
Abstract
Dear Editor,
A young male presented with a three-year history of inflammatory back pain, initially characterised by episodic flares that were partially alleviated by nonsteroidal anti-inflammatory drugs (NSAIDs). Backache was accompanied by intermittent polyarthralgia affecting multiple small joints of the hands and feet. Over time, the lumbar pain evolved into persistent, nonradiating, mechanical discomfort, significantly impairing daily activities. The patient reported difficulty with prolonged standing. Notably, there was no history of preceding infections such as fever, weight loss, diarrhoea, or dysuria, nor any extra-articular manifestations such as uveitis or psoriasis. There was no history of spondyloarthritis (SpA) or autoimmune conditions in family. Patient denies any history of multiple sexual partners, recent exposures or substance abuse.
On examination, the patient exhibited hypermobility, evidenced by hyperextension of the elbows, and knees (Beighton score 6). The flexion abduction external rotation (FABER) test elicited back pain. Single leg rise test was performed bilaterally without difficulty, and the modified Schober’s test showed spinal flexion of 6 cm. No active peripheral joint involvement was observed. Systemic and general examinations were otherwise unremarkable.
Laboratory parameters were largely unremarkable, including inflammatory markers. He tested positive for human leukocyte antigen B27 (HLA-B27) by polymerase chain reaction method. Based on a suspected diagnosis of SpA, his primary care physician prescribed sulfasalazine 3g/day and referred him to our institute. Repeat C-reactive protein (CRP) revealed minimal elevations, which correlated temporally with episodes of polyarthralgia. The serum uric acid level was 7.2 mg/dL. The autoimmune profile, including rheumatoid factor, anti-cyclic citrullinated peptide (CCP), anti nuclear antibody (ANA), and anti phospholipid antibody (APLA), was negative. X-ray of the pelvis and spine revealed corner erosions, collapse L3 vertebrae and right-sided grade I sacroiliitis (Figure 1A and F). Ultrasonography did not suggest any peripheral synovitis or enthesitis. A magnetic resonance imaging (MRI) of the spine and sacroiliac (SI) joints was conducted, which revealed degenerative disc changes, corner erosions and collapse at L3 with normal SI joints (Figure 1C and H-J). A dual-energy X-ray absorptiometry (DEXA) scan was ordered to rule out osteoporotic fractures and screen for secondary causes of osteoporosis, all of which were negative.
Atypical clinical features, including mechanical pain, lack of response to NSAIDs, normal inflammatory markers and nonspecific radiographic findings, necessitated consideration of alternative diagnoses. Computed tomography (CT) scan of the SI and spine suggested significant spinal lesions with minimal involvement of SI joints (Figure 1B and G). These imaging findings, combined with episodic pattern, raised suspicion for conditions such as crystal arthropathy or chronic reactive arthritis. Ultrasonography findings showed no evidence of synovitis or double contour sign, leading to further evaluation with dual-energy CT (DECT) of the axial skeleton. DECT identified extensive monosodium urate (MSU) crystal deposition in axial skeleton, along with nerve root compression in sacral foramina (Figure 1D and K-M). A final diagnosis of axial gout was established. In absence of typical clinical features, isolated presence of HLA-B27 was not considered contributory. Patient was initiated on colchicine, and febuxostat for gout management, along with a combination therapy of nortriptyline and pregabalin to address canal stenosis related symptoms.
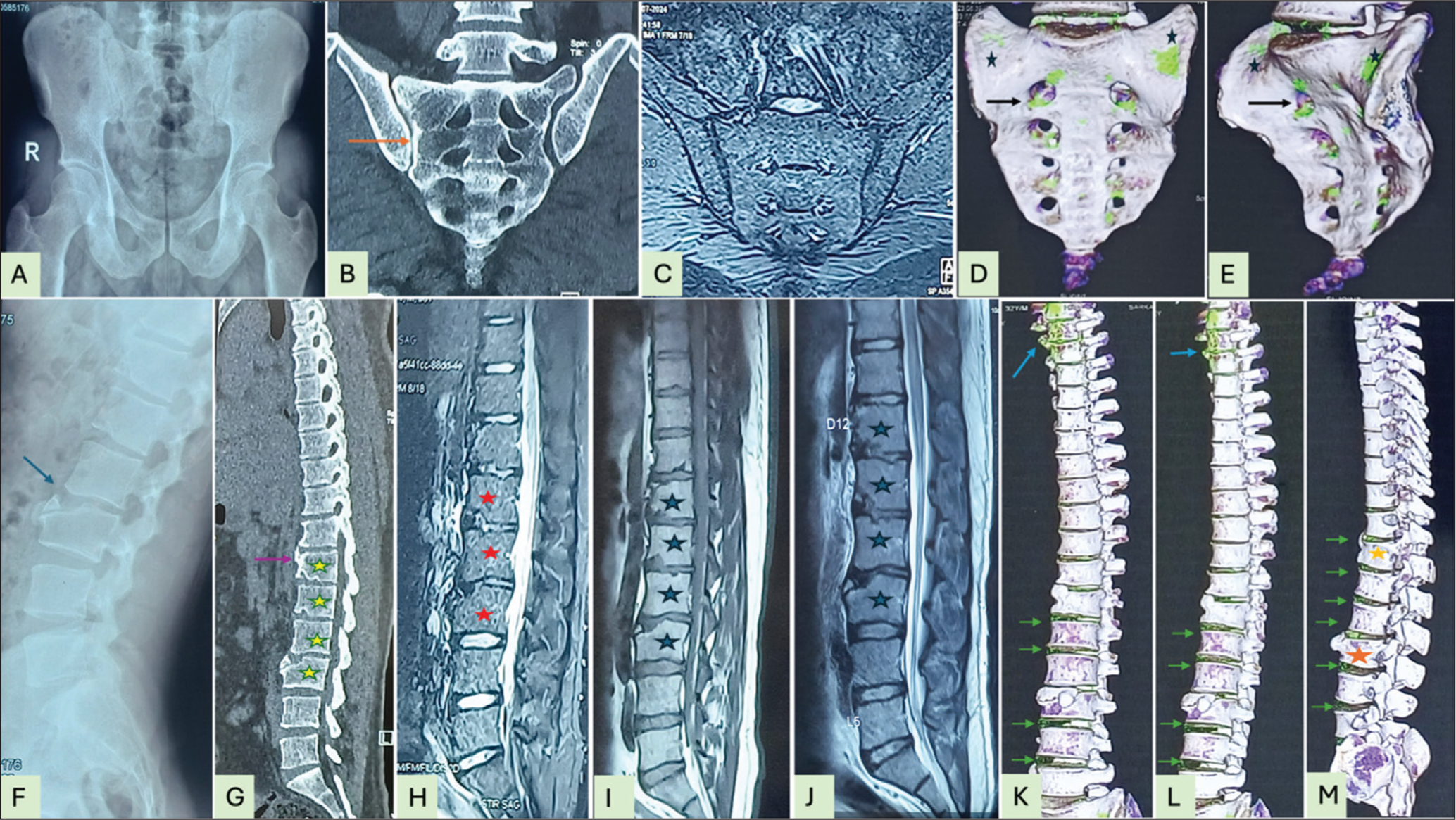
(F-M) Serial Images of Dorsolumbar Spine: (f) Lateral spine X-ray revealing vertebral corner erosion at L1–3 and bony fragmentation at L3 (blue arrow); (g), CT scan showing T12–L3 corner erosions (yellow stars), a syndesmophyte at T11-T12 (purple arrow), and a corner fracture at L3; (h), MRI (STIR) showing reduced aqueous signal in T12-L3 intervertebral discs due to degenerative disc disease (red arrow) without BME; (i), T1 MRI confirming nontraumatic fracture at T12 and L3 with corner erosion at L2; (j), T2 MRI documenting chronic spondylitis and minimal fatty metaplasia around the eroded vertebral borders (blue stars); (K, L, M), DECT of the spine showing extensive MSU crystal deposition (crystal icing) over multiple intervertebral discs (green arrows), foaming over the C7–T2 level (blue arrow), nonmarginal erosion with an overhanging edge and a giant osteophyte (red star), and bony bridging (yellow star) in anterior (k), oblique (l), and lateral (m) views.
Axial gout, a rare and underrecognised manifestation of gout involving the axial skeleton, often mimics other rheumatological disorders, posing significant diagnostic challenges. The prevalence of axial involvement in gout ranges from 15.8% to 29%.1,2 Clinical presentations are diverse, ranging from severe spinal pain to neurological complications, including canal stenosis, cord compression and acute radiculopathy. 3 Lumbar spine involvement is almost universal, and DECT has proven to be a valuable tool for its diagnosis.3,4 A notable association with diabetes mellitus and current peripheral tophi (not previous history) has been observed.1,2 Early recognition and timely initiation of therapy are crucial.
Differentiating gout from SpA based solely on back pain remains a diagnostic challenge. In cases of axial gout, a high index of suspicion is essential, as both conditions share overlapping clinical features, including a male predominance, lumbosacral spine involvement and the presence of dactylitis. A systematic review of spinal gout reported a higher mean age of onset (51.9 years), with approximately 30% of cases presenting with spinal cord or nerve compression symptoms. 5 Although rare, co-existence of gout and SpA has been documented (1.96%), likely reflecting shared risk factors. 6 Imaging modalities and synovial aspiration help to differentiate in a more definitive way. A comparative study of CT imaging of the SI joints in gout versus SpA demonstrated that gout is characterised by broad, deep para-articular erosions with sclerotic margins, overhanging edges and a multilobulated base, typically in the absence of significant subchondral sclerosis (<4.5 mm), frequently in association with tophi (65.7%). 7 In contrast, SpA is associated with numerous erosions accompanied by marked subchondral sclerosis. While MRI evidence of classical bilateral acute sacroiliitis—manifested as bone marrow oedema—may support a diagnosis of SpA, confirmation with DECT is often necessary. The absence of typical sacroiliitis findings on MRI, coupled with the presence of MSU crystal deposition on DECT, as seen in our patient, is indicative of axial gout.
DECT is a valuable diagnostic modality for gout; however, its clinical utility is limited by restricted availability and the need for extensive post-processing adjustments. Its diagnostic sensitivity is suboptimal during initial attacks and in patients with a shorter disease duration (<24 months). 8 Moreover, DECT may yield false-negative results in the presence of dense liquid tophi or calcified tophi, owing to subthreshold attenuation and signal obscuration, respectively. 9 Usually, longer disease duration, tophaceous disease and high serum uric acid level predict better MSU crystal volume.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written informed consent was taken.