
Abstract
Primary cutaneous cryptococcosis is a rare manifestation of Cryptococcus infection, which can present with diverse clinical manifestations, ranging from solitary nodules or papules to ulcerative lesions or cellulitis-like erythema. A 49-year-old female, a known case of rheumatoid arthritis who was on daily 4 mg of methyl prednisolone and 10 mg of tofacitinib, presented with painful, rapidly progressing ulcers over the right flank for 15 days. A differential diagnosis of pyoderma gangrenosum was considered since patient had rheumatoid arthritis. Histopathological examination of the skin biopsy from the edge of the ulcer showed granulomatous infiltrate with budding yeast forms surrounded by a thick capsule, suggestive of Cryptococcus neoformans. Fungal culture showed milky and creamy colonies on Sabouraud dextrose agar. Patient was initiated on oral Fluconazole 200 mg daily for three months. The ulcers healed completely after three months of treatment. To conclude, in patients with rapidly progressing ulcers, a differential diagnosis of cutaneous cryptococcosis must also be considered.
Keywords
Introduction
Primary cutaneous cryptococcosis (PCC) is an uncommon fungal infection that is limited to the skin and is caused by exogenous inoculation of Cryptococcus neoformans. It does not exhibit any symptoms of a systemic illness. 1
In immunocompromised individuals, such as cancer patients, persons with human immunodeficiency virus (HIV) infection and those undergoing long-term glucocorticoid and immunosuppressive medication following organ transplantation, cryptococcosis occurs as an opportunistic infection. 2 The lungs and central nervous system (CNS) are the primary sites of infection; skin invasion is thought to be an indicator of dissemination. 3
Here we report a case of PCC which presented as a rapidly progressive ulcer in a rheumatoid arthritis patient who was on systemic steroids and tofacitinib. Current literature suggests that tofacitinib, while being an efficacious and relatively safe treatment option for rheumatoid arthritis, is associated with an increase in opportunistic fungal and viral infections. 4
Case Report
A 49-year-old housewife hailing from rural north Karnataka presented with large painful ulcers over the right flank for the past 15 days. The ulcer was rapidly increasing in size, and was associated with purulent discharge. She subsequently developed two small ulcers in the adjacent area. There were no associated systemic complaints such as fever, cough, weight loss or gastrointestinal complaints. Patient did not give any history of antecedent trauma. The patient was a known case of rheumatoid arthritis and was on daily 4 mg of methyl prednisolone and 10 mg of tofacitinib for the past five years. Cutaneous examination revealed a 20 cm x 10 cm ulcer over the right flank with the adjacent ulcers measuring 2 cm x 2 cm each. These ulcers had irregular violaceous margins, undermined edges, and pale unhealthy granulation tissue at the floor with purulent discharge (Figure 1). No significant regional lymphadenopathy was appreciable in the patient
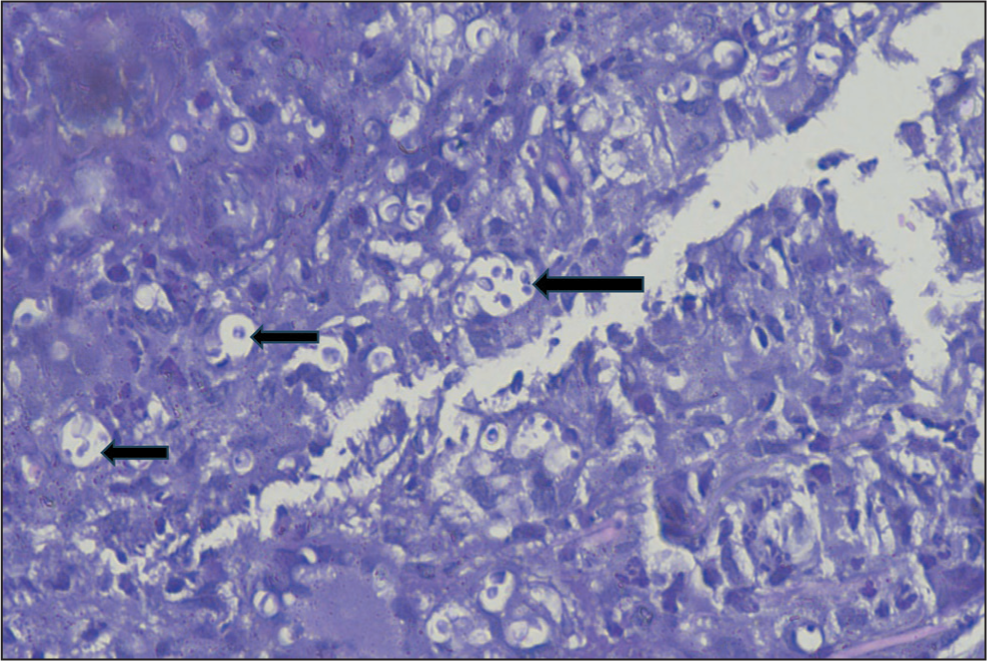
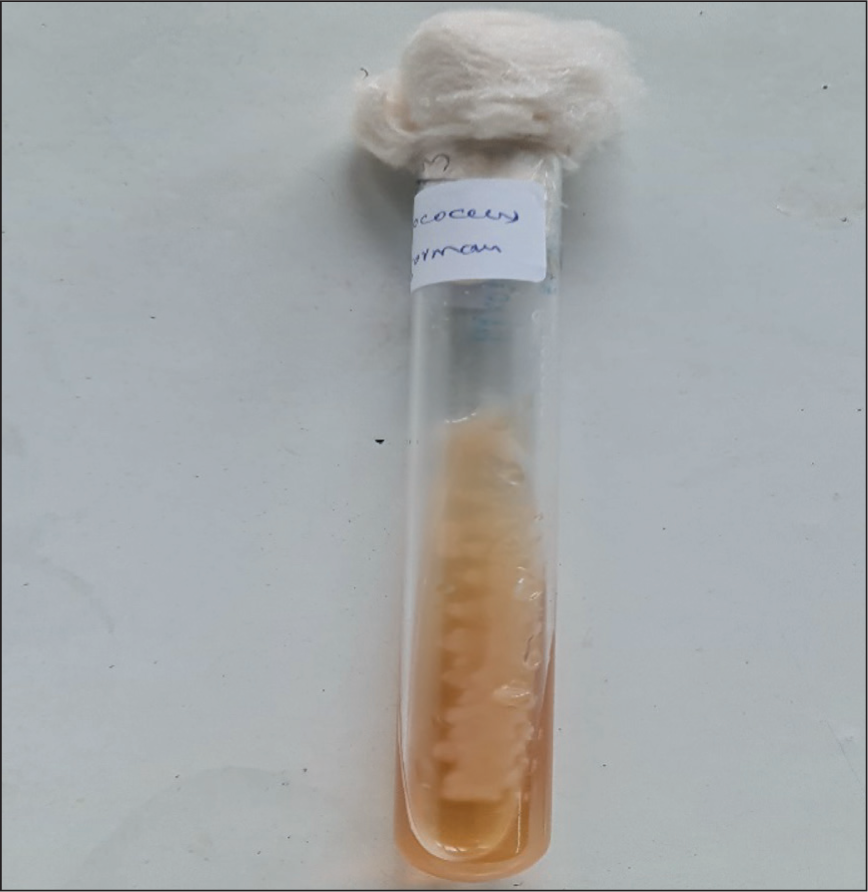
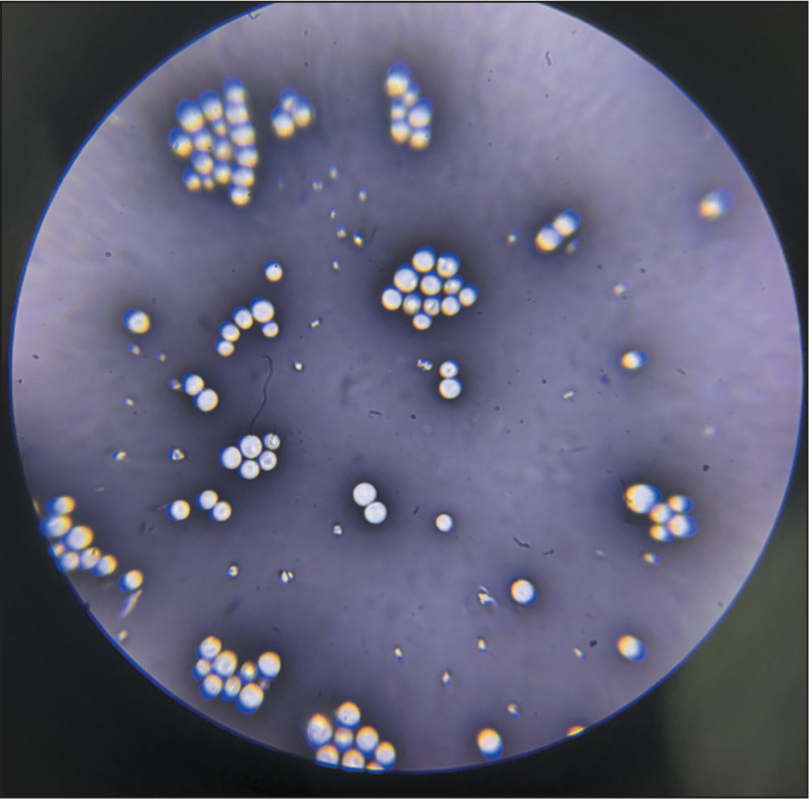
The differential diagnoses considered were pyoderma gangrenosum (PG) and atypical mycobacterial infection. Pathergy test was negative. Haematological and biochemical investigations, including complete blood count, liver function test (LFT) and renal function test (RFT), were within normal limits except for elevated blood sugar levels. Serological tests for HIV, hepatitis B surface antigen (HBsAg), hepatitis C virus (HCV) and Venereal Disease Research Laboratory test (VDRL) were non-reactive. Radiological investigations such as chest X-ray, high-resolution computed tomography (HRCT) thorax, CT brain and ultrasonography (USG) abdomen were normal. Histopathological examination of skin biopsy specimen from the edge of the ulcer showed granulomatous infiltrate with budding yeast forms surrounded by a thick capsule, suggestive of C. neoformans (Figure 2). Fungal culture of the skin tissue sample showed milky and creamy colonies of C. neoformans on Sabouraud dextrose agar (SDA; Figure 3). India ink preparation from the cultured growth demonstrated haloes (capsules) around the organisms (Figure 4). The patient was diagnosed with PCC and was initiated on systemic antifungal treatment consisting of oral fluconazole 200 mg once daily (OD) for three months. The ulcers showed complete resolution after three months of treatment (Figure 5).
Multiple Cutaneous Ulcers with Pale Unhealthy Granulation Tissue at the Floor Over the Flank Area.

Granulomatous Infiltrate with Budding Yeasts and Surrounded by Thick Capsule (Haematoxylin and Eosin (H & E) Stain-40×).
Fungal Culture Shows Milky and Creamy Colonies of C. neoformans on SDA.
India Ink Staining Shows Halo Around Organisms.
Healed Ulcers After Treatment with Oral Fluconazole for Three Months.

Discussion
C. neoformans has three variants, namely var. grubii, var. gattii and var. neoformans. C. neoformans generally causes life-threatening infections in immunocompromised hosts and less commonly is observed in healthy immunocompetent individuals. Excrements from pigeons and other birds, along with decaying wood, fruit and vegetables, are the primary sources of C. neoformans infection. C. neoformans var. grubii has a worldwide distribution. C. gattii, present in the tropics and subtropics, is found in several arboreal species, including multiple varieties of eucalyptus trees; however, it is not found in bird droppings.2,5 The fungus can infect the skin directly through traumatic injuries to cause PCC, or they can move through the haematogenic route to cause secondary cutaneous cryptococcosis. 6 In our case, direct inoculation by traumatic injury might be a probable cause of infection.
PCC is a distinct clinical entity that should not be confused with secondary cutaneous cryptococcosis, which occurs due to haematogenous dissemination from a systemic focus, most commonly pulmonary or meningoencephalitic cryptococcosis. Secondary cutaneous cryptococcosis infection usually affects immunocompromised hosts, whereas immunocompetent hosts are less likely to have it.7,8 As in secondary cutaneous involvement, acneiform lesions, pustules, purpura, vesicles, nodules, abscesses and sinuses, ulcers, granulomas and cellulitis can all be symptoms of PCC. The patient in our case presented with an uncommon manifestation of a rapidly expanding cutaneous ulcer which did not improve with antibiotic treatment.
The patient was also immunosuppressed due to daily 4 mg of methyl prednisolone and 10 mg of tofacitinib for rheumatoid arthritis. Interferon-gamma (IFN-γ) and granulocyte-macrophage colony-stimulating factor (GM-CSF), two cytokines that signal through the JAK-STAT pathway, are essential for host defence against opportunistic pathogens. 9 JAK1 is phosphorylated by four cytokine-receptor families, one among which are the class II cytokine receptors, including the IFN-γ receptor. JAK2 is involved in the signal transduction of the interleukin-3 (IL-3) receptor family (IL-3R, IL-5R) and GM-CSF receptor. 10 While it may not be possible to conclusively infer a causal association between the tofacitinib therapy in this patient and the ensuing cryptococcal infection, such association is likely as the patient was on a low dose of systemic corticosteroid and had only mild hyperglycaemia.
A total of only 15 confirmed serious opportunistic infections (excluding tuberculosis (TB) and disseminated herpes zoster (HZ)) were found through analysis of the pooled safety data across the tofacitinib clinical trials and long-term extension studies (9,291 patients, 34,223 patient-years). Candida was the most common pathogen, followed by Cryptococcus, cytomegalovirus, histoplasmosis and Pneumocystis jirovecii. 9
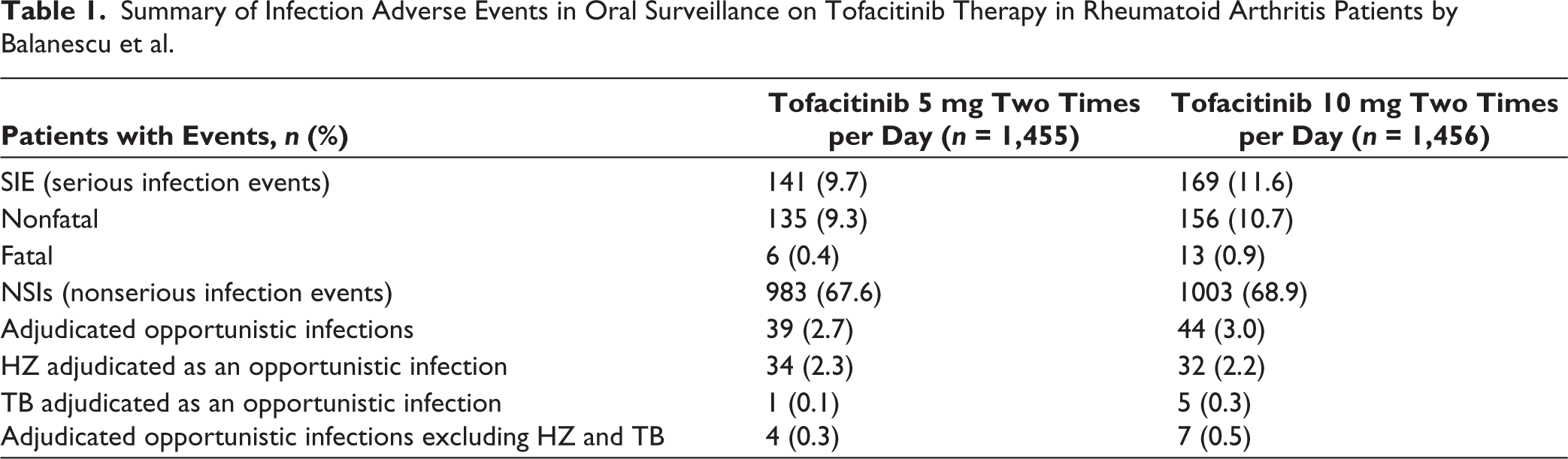
Table 1 shows adverse reactions in rheumatoid arthritis patients who have been treated with tofacitinib therapy. According to Balanescu et al., the most common adjudicated opportunistic infections in patients treated with tofacitinib (5 mg and 10 mg twice daily (BD)) were HZ, followed by TB. Other opportunistic infections, excluding HZ and TB, were 4 and 7 respectively in patients treated with tofacitinib 5 mg BD and 10 mg BD. 11
Summary of Infection Adverse Events in Oral Surveillance on Tofacitinib Therapy in Rheumatoid Arthritis Patients by Balanescu et al.
In another study conducted by Cohen et al. it was found that opportunistic infections excluding TB occurred in 25 out of 4,789 patients. Eight patients had oesophageal candidiasis (some of which were incidental findings on endoscopies done for other reasons), six patients had cytomegalovirus infection/viremia, three patients had cryptococcal infection (two cases of pneumonia and one case of meningitis), three patients had Pneumocystis jiroveci pneumonia, two patients had nontuberculous mycobacteria in the lung and one patient had BK virus, in addition to the two cases of multidermatomal HZ. 12
There have been only a few cases previously reported in the literature describing secondary cutaneous cryptococcosis occurring as an adverse event following treatment with tofacitinib and other JAK inhibitors. Seminario-Vidal L et al. reported a case of a 65-year-old Caucasian male with severe plaque psoriasis and psoriatic arthritis who had been receiving tofacitinib therapy for six months. He had a 10-week history of worsening nasal congestion, intermittent fever, nonproductive cough and dyspnoea. Pulmonary cryptococcosis was diagnosed after his serum tested positive for cryptococcal antigen, although no confirmatory fungal culture was obtained. He was treated with fluconazole 400 mg/day for six months, which led to a quick recovery. 13
Sánchez et al. reported the case of a 64-year-old lady who had a history of rheumatoid arthritis and had been on 5 mg of tofacitinib twice daily and 5 mg of prednisolone daily for the past three years. She was hospitalised after head trauma, and her cerebrospinal fluid culture revealed C. neoformans. She was diagnosed with acute meningitis due to C. neoformans and disseminated cryptococcosis. Despite treatment with liposomal amphotericin B and fluconazole 400 mg per day, her condition deteriorated, and she ultimately passed away. 14
Chen et al. reported another case involving a 75-year-old woman with post-polycythaemia vera myelofibrosis who had been on ruxolitinib for four years to manage her splenomegaly and constitutional symptoms. She presented with two prominent, crimson, readily bleeding mass lesions over her left abdominal region which developed over two months. Histopathology showed yeast-like microorganisms with thick, variable-sized capsules suggestive of cryptococcosis. A blood cryptococcal antigen titre of 1:256 confirmed disseminated cryptococcosis with cutaneous involvement. 15
Although pulmonary and CNS cryptococcosis have been documented as adverse events associated with tofacitinib use in rheumatoid arthritis, we could not find any report of PCC in this context. This case report aims to report its occurrence and highlights the clinical features of PCC to facilitate early detection and thereby minimise the potentially fatal risk of dissemination. To the best of our knowledge, PCC has not been previously reported in literature as an adverse event with tofacitinib therapy.
Cryptococcal skin lesions are usually indicators of a systemic cryptococcal infection. Therefore, detection of Cryptococcus on biopsy or culture should prompt additional appropriate investigations like chest radiography, thoracic CT, blood and urine cultures, CSF analysis and HIV serology to rule out systemic infection. 16
Fluconazole (200-400 mg/day), itraconazole (200–400 mg/day) and amphotericin B (0.5–1 mg/kg/day) are standard treatments for PCC. The patient’s immunological state and degree of involvement determine the dosage and length of treatment. 3 In our case, the patient was treated with fluconazole 150 mg /day for one week followed by 200 mg/day for three months, and the ulcers were healed completely. The patient was subsequently lost to follow-up. Upon telephonic enquiry, it was found that the patient had succumbed to underlying sepsis.
Conclusion
To conclude, PCC presents a diagnostic challenge due to its varied clinical manifestations, overlap with other skin conditions and the need for histopathological and mycological confirmation. Thorough evaluation for detecting other possible foci of cryptococcal infection is of utmost importance. Prompt recognition and diagnosis are crucial, particularly in immunocompromised individuals, to initiate appropriate treatment and prevent potentially fatal dissemination.
Footnotes
Acknowledgements
I extend my sincere gratitude to Dr. Manjunath Shenoy (HOD, Department of Dermatology, Venerology & Leprosy) and Dr. Swathi (Final-year Postgraduate) for the general support and guidance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Our institution does not require ethics approval for reporting individual cases or case series.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Not Applicable.