographic setting of the study (i.e., in the rural areas) and the non-teenage youths and adolescents, who are also the target of the studied HIV and AIDS materials. As such, the results of this study may not be generalised to the wider population of young people in Harare. This points to the need for conducting another research, which will shed light on the experiences and perceptions of other groups of young people, in relation to HIV and AIDS communication efficacy. Bridging this research gap will go a long way in presenting a balanced view of reality.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.