
Abstract
Background:
Takayasu’s arteritis (TA) is a rare medical disorder of probable immune aetiology which complicates pregnancy. It affects younger women predominantly and may have a significant impact on maternal and foetal health.
Aim:
To study the maternal and perinatal outcomes among pregnant women with TA, attending a dedicated obstetric hospital in South India.
Method:
It is a retrospective observational study done at Fernandez Hospital, Hyderabad, with 10,000 births per annum. All women with TA-complicating pregnancies who were birthed from 2005 to 2022 were included. American College of Rheumatology criteria were used for the diagnosis of TA. The primary outcome of interest was to analyse the type of TA, maternal and foetal outcomes in pregnant women with TA. The secondary outcome of interest was to compare foetal outcomes between pregnancies managed at Fernandez Hospital (group A) versus previous pregnancies managed elsewhere (group B).
Results:
During the study period, there were 119,053 births of which 38 women had TA, with a total of 92 pregnancies, of which 59 pregnancies were in group A and 33 pregnancies in group B. Type 4 was the commonest seen in 44% of women. Hypertensive disorders of pregnancy were seen in 67.7% of women. The live birth rate was 84%, miscarriages were 10% and 5% of women had stillbirths. Caesarean section rate was 59.3%. There was one maternal mortality.
Conclusions:
TA should be considered in young women with secondary hypertension. Maternal and foetal outcomes are good with appropriate diagnosis, treatment and management of complications.
Introduction
Takayasu’s arteritis (TA) is a chronic systemic vasculitis that affects the aorta and its major branches. 1 It is a rare disease with a male:female ratio of 1:9. Most of the women are of childbearing age. 2 The disease was first described by Mikito Takayasu, a Japanese ophthalmologist. The inflammation of major vessels leads to stenosis, occlusion and aneurysm formation and the resultant ischemia can result in maternal complications. Vasoconstriction affects placental trophoblastic invasion, leading to chronic placental insufficiency resulting in superimposed preeclampsia and foetal growth restriction. The course of the TA per-se is not affected by pregnancy.The main modality of treatment involves immune modulators (steroids, azathioprine, methotrexate, mycophenolate mofetil or cyclophosphamide) and control of hypertension.
Indian data in pregnancy outcomes is based on small studies, and the reports are conflicting about maternal and foetal outcomes in different studies. Of 16 women with TA, 50% had surgical intervention before conception and all received medical therapy and one-third had foetal growth restriction and a quarter were born preterm. Suppression of the inflammatory process of TA and its effect on placental inflammation in pregnancy with immunomodulators has been found to improve outcomes. 3
Pregnancy management remains a major challenge to rheumatologists and obstetricians as there is a lack of robust guidelines. This study is aimed to analyse the maternal and perinatal outcomes among pregnant women with TA.
Material and Methods
A retrospective observational study was done at Fernandez Hospital, Hyderabad, a tertiary care referral perinatal centre in India, with 10,000 births per annum from 2005 to 2022. This study was approved by the institutional review board and ethics committee with EC reference number 48_2022. All women with TA-complicating pregnancies who birthed from 2005 to 2022 were included. American College of Rheumatology criteria were used for the diagnosis of TA. Since TA is a rare disease, all women with TA, delivered and followed up at the study site during the study period were included. Women who were lost for follow-up were excluded.
Data was extracted from the medical records. Maternal characteristics studied were parity, type of TA disease based on the angiographic report (ref 3) (types 1–5), complications such as hypertension, aortic valve regurgitation, ocular and renal artery involvement and aortic artery aneurysm. Details about treatment such as disease-modifying drugs, antihypertensive medications and surgical interventions before pregnancy were noted. Obstetric data such as miscarriage, type of labour, mode of birth and indication for caesarean section were collected. Neonatal outcomes studied included gestational age, birth weight, perinatal mortality rate and neonatal intensive care unit (NICU) admissions.
Pregnancies were divided into group A and group B based on place of care. Group A were pregnancies managed at study centre with complete availability of maternal and foetal data, group B were pregnancies managed elsewhere where maternal data was lacking, and foetal outcome data was elicited from patient history.
The primary outcome of interest was to analyse the type of TA, maternal and foetal outcomes in pregnant women with TA. The secondary outcome of interest was to compare foetal outcomes between pregnancies managed at Fernandez Hospital (group A) versus previous pregnancies managed elsewhere (group B). Descriptive data analysis was carried out by frequency and proportion for categorical variables. Statistical analysis was carried out using Microsoft Excel.
Definition of Variables
Chronic hypertension: Blood pressure >140/90 mm Hg that predates conception or present before 20 weeks gestation and persists >12 weeks postpartum. 4
Gestational hypertension: Hypertension arising de novo at >20 weeks’ gestation in the absence of proteinuria or other findings suggestive of preeclampsia. 4
Pre-eclampsia: Pre-eclampsia is gestational hypertension accompanied by one of the following new onset conditions after 20 weeks’ gestation like (a) proteinuria, (b) maternal end-organ dysfunction (creatinine 1 mg/dL, elevated transaminases AST or ALT > 40 IU/L, neurological complications or pulmonary oedema) and (c) uteroplacental dysfunction. 4
Preeclampsia superimposed on chronic hypertension: Among women with chronic hypertension, development of new proteinuria, another maternal organ dysfunction or evidence of uteroplacental dysfunction. 4
Spontaneous miscarriage: Miscarriage is defined as the spontaneous loss of pregnancy before the foetus reaches viability. 5
Termination of pregnancy: Termination of pregnancy for medical indications with the consent of the patient and joint decision of the family and the obstetrician.
Foetal growth restriction: Foetal weight less than 10th centile for that gestational age. 6
Stillbirth: Baby born after 28 weeks without any signs of life. 7
Results
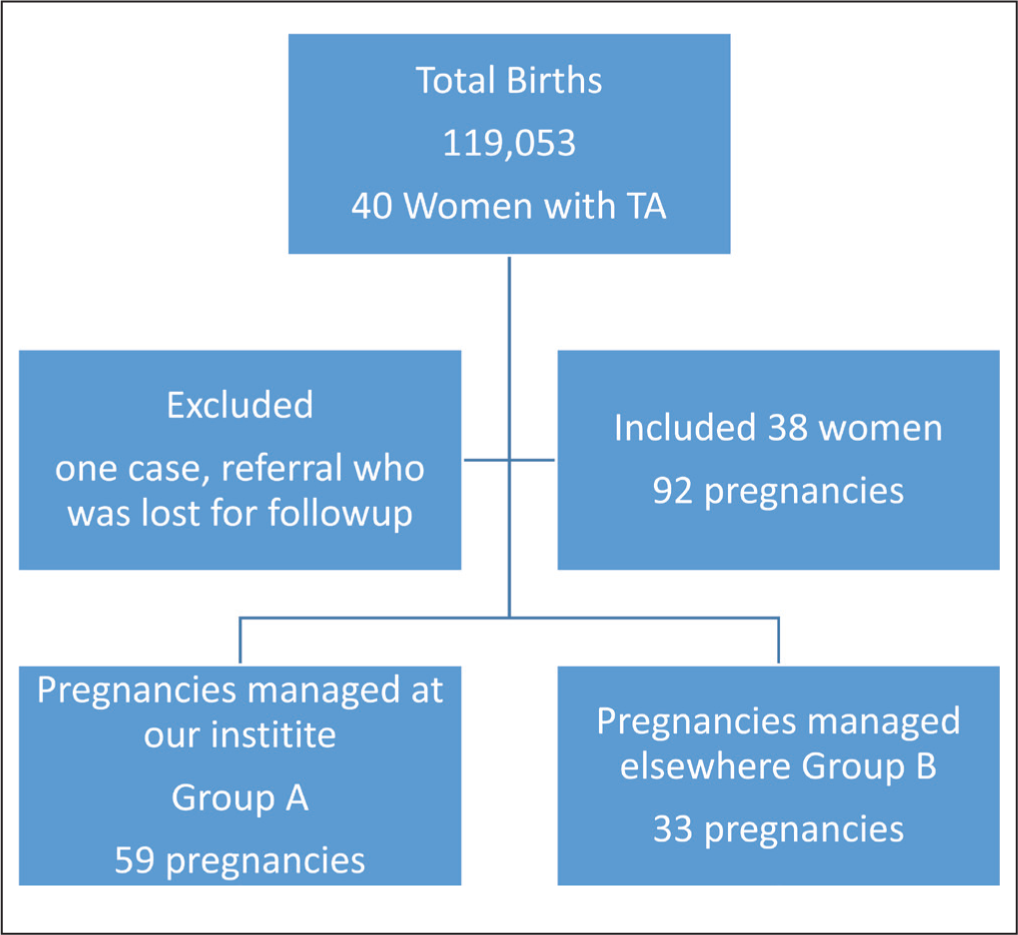
During the study period, there were 119,053 births of which 40 women had TA. The angiographic type was not available in one case as she came in an emergency and birthed immediately. Later, she was lost for follow-up hence excluded from the study.
A total of 38 women diagnosed case of TA with 92 pregnancies were included, of which 59 pregnancies were in group A and 33 pregnancies in group B (Table 1).
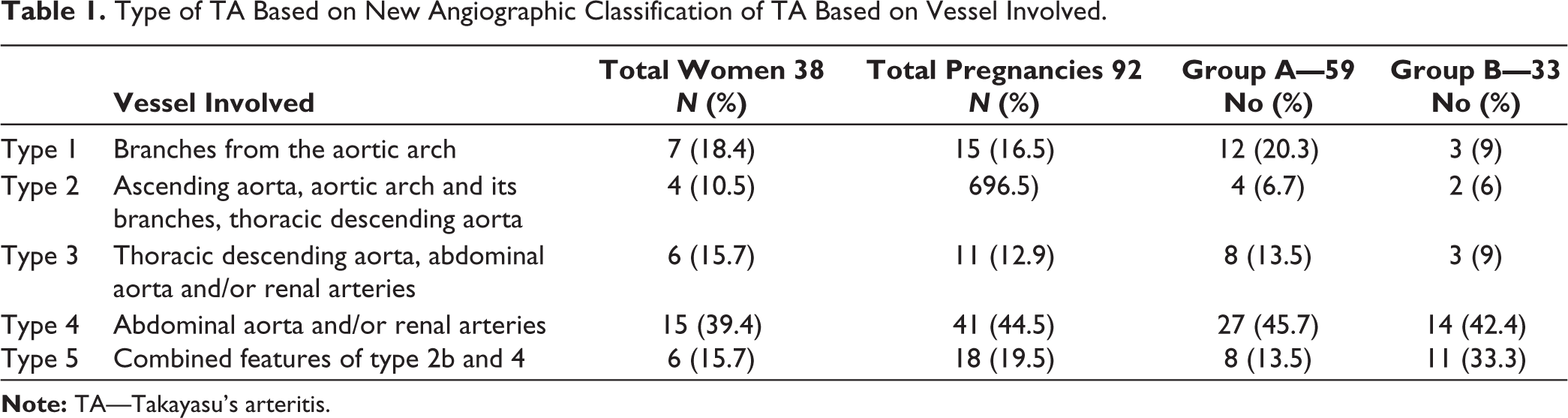
Type of TA Based on New Angiographic Classification of TA Based on Vessel Involved.
Primary outcome of interest was to analyse the type of TA, maternal and foetal outcomes in group A with 59 pregnancies.
Maternal outcome: Type 4 TA was the most common type (44%) followed by type 5 in 19%. Table 1 shows the number of cases in each type of TA.
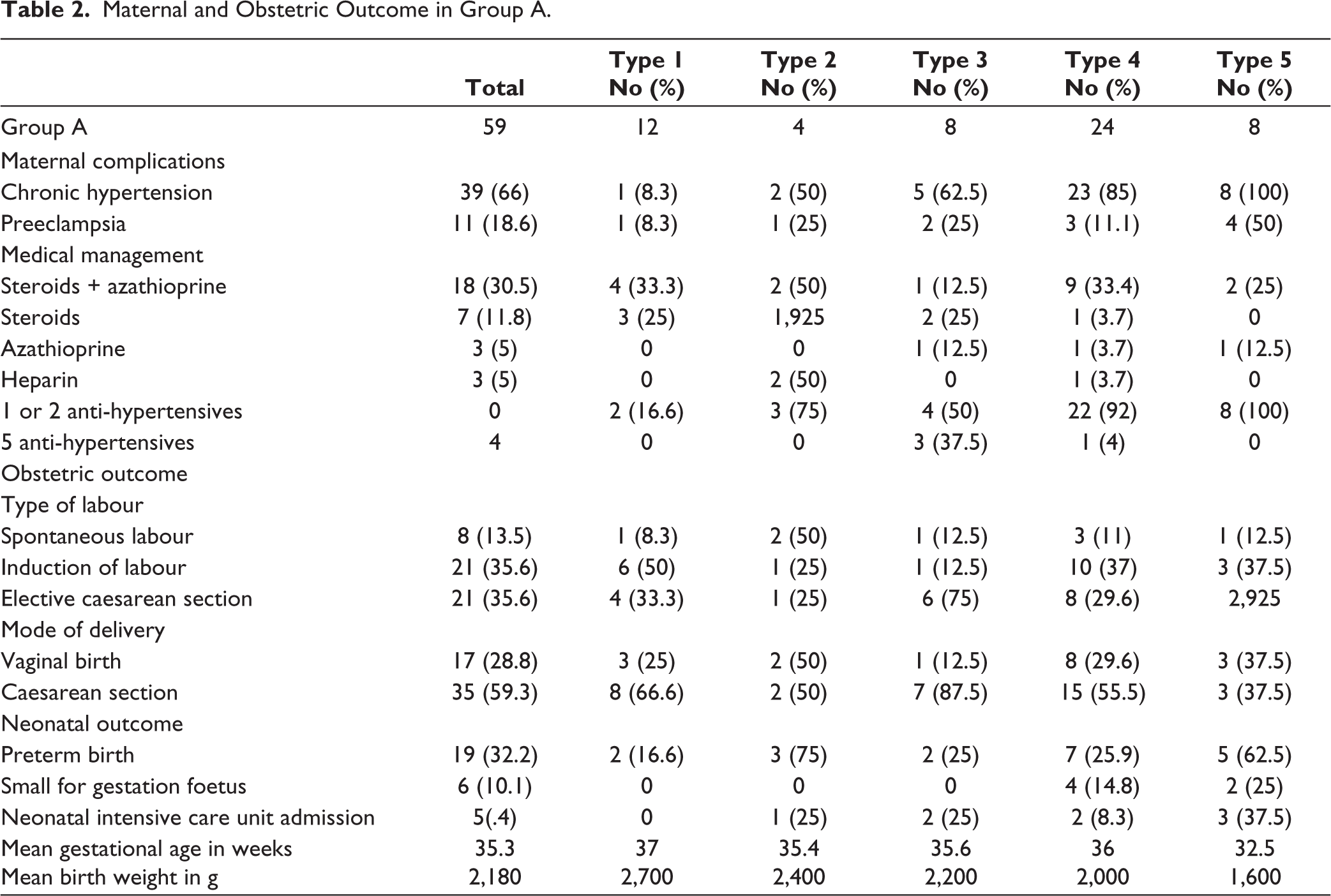
The majority (84.2%) of TA were diagnosed before pregnancy. Six (15.7%) were diagnosed during pregnancy. Hypertension complicating pregnancy was observed in 40 (67.7%) cases. Chronic hypertension was seen in 39 (66%) pregnancies of which 9 had superimposed preeclampsia. Gestational hypertension was seen in one pregnancy (type 4) and eclampsia (type 1 TA) in one pregnancy (Table 2).
Maternal and Obstetric Outcome in Group A.
Cardiovascular complications present were coarctation of the aorta (1, 2.6%), thoracic aorta aneurysm (1, 2.6%), internal iliac artery aneurysm (1, 2.6%), rheumatic heart disease in 4 (10.5%) and abdominal aorta flap dissection in one (1, 2.6%) woman.
Medications used included immune modulators such as steroids with azathioprine in 18 (30.5%) and steroids alone in 11% of women (Table 2).
In 90% of pregnancies, blood pressure could be controlled with a single drug or two anti-hypertensives (a combination of methyldopa, nifedipine and labetalol). Three pregnancies (37.5%) in type 3 and one (4%) in type 4 TA had refractory blood pressure and needed a combination of Nifedipine, Labetalol, Clonidine, Prazosin and Nitroglycerine to achieve good control.
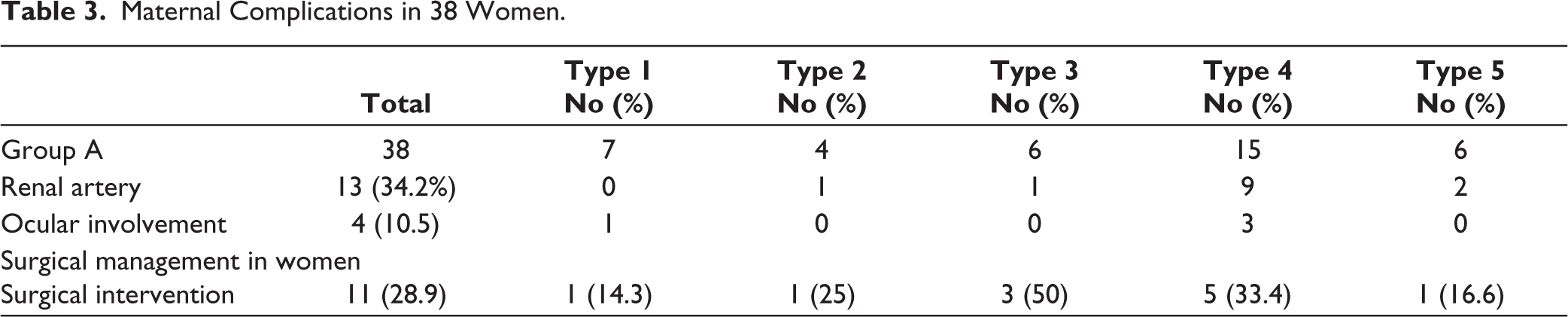
Table 3 shows details of renal and ocular involvement and surgical interventions in these women. The most common surgical procedure done in TA cases before conception was percutaneous transluminal angioplasty with stenting of the stenosed vessel. Vessel stenting was done for 11 (28.9%) women in all. Type 4 had the highest number of surgical interventions (5/15 = 33.3%).
Maternal Complications in 38 Women.
Comparison of Foetal Outcome Between Group A and Group B.

In this series, there was one maternal death. She was a gravida 4 para 1 live 1, miscarriages 2 mother with type 5 TA and chronic hypertension. She had accelerated hypertension, and flash pulmonary oedema and succumbed despite standard treatment.
Obstetric outcomes: Because of maternal medical condition labour was induced between 37 and 38 weeks in 21 cases (35.6%), and elective/prelabour caesarean section was done in 21 (35.6%). Caesarean section was done in 35 (59.3%) while 17 had vaginal birth (28.8%). The common reason for caesarean section was maternal condition in 10, followed by presumed foetal compromise in 6 (Table 3).
Foetal outcomes: Average gestational age at delivery was 35.7 weeks, average birth weight was 2,180 g, 6 babies (10%) were small for gestational age, and 19 (32.6%) babies were born before 37 weeks (Table 2). Type 5 TA had 62% preterm births with an average gestational age of 32.5 weeks, and an average birth weight of 1,600 g. NICU admission was seen in 8 (8.4%) neonates, 4 required non-invasive ventilation, one required ventilator support and the rest of the admissions were for prematurity. Stillbirths were 3 (5%), 2 were due to severe foetal growth restriction at 28 weeks, and one was at 36 weeks with an average gestational age foetus due to jaundice complicating pregnancy.
Secondary objective was to compare foetal outcomes in pregnancies in group A and group B. Fifty-eight pregnancies were included in group A, with 84% live births as shown and none of pregnancies were terminated because of TA. Group B had 33 previous pregnancies which were managed elsewhere, of which alive births were 24.2%, the miscarriage rate was 42.4% and 18% had stillbirths. Five pregnancies (15%) were terminated in the first trimester because of accelerated hypertension later evaluation showed TA. Multidisciplinary care was lacking in these cases (Table 4).
Discussion
TA is a rare inflammatory disease involving large arteries. Vessel inflammation leads to wall thickening, stenosis and thrombus formation. Pregnancy with TA is a high-risk state for vascular complications.
There were 38 women with 92 pregnancies of which 59 were managed at the study centre (group A) previous pregnancies33 in these same women were managed elsewhere (group B). Hypertension in pregnancy was observed in 67.7% of cases and most needed two to three antihypertensive medications. In group A, the live birth rate was 83%, and in group B it was 24%. Fifteen per cent underwent termination of pregnancy due to accelerated hypertension in group B.
A study done by Comarmond et al. concluded that TA increases 13—fold the odds of complications during pregnancy due to arterial hypertension. Disease activity of TA is independently associated with poor pregnancy outcomes. Factors independently associated with the risk of obstetric and maternal complications were a history of hypertension and tobacco use, Ishikawa group 2 and National Institute of Health score> 1 (OR =28.7[7.89–104.7]. 8
In this study, 15.7% of women with early onset hypertension (<20 weeks) in pregnancy were diagnosed denovo to have TA. Studies done earlier showed denovo diagnosis of TA in women with early onset hypertension 60% by Suri et al. 9 and 53% by Wong et al. 10 TA is also known as young female arteritis, so it is important to consider TA as a differential diagnosis of early-onset hypertension in pregnancy. In women with hypertension, physical examination with palpation of all peripheral pulses, checking blood pressure in all four limbs, and auscultation for vascular bruit help in the diagnosis of TA.
The most common complication was hypertension in pregnancy 40 (67.7%) cases. Chronic hypertension was the most common of all hypertensive disorders of pregnancy. Garikapati observed hypertension in 9% of cases. 11 In a study by David et al. chronic hypertension was seen in 43% and superimposed preeclampsia in 12.5% of cases. 3
Most cases needed two to three anti-hypertensive medications, with a combination of labetalol, methyldopa and nifedipine. The most challenging was in type 3 (three pregnancies) and type 4 (one pregnancy) TA where five anti-hypertensives were needed to achieve blood pressure control. David et al. showed 43% of cases with hypertension, where all of them required anti-hypertensives. It was also concluded that tight control of blood pressure is required to avoid complications and improve pregnancy outcomes. 3
In this study, the renal artery was involved in 34%(13 cases) and ocular in 10.5% compared to the study by David et al. in which 37% cases of the renal artery and 15% cases of ocular were involved. 3 Of 13 cases with renal artery involvement, 5 had a surgical intervention with a stent, and 3 had non-functioning kidneys.
Vascular complications were seen in 10.5% of cases, which included abdominal aorta aneurysm, inter iliac artery aneurysm, coarctation of aorta, and aorta flap dissection. In our series, three women had associated rheumatic heart disease.
The mainstay of treatment is immune modulators (steroids and immune suppressants). In this series 30% received steroids and azathioprine, 11% received only steroids, only azathioprine in 5% and heparin in 5%. In a study by David et al. 3 56% received steroids and immune suppressants and 25% received only steroids. He et al. described glucocorticoid usage at 23% and immune suppressants at 36%. 12
One maternal death occurred in a woman with type 5 TA at 28 weeks, with accelerated hypertension, flash pulmonary oedema and seizures. Maternal mortality was observed in a study by Wong et al. 10 and Mandal et al. 13 Maternal death was due to raised blood pressure and Cerebral vascular event. 13 Suri et al. 9 study showed one maternal death at 35 weeks due to accelerated hypertension and its complications. 6
In this series, one woman had eclampsia during the intrapartum period. Technical difficulties to get correct blood pressure and failure to act on raised blood pressure led to eclampsia.
In view of maternal complications with raised hypertension, patient education about checking blood pressures in the correct arm, compliance with medication and regular follow-up with a multidisciplinary team is important.
In group A, the live birth rate was 83%, the miscarriage rate of 10% and the stillbirth rate was 5%. In group B, 42% had miscarriages a live birth was 24%, stillbirth rate was 18%. Raised blood pressure was noticed for the first time in early pregnancy, had a termination of pregnancy in 15%, and later evaluation showed TA. Lack of multidisciplinary care led to the termination of the pregnancy. A similar trend was seen in a study by Hauenstein et al. where hypertension could not be controlled and so pregnancy was terminated. 14
The overall miscarriage rate was pregnancies managed elsewhere it was 42.4%. While for the same women, in this series, it was 10%. The cause of miscarriage was difficult to ascertain. It could not be confirmed whether it was due to disease activity. The spontaneous miscarriage rate ranged from 12% to 38% in various studies.10, 14, 15
The live birth rate in this series was 83%, whereas the study by Gupta et al. had a 50% live birth rate. 16 Other studies describe a live birth rate between 65% and 100%.4, 5, 17, 18 Overall stillbirth rate in this study was 15%. Whereas in pregnancies that were managed elsewhere for the same women, it was 18%. The stillbirth rate in cases managed in this series was 5%. One woman had a stillbirth at 36 weeks due to jaundice complicating pregnancy, and two cases were at 28 weeks with severe foetal growth restriction due to underlying medical conditions. David et al. study did not report intrauterine foetal demise or neonatal death. 3
Timing of birth is important in medical disorders complicating pregnancy, foetus is at risk of placental insufficiency hence planning delivery at 37 weeks would be beneficial. Thirteen per cent went into spontaneous labour, 35% needed induction of labour, and 35.6% required elective caesarean section. Induction rates varied from 25% in David et al. study to 47% in a study by Suri et al. and the rest set into labour spontaneously.3, 9 In this series caesarean section rate was 59%, other studies describe a similar rate of around 60%.10–12 Indications for the caesarean section were high blood pressure in 22.8%, previous caesarean section in 22.8% followed by presumed foetal compromise in 14.2%.
The mean gestational age at delivery was 35.3 weeks, mean birth weight was 2,180 g. Preterm birth in this study was 32.6%, which was higher compared to a study by Suri et al. (28%). David et al. had a 25% preterm birth rate, due to preterm premature rupture of membranes. 3 Wong et al. found there was no increase in induction of labour and preterm birth. 10
Small for gestational age foetuses were 10%. Eight babies (13.5%) required NICU admission. Foetal growth restriction was observed in 31% of cases in a study by David et al. 3 and it was 13% in a study by Tanacan. 15 Women with TA are at risk of preterm birth, foetal growth restriction and stillbirth, hence they need foetal growth monitoring once in 2–3 weeks from 28 weeks of gestation and weekly cardiotocograph from 32 weeks onwards till delivery and a more frequent antenatal visit from 28 weeks.
Strengths: Data was collected from case records from a single centre, so ascertainment of data is good.
Study limitation: The study was done retrospectively from 2005, data about disease activity based on acute phase reactants was incomplete as few cases presented late in pregnancy and for a few cases reports were not entered. Although there were 59 pregnancies, the sample size may not be sufficient to clear controversies.
Conclusion
Takayasu arteritis should be in the differential diagnosis when a young female presents with hypertension. Palpating all peripheral pulses and checking blood pressure in all four limbs at booking visit helps in the early diagnosis of TA. Adequate control of blood pressure and immune modulators to suppress inflammation help to improve outcomes. Women with TA are at risk of preterm birth, foetal growth restriction and stillbirth, hence they need foetal growth monitoring and timely delivery. Multidisciplinary care involving obstetricians, physicians, rheumatologists, anaesthetists and protocol-based maternal and foetal monitoring is of utmost importance to improve pregnancy outcomes in TA.
Footnotes
Acknowledgements
The authors thank all patients, their families and hospital staff who made this study possible.
Author Contributions
Kallur Sailaja Devi did the study design, data collection, analysis and compiled the article. All authors reviewed and approved the final article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
This study was approved by the Fernandez Foundation Ethics Committee (EC reference No 48_2022).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Being a retrospective collection of data individual consents were not taken. Blanket consent is taken at the time of antenatal booking and at the time of admission from all women.