
Abstract
Background:
Emerging evidence suggests a potential link between coronavirus disease 2019 (COVID-19) and the development of autoimmune diseases. This study aims to assess the pooled risk of this association.
Methods:
A Literature search was conducted across three databases. Full-text, English-language cohorts between 2019 and 2023 were included. Standard meta-analysis methods were employed using the random-effects model and heterogeneity was assessed using the I2 statistic.
Results:
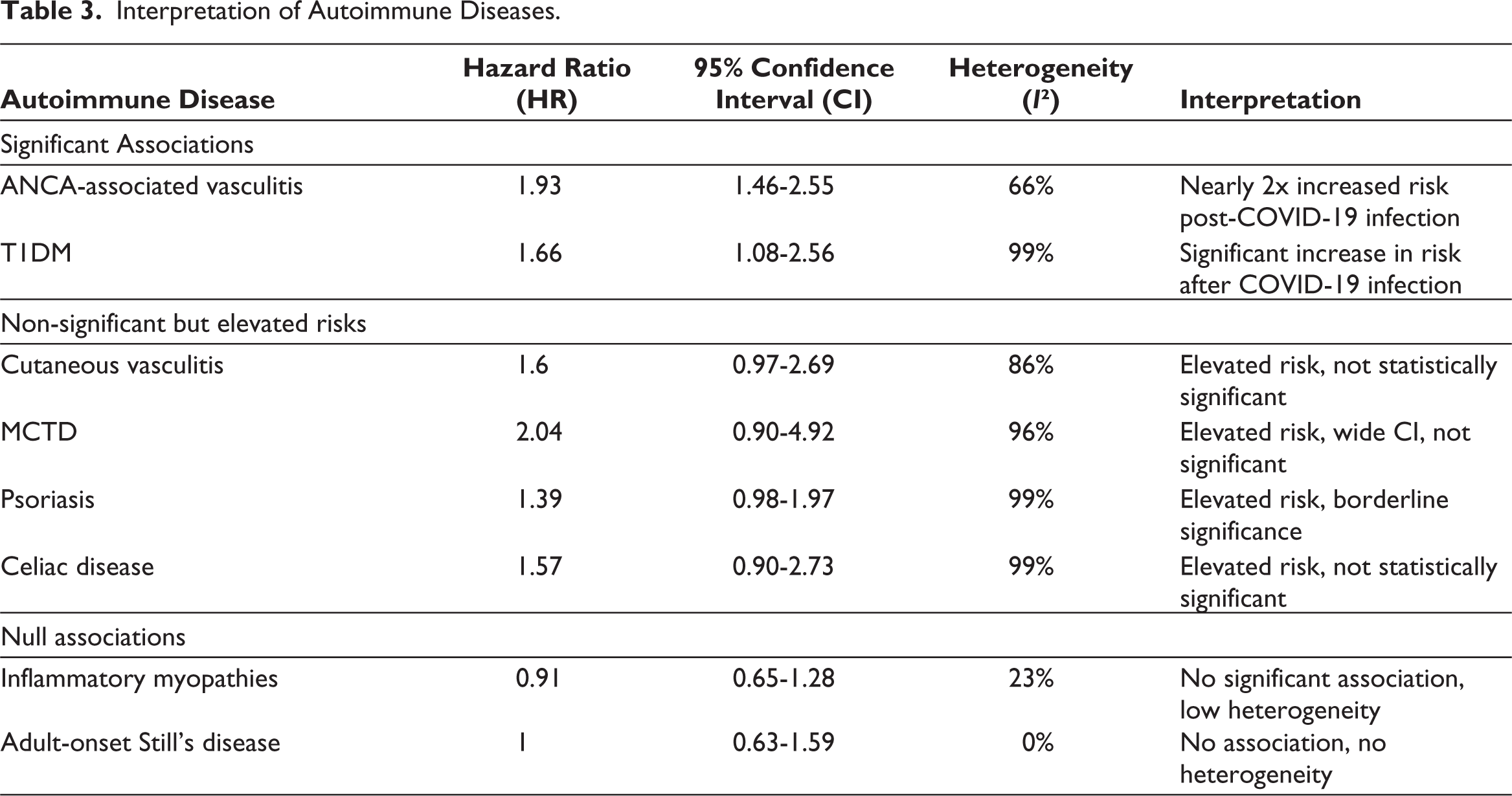
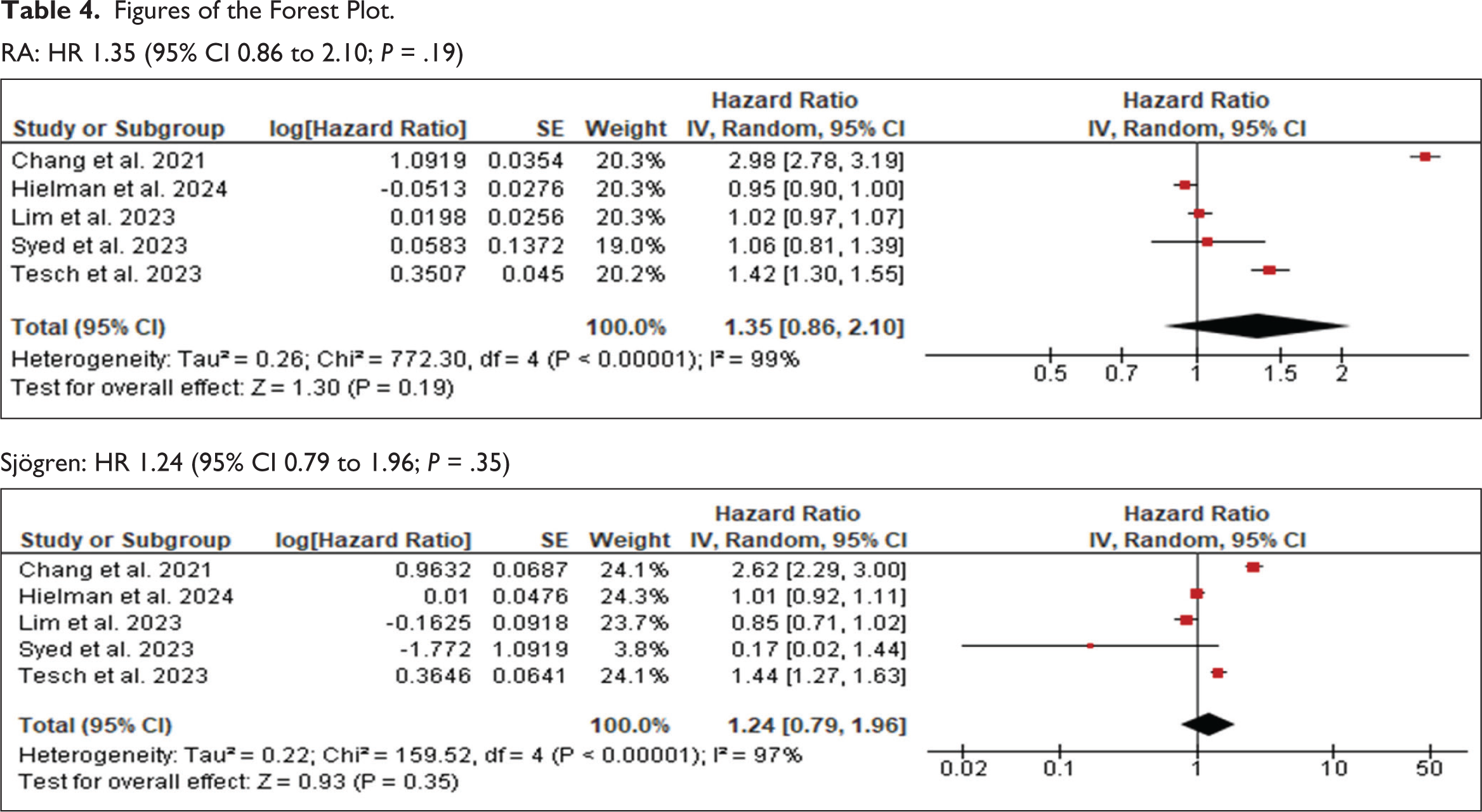
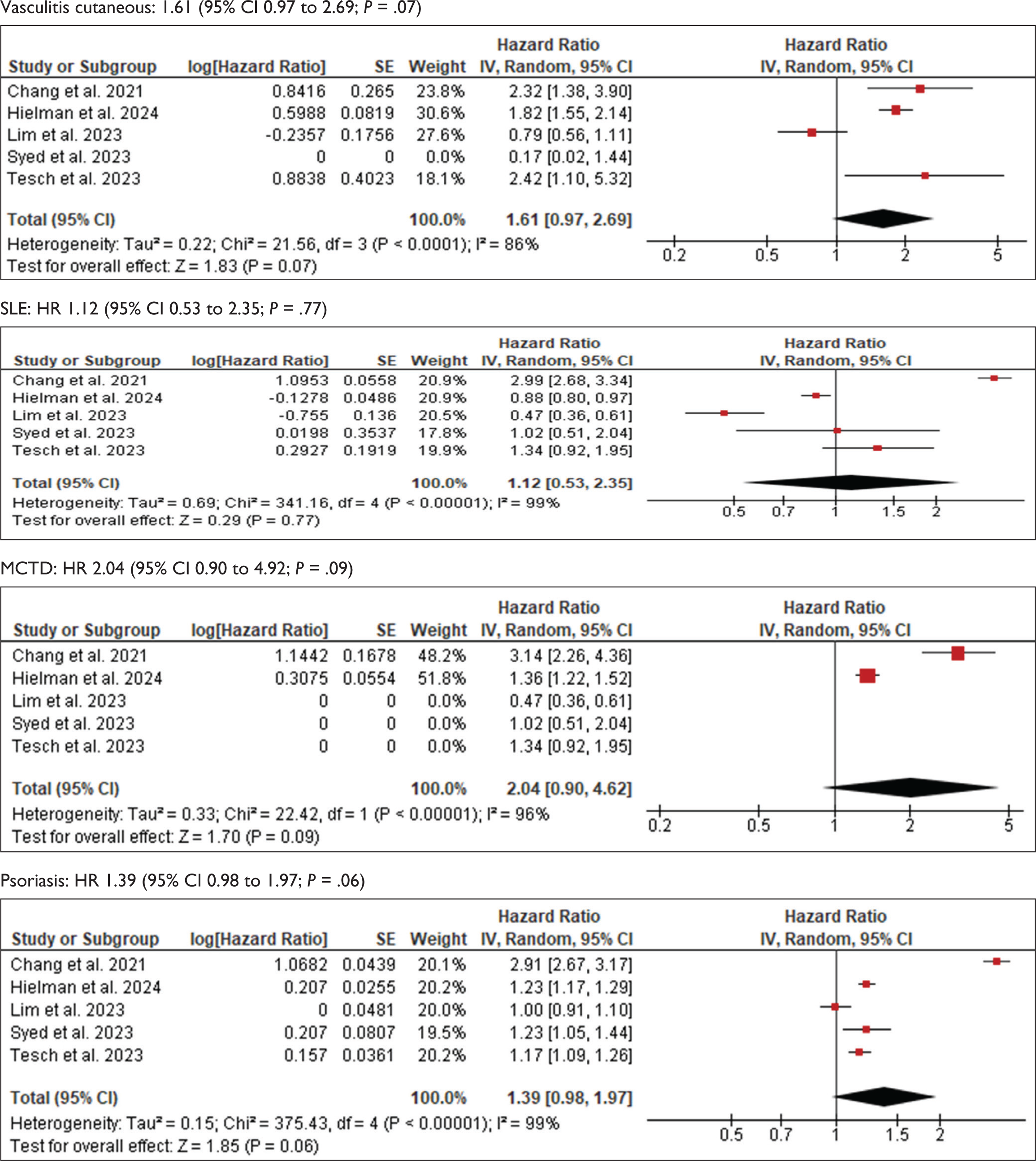
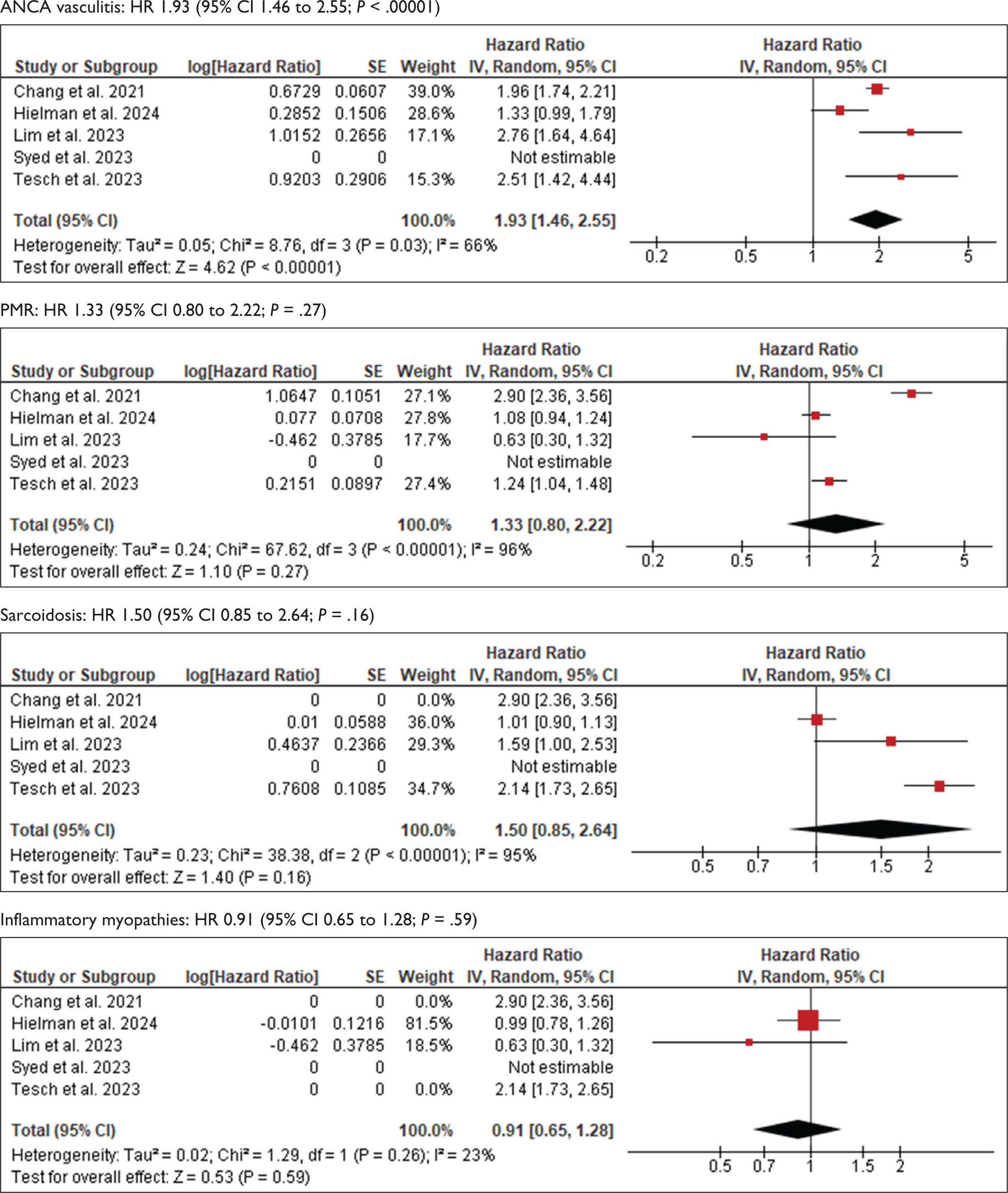
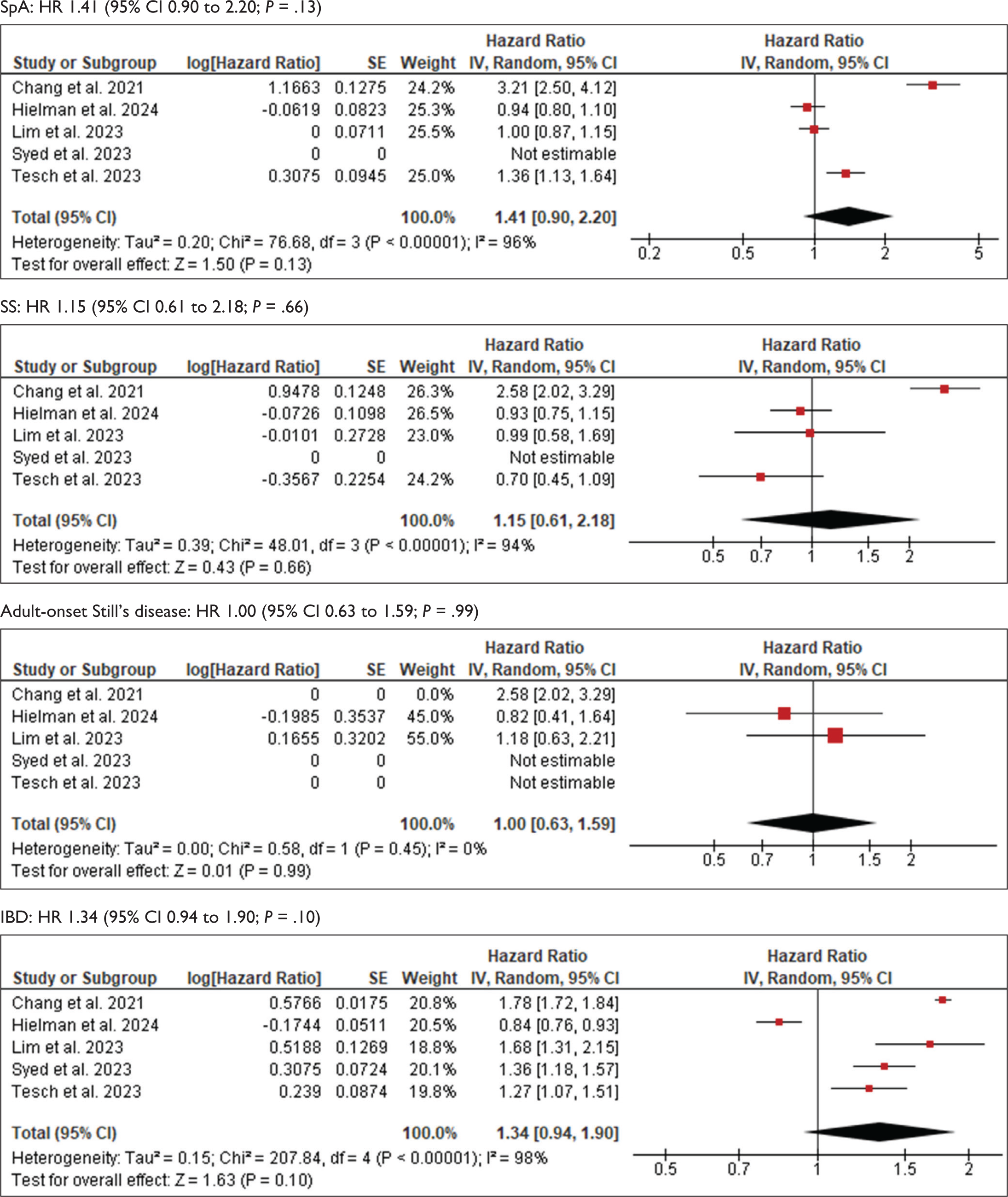
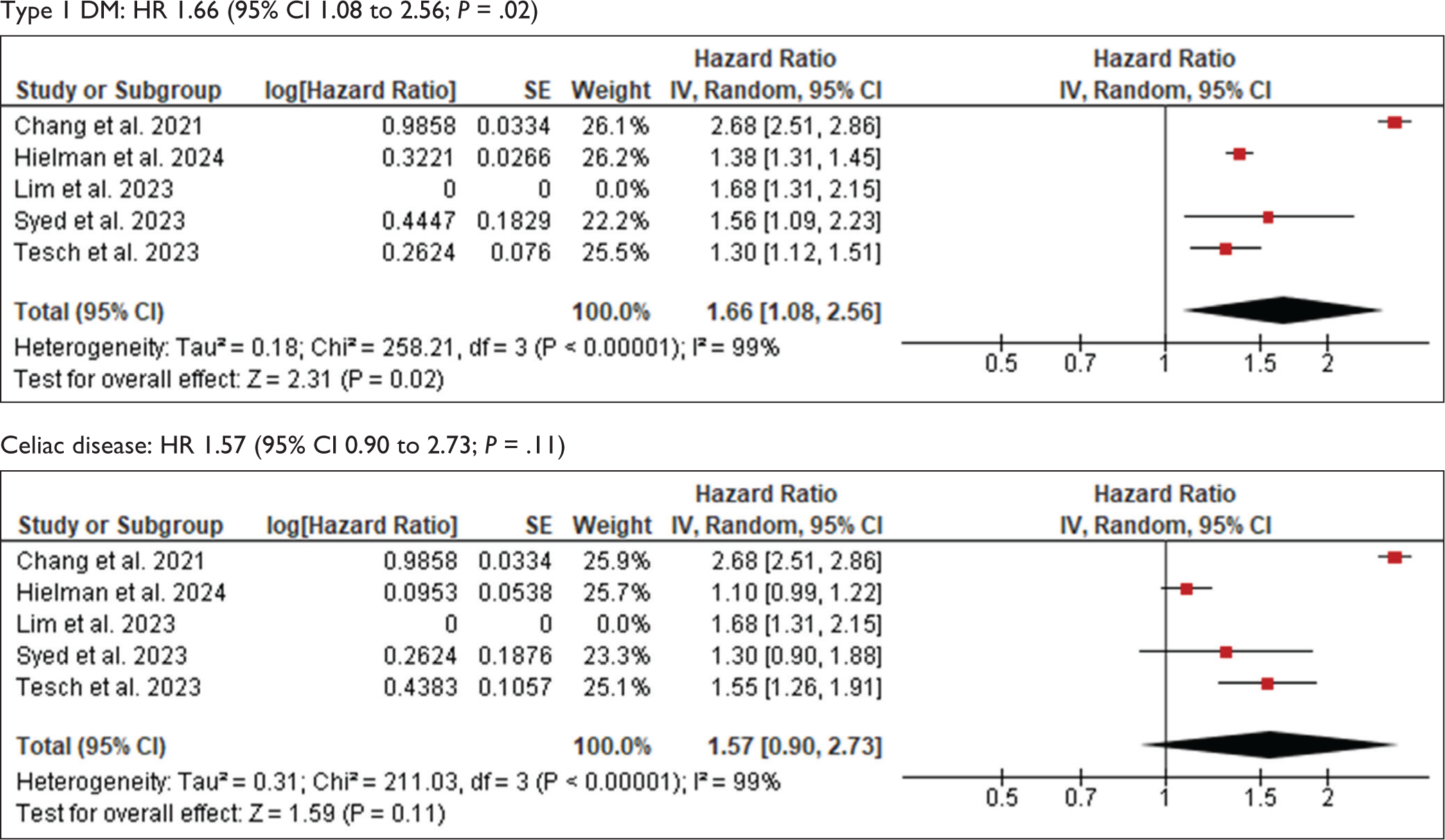
Data analysed across five studies revealed the following hazard ratios, confidence intervals (CIs) and I2 heterogenicity; systemic lupus erythematosus (SLE) 1.12 (CI [0.53-2.35, I2 0.99]); RA 1.35 (CI [0.86–2.10, I2 0.99]); psoriasis 1.39 (CI [0.98–1.97, I2 0.99]); Sjögren 1.24 (CI [0.79–1.96, I2 0.97]); PMR 1.33 (CI [0.80–2.22, I2 0.96]); spondyloarthropathies 1.41 (CI [0.90–2.20, I2 0.96]); anti-neutrophil cytoplasmic antibody (ANCA) vasculitis 1.93 (CI [1.46–2.55, I2 0.66]); cutaneous vasculitis 1.6 (CI [0.97–2.69, I2 0.86]); mixed connective tissue disease (MCTD) 2.04 (CI [0.90–4.92, I2 0.96]); sarcoidosis 1.50 (CI [0.85–2.64, I2 0.95]); inflammatory myopathies 0.91 (CI [0.65–1.28, I2 0.23]); SS 1.15 (CI [0.61–2.18, I2 0.94]); adult-onset Stills disease 1.00 (CI [0.63–1.59, I2 0]); IBD 1.34 (CI [0.94–1.90, I2 0.98]); celiac disease 1.57 (CI [0.90–2.73, I2 0.99]); type 1 diabetes mellitus (T1DM) 1.66 (CI [1.08–2.56, I2 0.99]).
Conclusion:
This meta-analysis identifies an increased risk of ANCA-associated vasculitis and type 1 diabetes mellitus (T1DM) following COVID-19 infection. While some conditions, such as cutaneous vasculitis and MCTD, show trends toward increased risk, additional studies are necessary to confirm these associations. Further research is crucial to understand the underlying mechanisms and long-term implications of COVID-19-induced autoimmunity.
Keywords
Abbreviations
Coronavirus disease 2019
Severe acute respiratory syndrome coronavirus 2
Mixed connective tissue disease
Anti-neutrophil cytoplasmic antibody
Acute respiratory distress syndrome
Inflammatory bowel disease
Systemic lupus erythematosus
Diabetes mellitus
Systemic sclerosis
Rheumatoid arthritis
Polymyalgia rheumatica
Angiotensin-converting enzyme 2 (ACE2) receptor
Introduction
In 2019, coronavirus disease 2019 (COVID-19) was first reported in Wuhan, China and has since spread rapidly worldwide. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a positive-polar single-stranded Ribonucleic acid (RNA) (ssRNA) virus that is transmitted directly by respiratory droplets. 1
COVID-19 is characterised by a wide range of presentations, from asymptomatic or flu-like illnesses, which can cause fever, dry cough, fatigue, headache and loss of taste and smell, to severe pneumonia leading to acute respiratory distress syndrome (ARDS), with subsequent respiratory failure requiring mechanical ventilation. 2
Beyond the immediate respiratory and systemic effects of the virus, there is a growing concern about the potential long-term consequences of COVID-19, particularly regarding its influence on the immune system and the development of autoimmune diseases. 3 Viruses are known to be implicated in the development of autoimmunity through various molecular mechanisms. 4 To supplement this, several studies have noted the presence of autoantibodies in patients with COVID-19, 5 and some have described autoimmune and rheumatic musculoskeletal diseases arising as a consequence of SARS-CoV-2 infection. 6 The clinical spectrum of autoimmune-related manifestations in COVID-19 patients ranges from organ-specific (e.g., cutaneous vasculitis, immune thrombocytopenic purpura, transverse myelitis, Guillain–Barré syndrome) to systemic autoimmune and inflammatory conditions (e.g., systemic vasculitis, multisystem inflammatory syndrome [MIS]), hemophagocytic lymphohistiocytosis and systemic lupus erythematosus (SLE). 7 The temporal association between COVID-19 infection and the onset of these autoimmune diseases raises questions regarding causality and underlying immunological mechanisms. This meta-analysis aims to assess the pooled risk of new-onset autoimmune conditions following SARS-CoV-2 infection.
Methods
To comprehensively assess the current state of knowledge on autoimmune diseases post-COVID-19 infection, a systematic literature search was conducted across three major databases: PubMed, the Cochrane Library and Google Scholar. The search strategy involved five rounds of data exploration to ensure thorough coverage of relevant studies.
Search Terms
The search process was carried out following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 8 The search terms included a combination of keywords such as ‘COVID-19’, ‘SARS-CoV-2’, ‘rheumatoid arthritis’, ‘Sjögren syndrome’, ‘SLE’, ‘cutaneous and anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis’, ‘psoriasis’, ‘mixed connective tissue disease (MCTD )’, ‘inflammatory bowel disease (IBD)’, ‘polymyalgia rheumatica (PMR)’, ‘sarcoidosis’, ‘spondyloarthropathies’, ‘inflammatory myopathies’, ‘systemic sclerosis’, ‘adult-onset Still’s disease’, ‘celiac disease’ and ‘type 1 diabetes mellitus (T1DM)’. These terms were used in various combinations to ensure that all relevant studies were identified.
Inclusion Criteria
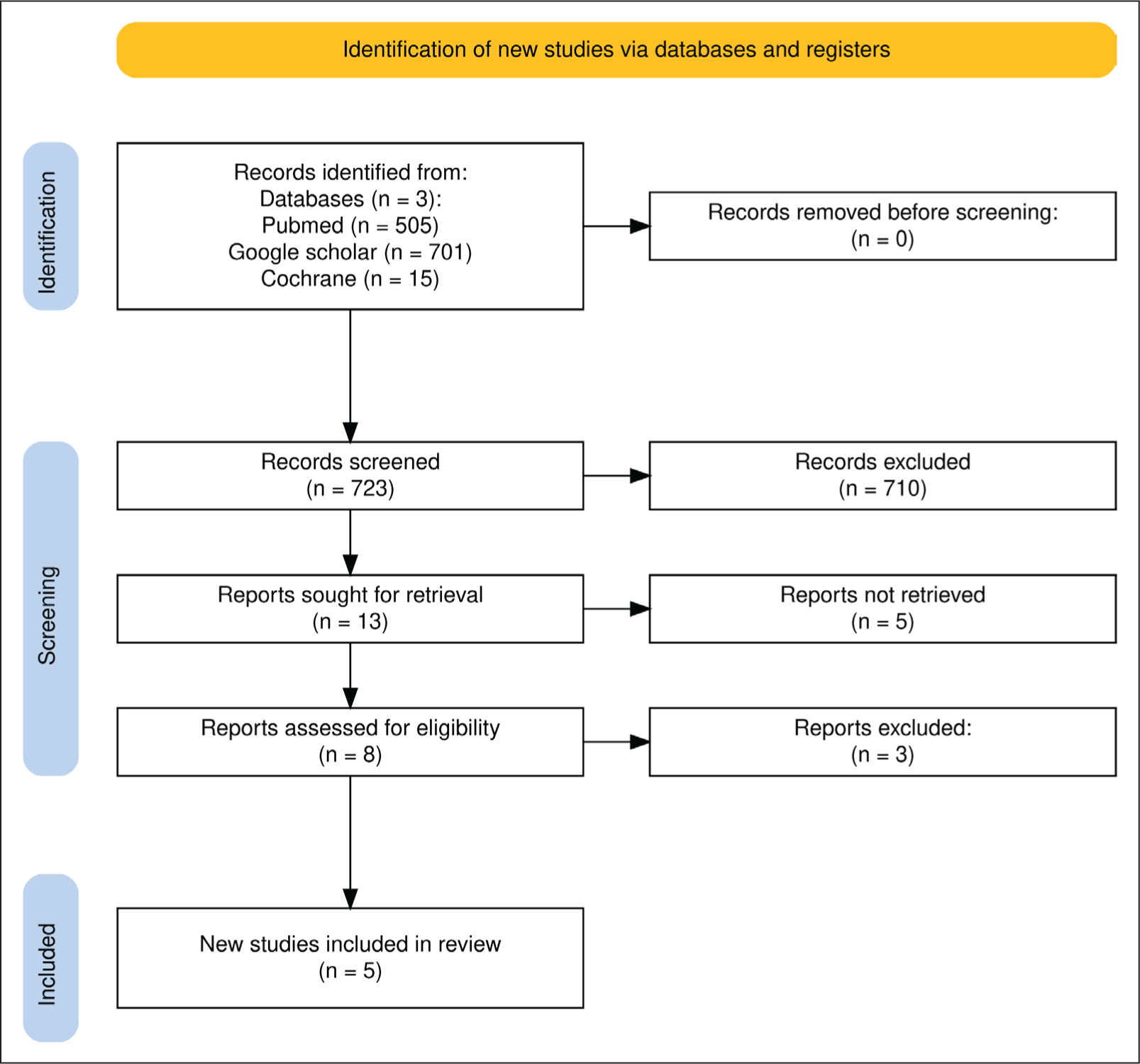
After five rounds of thorough literature search using the search terms, studies were selected based on the following criteria (Figure 1):
Study design: Only full-text, English-language cohort studies that compared groups with and without COVID-19 infection were included. Publication period: Studies published between 2019 and 2023 were considered to capture recent trends and findings. Diseases of interest: The analysis focused on a broad range of autoimmune diseases, including rheumatoid arthritis, Sjögren’s syndrome, SLE, cutaneous and ANCA-associated vasculitis, psoriasis, MCTD, IBD, PMR, sarcoidosis, spondyloarthropathies, inflammatory myopathies, systemic sclerosis, adult-onset Still’s disease, celiac disease and T1DM in association with COVID-19.
PRISMA Workflow Chart.
Exclusion Criteria
Studies were excluded if they did not meet the specified inclusion criteria. These included non-cohort studies, animal, in vivo and in vitro studies, those published outside the specified time frame and those not available in full-text or in English.
Statistical Methods
Data was analysed using RevMan 4.2.1. Pooled hazard ratios with 95% confidence intervals (CIs) were calculated using Mantel-Haenszel methods. Random- or fixed-effects models were applied based on heterogeneity (Higgins I2). Statistical significance was set at P < .05. Risk of bias was assessed using Risk of Bias (RoB) 2.0.
Result
Study Selection and Characteristics
A total of 7,97,295 records were identified through the literature search. After removing duplicates and screening titles, abstracts and full texts, five cohort studies met the inclusion criteria. These studies, namely Chang et al. 9 Hileman et al. 10 Lim et al. 11 Syed et al. 12 and Tesch et al. 13 collectively analysed data from 11,276,180 patients, including individuals with confirmed COVID-19 and matched control groups without COVID-19 (Table 1). The cohorts were geographically diverse, with studies conducted in the United States, the United Kingdom, South Korea, Taiwan, Canada and Germany. The included studies varied in sample size and follow-up duration (Table 2):
Study Characteristics and Vaccination Status.
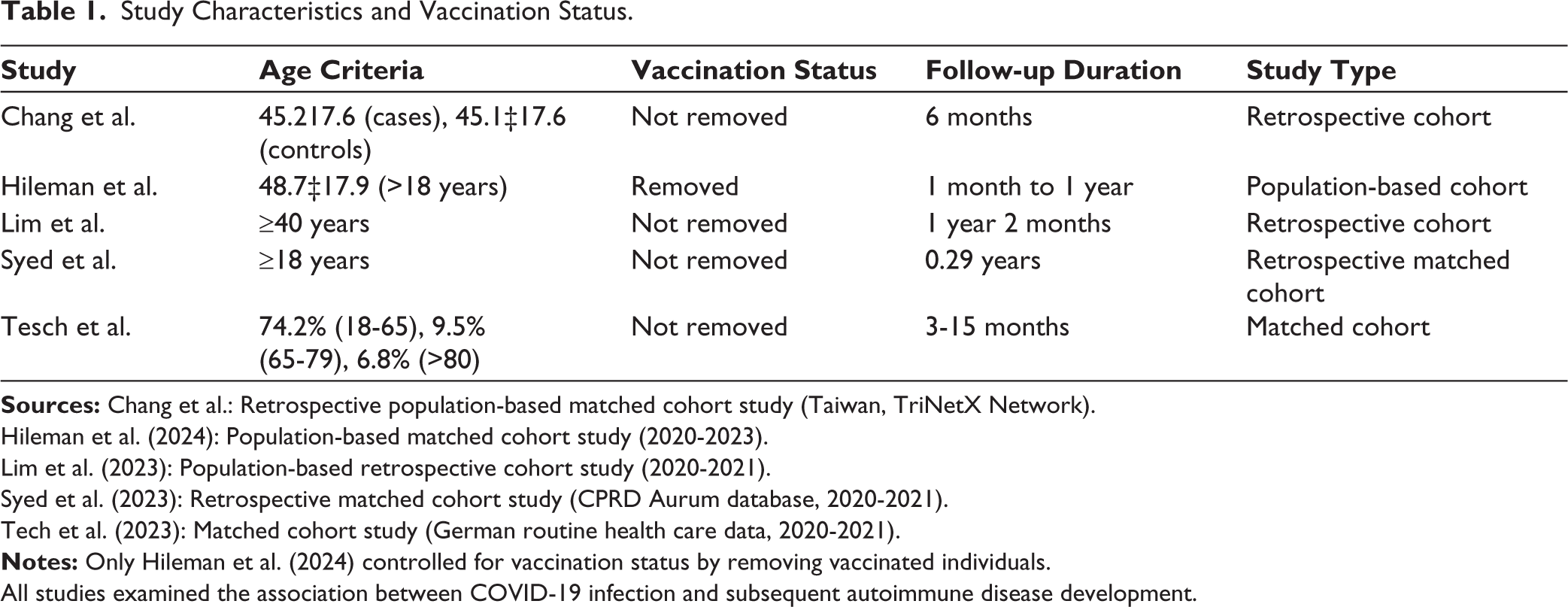
Hileman et al. (2024): Population-based matched cohort study (2020-2023).
Lim et al. (2023): Population-based retrospective cohort study (2020-2021).
Syed et al. (2023): Retrospective matched cohort study (CPRD Aurum database, 2020-2021).
Tech et al. (2023): Matched cohort study (German routine health care data, 2020-2021).
All studies examined the association between COVID-19 infection and subsequent autoimmune disease development.
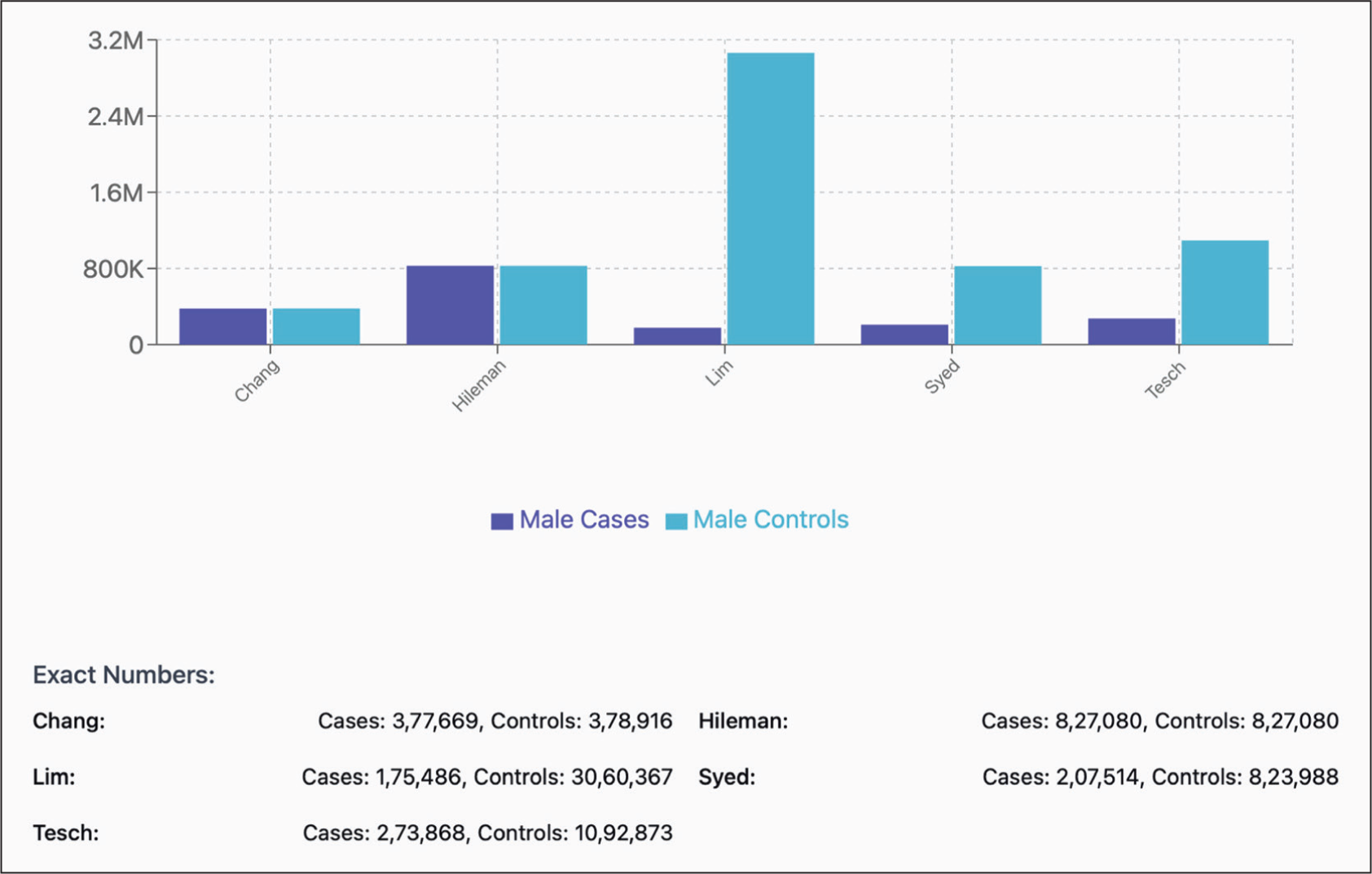
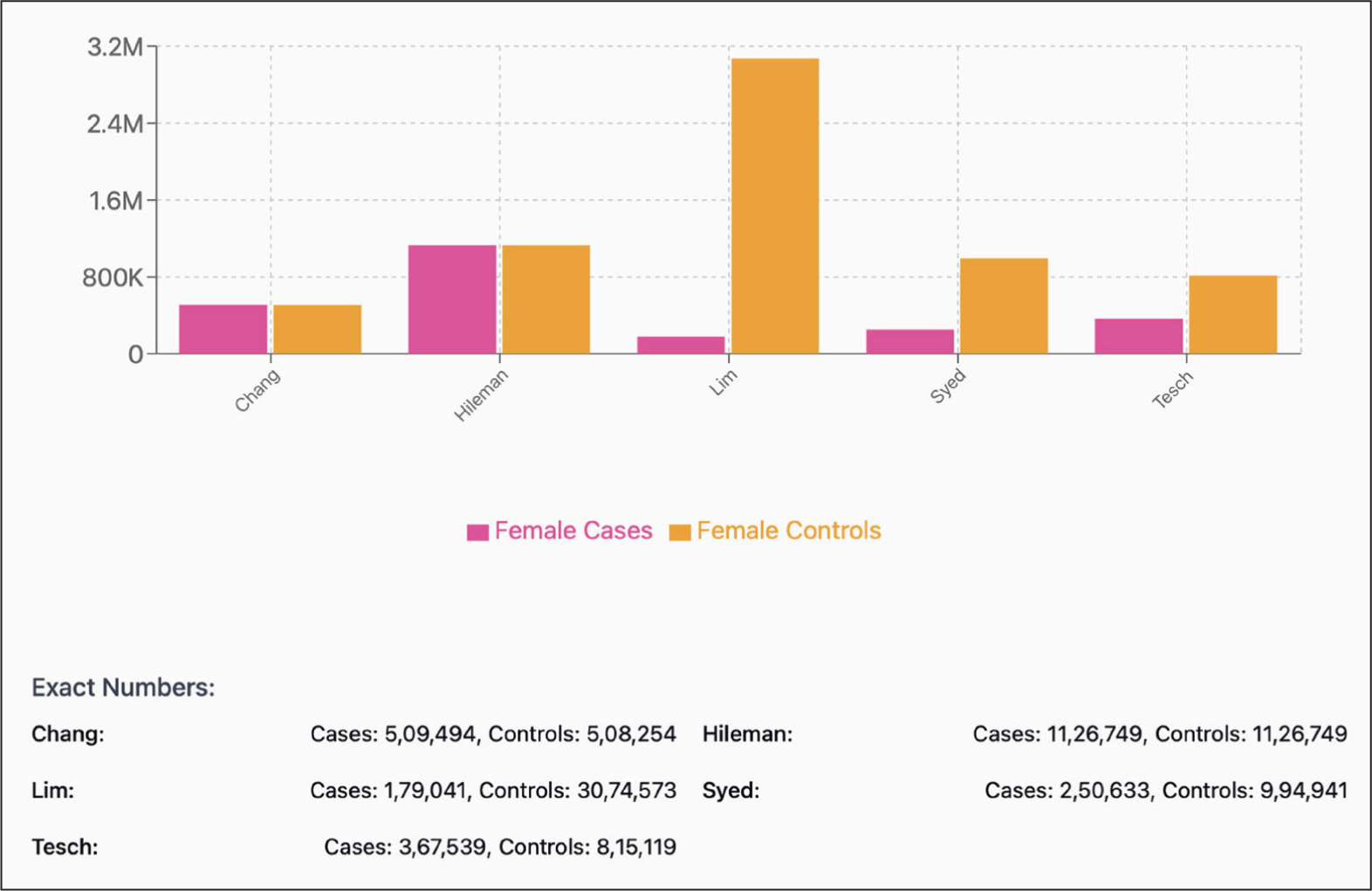
Population in the Study Groups.

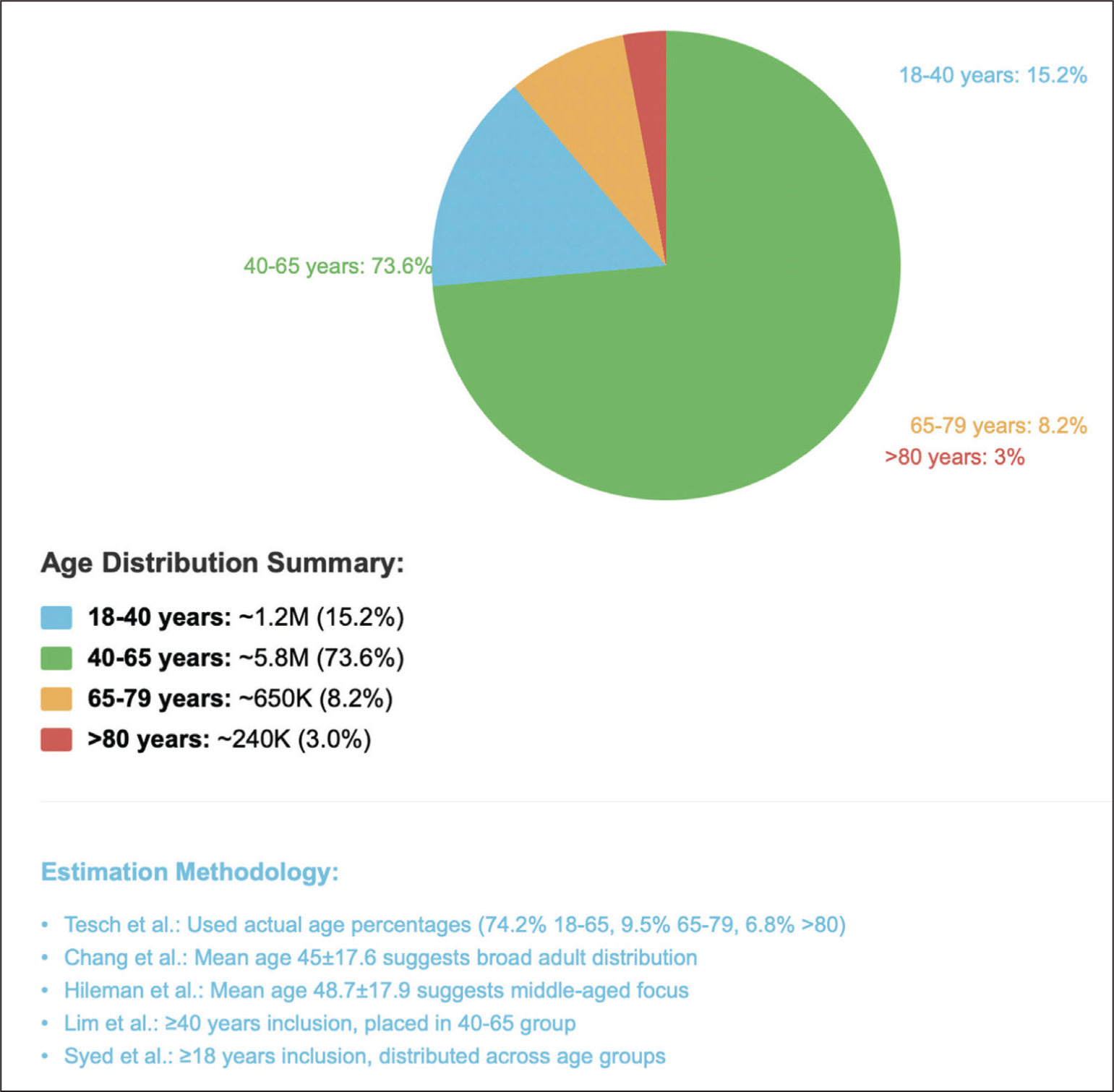
The study cohorts were well-matched for age and sex between the COVID-19 and control groups in all studies (Figures 2, 3 and 4). Adjustments for potential confounders such as comorbidities (e.g., hypertension or diabetes) and vaccination status were reported in most studies.
Male Participants Graphical Illustration.
Female Participants Graphical Illustration.
Age Distribution Across all Studies.
Meta-analysis Findings
Our meta-analysis found a significant association between COVID-19 and ANCA-associated vasculitis and type 1 diabetes. Diseases such as cutaneous vasculitis, MCTD, psoriasis and celiac disease showed elevated but non-significant risks, while inflammatory myopathies and adult-onset Still’s disease showed no association (Table 3 and Table 4).
Interpretation of Autoimmune Diseases.
Figures of the Forest Plot.
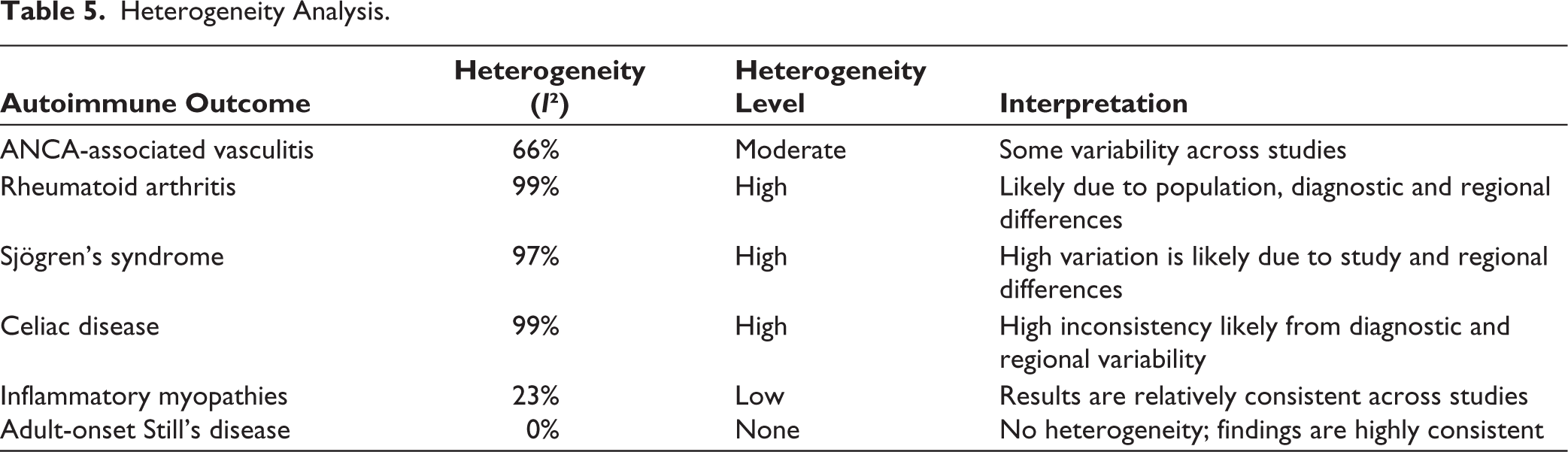
Heterogeneity Analysis
Heterogeneity (I2) varied widely across autoimmune outcomes (Table 5).
Heterogeneity Analysis.
Sensitivity Analysis
Sensitivity analysis confirmed the robustness of findings for ANCA-associated vasculitis and T1DM when individual studies were excluded from the meta-analysis or when fixed-effects models were applied.
Publication Bias
Funnel plots for outcomes such as ANCA-associated vasculitis and T1DM appeared symmetrical, suggesting no significant publication bias for these results based on Egger’s test (P > 0.05).
Discussion
Recent evidence highlights the existence of a bidirectional relationship between COVID-19 and autoimmune diseases. SARS-CoV-2 infection may trigger autoimmunity via molecular mimicry and immune dysregulation, increasing post-infection autoimmune disease risk (25%-42.6% higher within a year), while pre-existing autoimmune conditions heighten COVID-19 severity and impair vaccine responses, necessitating tailored clinical management. 14
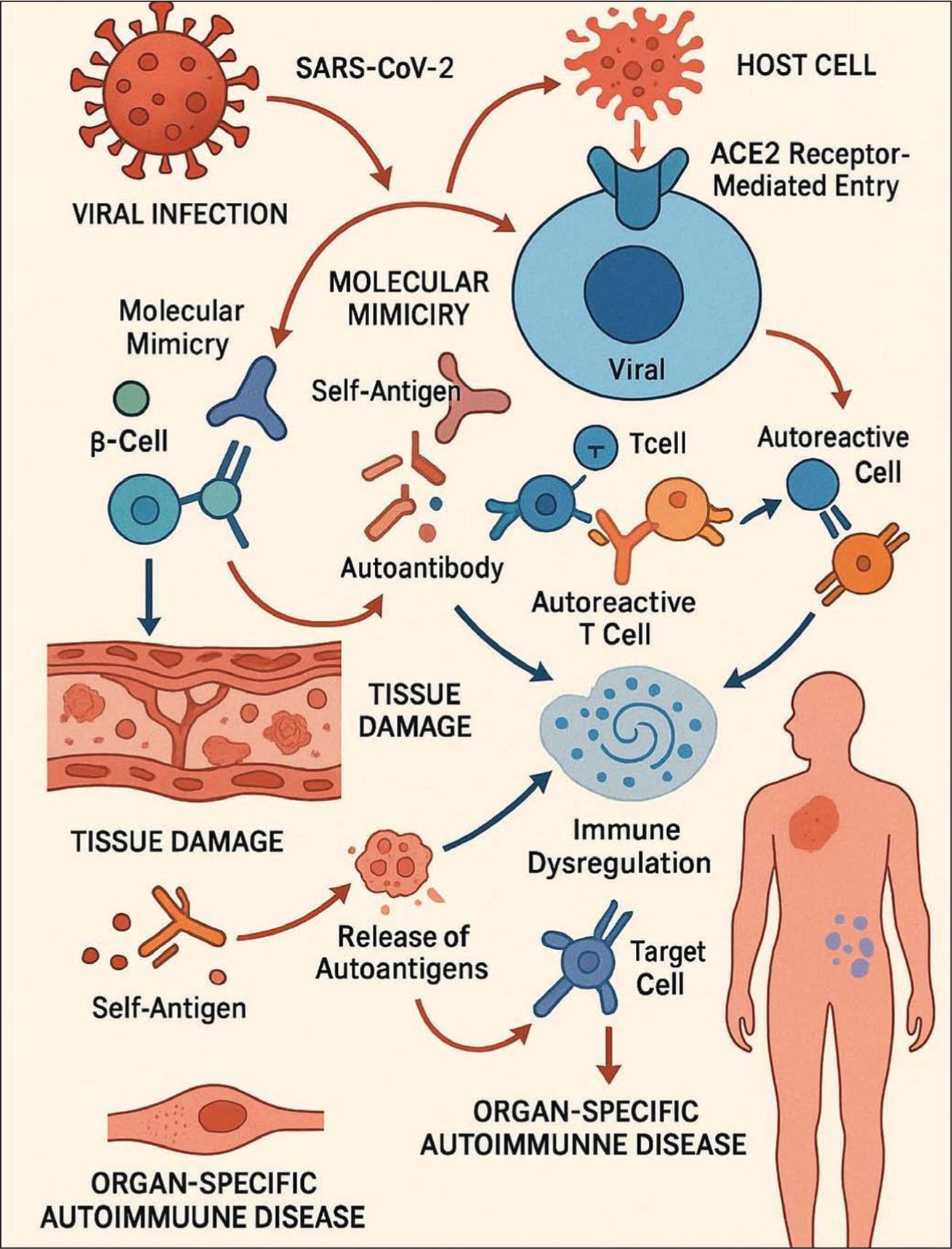
The pathogenesis of SARS-CoV-2 in the development of autoimmune diseases is complex and multifactorial. The virus possesses a large RNA genome with interrupted transcription, resulting in the production of a diverse array of viral epitopes. This increases the likelihood of molecular mimicry between viral and host peptides, potentially leading to the generation of cross-reactive autoantibodies. Similar to SARS-CoV, SARS-CoV-2 gains cellular entry via angiotensin-converting enzyme 2 (ACE2) receptor-mediated endocytosis. These receptors are widely distributed across multiple organ systems, including the blood vessels, heart, lungs, kidneys and intestines, allowing the virus to infect a broad range of cell types and potentially initiate organ-specific autoimmune responses.15,16 Moreover, the enhanced inflammatory response, often characterised as a cytokine storm, can independently promote the production of autoantibodies and contribute to tissue damage. 17 This tissue destruction further exacerbates immune dysregulation, facilitating the activation of autoreactive immune responses (Figure 5).
Mechanisms involved in Autoimmunity Induced by the COVID-19 Virus.
The clinical presentation of autoimmune-related manifestations in patients with COVID-19 spans a broad spectrum, ranging from organ-specific conditions to systemic autoimmune disorders. 3 Through this meta-analysis, we assessed the pooled risk of new-onset autoimmune conditions following SARS-CoV-2 infection from full-text English-language cohort studies published between 2019 and 2023 and the extracted data showed an increased risk of ANCA-associated vasculitis and type 1 diabetes after COVID-19.
The pathogenesis of vasculitis in the context of COVID-19 appears to be multifactorial. SARS-CoV-2 infection induces a profound pro-inflammatory state characterised by the release of cytokines such as IL-6, IL-1β and TNF-α, contributing to the development of a cytokine storm.18,19 This excessive immune activation can cause endothelial dysfunction and damage, a key event in the initiation of vasculitic processes. The virus can directly infect endothelial cells through ACE2 receptors, leading to endotheliitis and vascular inflammation. 20 In addition, COVID-19 may trigger autoimmune mechanisms through molecular mimicry, where viral antigens resemble self-antigens, prompting the development of autoantibodies and autoreactive T-cells. 21 Reports of COVID-19-associated vasculitis, including cutaneous leukocytoclastic vasculitis, Kawasaki-like disease in children (MIS-C) and ANCA-associated vasculitis, support the hypothesis of a virus-induced dysregulated immune response.22,23
Similarly, rising evidence has further strengthened the previously established link between viral infections and the onset of T1DM.24,25 One proposed mechanism is the direct invasion of pancreatic β-cells by SARS-CoV-2 via the ACE2 receptor, which is abundantly expressed on islet cells. This hypothesis is supported by findings from the Diabetes Virus Detection (DiViD) study, which demonstrated the presence of SARS-CoV-2 in pancreatic tissue through post-mortem analyses and in vitro experiments, highlighting the virus’s cytotoxic effect on β-cells. 26 In addition, the infection induces a systemic inflammatory response with elevated cytokines such as IL-6 and TNF-α, which may impair β-cell function and accelerate autoimmune destruction in genetically susceptible individuals.27,28 Molecular mimicry between viral antigens and β-cell proteins such as Glutamate decarboxylase 65 (GAD65s) also been proposed, potentially triggering cross-reactive T-cell responses and initiating or unmasking autoimmune diabetes. 15 These auto-antibodies were also further associated with prognosis and complications of the infection. 12
Conditions such as cutaneous vasculitis and MCTD appear to have potential risk associations with COVID-19; however, we require further studies to confirm these findings and understand their long-term effects. Conversely, our study found no increased risk for certain other autoimmune conditions, though the underlying mechanisms for this selective association remain unclear. Several study limitations may have contributed to these null findings, including an insufficient follow-up duration to capture delayed autoimmune manifestations and the inherently nonspecific symptomatology of some autoimmune diseases, which could lead to underdiagnosis or misclassification.
Among the included studies, only the study by Hileman et al. differentiated cohorts based on vaccination status. Notably, their study also offered unique insights into the increased risk of autoimmunity associated with the Delta variant, as their data collection spanned from June 2020 to June 2021, which corresponds with the peak of Delta variant transmission. However, the role of COVID-19 vaccination and its potential role in the development of autoimmune diseases still remains unclear and is yet to be established by evidence-based results.
Limitations
This systematic review has a few limitations. First, except for the Hileman et al. study, none of the included studies were able to stratify their populations based on vaccination status. This limitation prevents adequate differentiation between autoimmunity triggered by SARS-CoV-2 infection versus COVID-19 vaccination, which is crucial for understanding disease pathogenesis and establishing causality. Second, the prolonged latency period between COVID-19 infection and the development of clinically apparent autoimmune diseases poses a significant challenge in establishing temporal associations. Many autoimmune conditions require extended periods to manifest and the current follow-up duration in the included studies may be insufficient to capture the full spectrum of post-COVID autoimmune complications. Final, the limited statistical power of individual studies and the high heterogeneity observed across the included study groups restrict our ability to draw definitive conclusions. The variability in study designs, populations, diagnostic criteria and follow-up periods contributes to this heterogeneity, limiting the generalisability of the findings.
Conclusion
This meta-analysis demonstrates statistically significant associations between COVID-19 infection and increased risks of developing ANCA-associated vasculitis (HR = 1.93) and T1DM (HR = 1.66). While elevated hazard ratios are observed for cutaneous vasculitis (HR = 1.60) and MCTD (HR = 2.04), these associations did not reach statistical significance, potentially due to limited statistical power or high heterogeneity among studies. Conversely, null associations were identified for inflammatory myopathies (HR = 0.91) and adult-onset Still’s disease (HR = 1.00). These findings highlight the heterogeneous nature of COVID-19’s impact on the development of autoimmune diseases. The underlying mechanisms explaining why SARS-CoV-2 infection confers a significantly increased risk for certain autoimmune diseases while showing no association with others remain unclear and warrant further investigation.
Although these results should be interpreted with caution due to the study’s limitations, they provide essential evidence for the development of targeted clinical surveillance strategies. The demonstrated significant associations underscore the critical importance of closely monitoring patients for specific autoimmune manifestations following COVID-19 infection. Healthcare providers should implement tailored management approaches that prioritise vigilance for ANCA-associated vasculitis and T1DM in post-COVID patients, while maintaining awareness of potentially emerging risks for other autoimmune conditions.
Future research should focus on elucidating the pathophysiological mechanisms underlying these selective associations and conducting larger, more homogeneous studies to clarify the risk profiles for conditions currently showing non-significant trends.
Footnotes
Acknowledgements
I thank Dr Babu Mohan for his gracious help and assistance in providing direction for performing the meta-analysis. His expertise from his large number of first-author meta-analysis research projects and his guidance as a clinical educator have helped us complete this project successfully.
Authors’ Contribution
Vedantam, Deepanjali-Conceptualisation, investigation, writing-draft, review and editing. Gogula, Naga Sai Akhil Reddy-Methodology, writing-draft, review and editing. Nookala, Vinod-Formal analysis, methodology, writing-review and editing. Babu Mohan-Validation and supervision.
Conflicts of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Consent to Participate
N/A.
Consent for Publication
N/A.
Data Availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Declaration of Generative AI in Scientific Writing
None.
Ethical Considerations
N/A.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.