
Abstract
Background:
Systemic lupus erythematosus (SLE) is a chronic inflammatory autoimmune disease. Effective evaluation of activity indexes is very important in disease management. Serum amyloid A (SAA) is one of the acute-phase reactants. Serum albumin is a negative phase reactant protein; lower than normal levels have been frequently reported in SLE. Hypoalbuminemia is a consequence of the inflammatory process. This study is to evaluate the SAA-to-albumin ratio in SLE patients as a marker of activity.
Results:
This study was performed on 25 SLE patients and 25 matched healthy subjects, who underwent detailed history taking, clinical assessment and disease activity assessment using the SLE Disease Activity Index (SLEDAI). The SAA to serum albumin ratio was significantly increased in SLE patients compared to controls (P < .001). There was a significantly positive correlation between SAA-to-albumin ratio (SAA/ALB) and SLEDAI, complement (C)3 and 24-hrs urinary proteins (P < .05), while there was no significant correlation between SAA/ALB and ESR, CRP, C4 and Anti-dsDNA (P > .05).
Conclusions:
The SAA/ALB was associated with high disease activity in SLE patients. The SAA/ALB might be an indicator of increased disease activity in SLE.
List of Abbreviations
ACR: American College of Rheumatology
ALB: Albumin
ALT: Alanine transferase
ANA: Antinuclear antibody
AST: Aspartate transferase
AUC: Area under the curve
BMI: Body mass index
BUN: Blood urea nitrogen
C: Complement
CRP: C-reactive protein
ds DNA: double-stranded deoxyribonucleic acid
eGFR: Estimated glomerular filtration rate
ELISA: Enzyme-linked immunosorbent assay
ESR: Erythrocyte sedimentation rate
EULAR: European League Against Rheumatism
IL: Interleukin
IQR: Interquartile range
ROC: Receiver operating characteristic
SAA: Serum amyloid A
SD: Standard deviation
SLE: Systemic lupus erythematosus
SLEDAI: Systemic Lupus Erythematosus Disease Activity
TNF: Tumour necrosis factor
Background
Systemic lupus erythematosus (SLE) is a chronic autoimmune disorder characterised by a breakdown in immune tolerance, the production of autoantibodies, and the formation and deposition of immune complexes. These processes drive inflammation and lead to multisystem organ damage. 1 The clinical presentation of SLE is highly heterogeneous, ranging from mild mucocutaneous involvement to severe and potentially life-threatening complications affecting the kidneys, central nervous system, cardiovascular system, and haematologic system. 2 The disease typically follows a relapsing-remitting course, where periods of exacerbation and remission contribute to cumulative, and often irreversible, organ damage over time if inadequately controlled. 3
Timely and accurate assessment of disease activity is essential for guiding therapeutic decisions, preventing long-term complications, and improving prognosis in patients with SLE. Currently, clinical evaluation is supplemented by laboratory markers such as anti-dsDNA antibodies, complement (C) 3, C4, erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). However, these biomarkers have limited sensitivity and specificity, and may not consistently reflect disease activity, especially in cases of renal or neuropsychiatric involvement.4,5 Consequently, there remains an unmet need for novel, accessible, and reliable biomarkers that can provide real-time insights into systemic inflammation and disease activity in SLE.
Serum amyloid A (SAA) is a highly sensitive acute-phase reactant synthesised primarily by hepatocytes in response to pro-inflammatory cytokines such as interleukin (IL) 1, IL 6, and tumour necrosis factor (TNF)α. Elevated SAA levels have been observed in numerous inflammatory and autoimmune conditions, including rheumatoid arthritis, familial Mediterranean fever, and systemic infections.6,7 In SLE, elevated SAA has been associated with active disease, particularly during flares and in cases of renal involvement. 8
In contrast, serum albumin is a negative acute-phase reactant. Its levels decline during inflammation due to decreased hepatic synthesis, increased catabolism, or loss through renal and gastrointestinal pathways. Hypoalbuminemia in SLE has been linked to active disease and poor clinical outcomes, especially in patients with lupus nephritis, serositis, or protein-losing enteropathy. 9
The SAA-to-albumin ratio (SAA/ALB) has recently emerged as a novel composite biomarker that integrates both inflammatory response and hepatic synthetic function. This ratio has demonstrated diagnostic and prognostic value in various pathological settings, including cardiovascular diseases, malignancies, and sepsis.10,11 Unlike single inflammatory markers or complete blood count-derived ratios, the SAA/ALB ratio utilises a positive acute-phase reactant and a negative acute-phase protein, potentially reflecting the balance between systemic inflammation and hepatic response, which gives a complementary role to the traditional SLE activity indices.
Accordingly, the present study was designed to evaluate the clinical significance of SAA, serum albumin, and the SAA/ALB ratio in patients with SLE. We aimed to investigate their associations with clinical manifestations, disease activity indices, and conventional laboratory parameters, and to explore their value in routine clinical settings.
Patient and Methods
This cross-sectional comparative study included 25 patients fulfilling the 2019 European League Against Rheumatism (EULAR)/American College of Rheumatology (ACR) classification criteria for SLE, 12 and 25 age and sex matched healthy individuals served as the control group. Sample size was calculated using the PASSA 11 programme for sample size calculation, setting power at 80%, alpha error at 5%, and ratio at 1. A sample size of at least 50 participants (25 patients with SLE and 25 healthy controls) can detect an expected area under the ROC curve of 0.733 for the predictive ability of the SAA/ALB ratio for the activity of SLE.
Ethical approval for the study was obtained from the local Research Ethics Committee. This study has been approved by the Research Ethics Committee of the Faculty of Medicine, Ain Shams University, and received formal approval on 28 November 2023. The approval number is FMASU MS 705/2023. The study procedure was explained to all participants. Written informed consent was obtained from all the participants prior to their enrollment in the study.
Exclusion criteria of the study included patients with significant renal impairment (defined as eGFR < 60 mL/min/1.73 m²) or hepatic dysfunction (defined as ALT or AST > 3 times the upper limit of normal or known chronic liver disease). Also, patients with overlapping autoimmune disease, pregnancy, and malignancy were excluded from our work. Patients were excluded from the study.
Detailed clinical evaluations were performed for all patients, including documentation of demographic characteristics, clinical manifestations, and current medications. Disease activity was assessed using the SLE Disease Activity Index (SLEDAI-2K). 13 It includes 24 weighted objective clinical and laboratory variables, and it measures disease activity within the last 10 days. The score can be between 0 and 105. Regarding SLE disease activity of our included SLE patients, SLEDAI ≤6 was denoted as mild, SLEDAI from 7 to 12 was denoted as moderate, and SLEDAI >12 was denoted as severe disease activity. 4
Study Procedure
Venous blood samples were taken under sterile conditions and collected in dry tubes containing no anticoagulant for serum separation. All samples were allowed to clot for 10–20 minutes at room temperature and then were centrifuged at approximately 2000–3000 RPM for 20 minutes. Samples were used within 5 days and stored at 2°C-8°C. SAA levels were measured using a commercial sandwich ELISA kit (Human SAA ELISA Kit, Elabscience, USA) according to the manufacturer’s instructions. Serum albumin concentrations were measured using the bromocresol green colourimetric method with automated biochemical analysers, while the SAA/ALB ratio was calculated by dividing the SAA value (mg/L) by the serum albumin level (g/dL).
Statical Analysis
Data were fed to the computer and analysed using IBM SPSS software package version 25.0 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp). Qualitative data were described using numbers and percentages. The Shapiro-Wilk test was used to verify the normality of the distribution. Quantitative data were described using range (minimum and maximum), mean, standard deviation, median and interquartile range (IQR). Student’s t-test was used to analyse parametric data between two groups. Chi-square test was used to compare nominal categorical data. The Mann-Whitney U-test was used to analyse nonparametric data between two groups. The Spearman’s rho method was used to analyse the correlation between two quantitative variables. The linear relationship between two variables was determined by the correlation coefficient, represented symbolically by the letter ‘r’. P values from correlation analyses (n = 27) were adjusted using the Benjamini-Hochberg false discovery rate method. The sensitivity and specificity were assessed using the receiver operating characteristic (ROC) curve. P value is the significance level; a P value of <.05 was regarded as significant. Comparative linear regression models were built to observe if the ratio offered better predictive value than each of its components alone.
Results
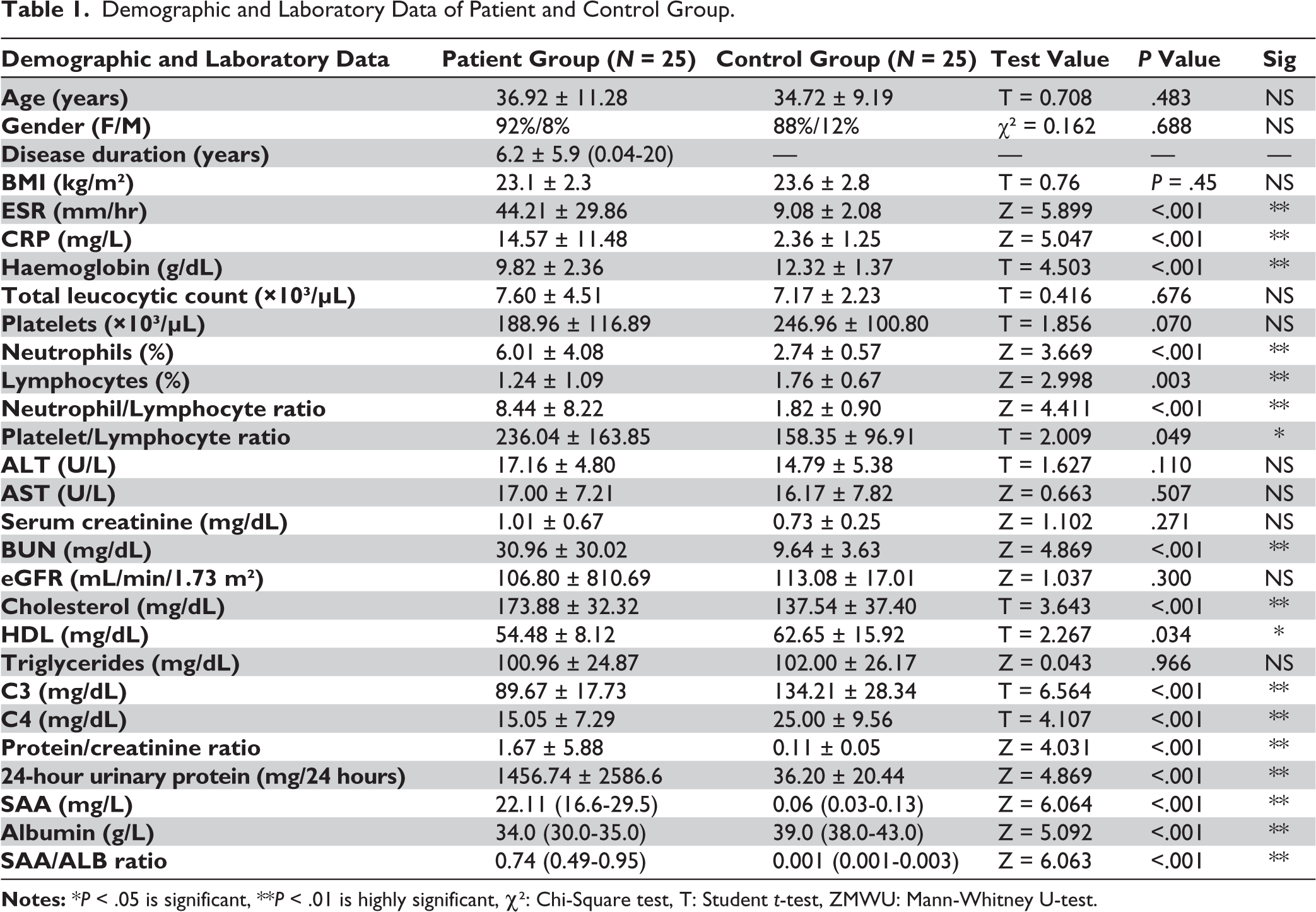
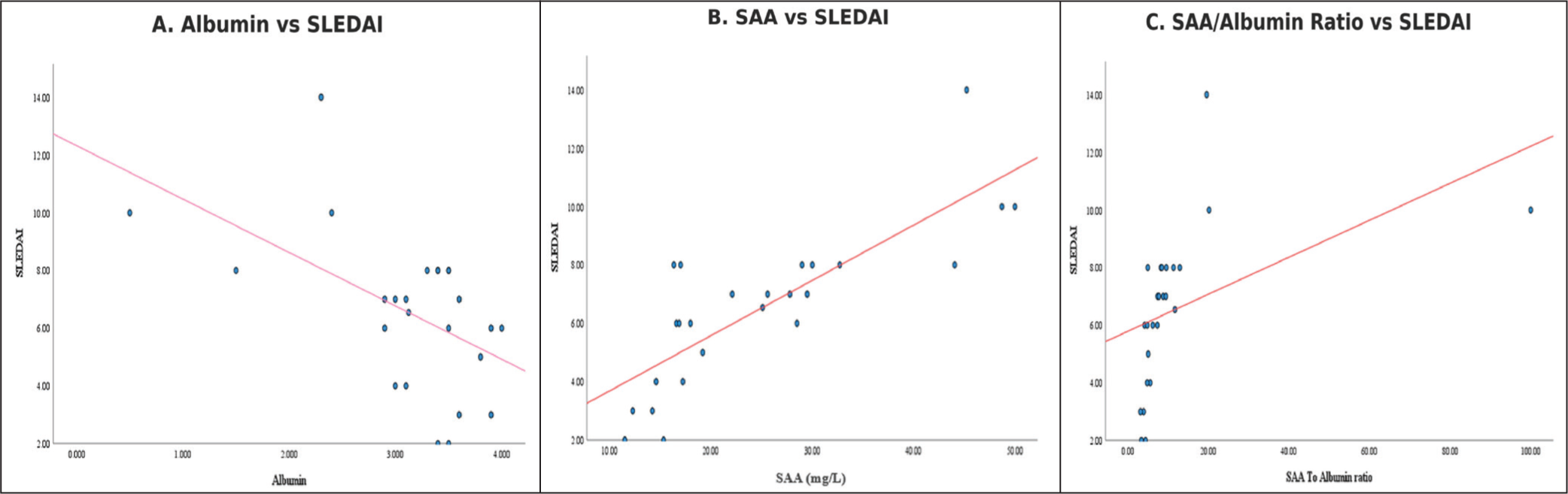
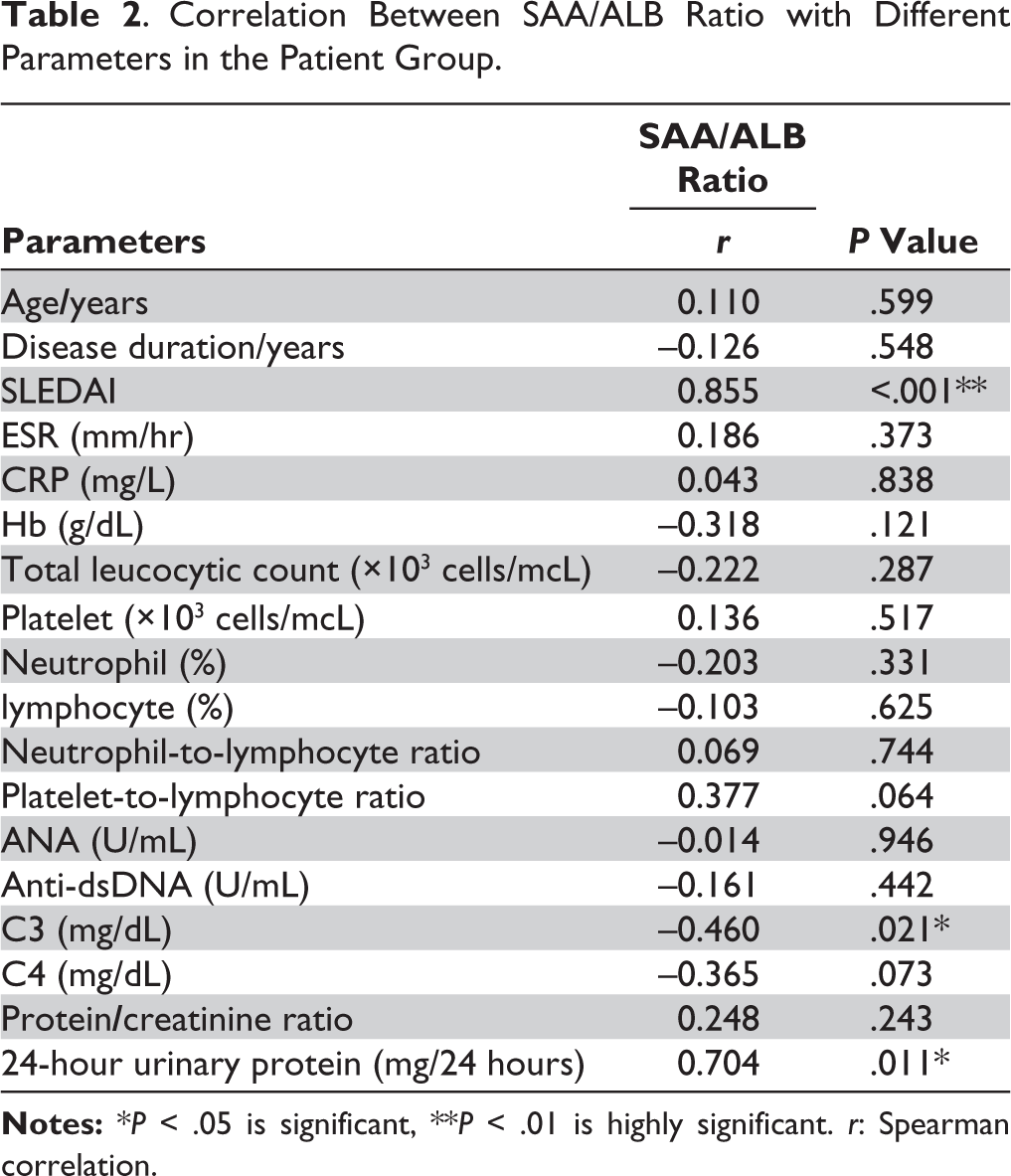
The study included 25 SLE patients and 25 age and sex matched healthy individuals who served as the control group. Among the SLE patients, 92% were females and 8% were males, with a mean age of 36.92 ± 11.28 years, and a body mass index (BMI) of 23.1 ± 2.2 kg/m². The mean disease duration was 6.2 ± 5.9 years. In the control group, 88% were females and 12% were males, with a mean age of 34.72 ± 9.19 years and BMI of 23.6 ± 2.8 kg/m². BMI did not differ significantly between the two groups (23.1 ± 2.2 kg/m² vs. 23.6 ± 2.8 kg/m²; t = −0.76, P = .45). There was no statistically significant difference between the two groups in terms of age, gender or BMI (P > .05). Disease activity was assessed by SLEDAI, which ranged from 2 to 14 with a mean of 6.5 ± 5.9. Twenty eight percent of patients had mild activity, 68% had moderate activity, while one patient had severe activity. Regarding organ system involvement, the domains involved in our SLE patients were haematologic, renal, mucocutaneous, serosal, musculoskeletal, constitutional, and neuropsychiatric systems. The most frequently observed clinical manifestation among SLE patients was thrombocytopenia (44%) (<100 × 109 /L), followed by proteinuria (28%), rash (28%), arthritis (24%), and alopecia (24%). Other clinical features included oral ulcers (20%), urinary casts (20%), leukopenia (16%), haematuria (16%), pleural effusion (16%), pericarditis (12%), fever (12%), seizures (12%), psychosis (8%), and organic brain insult (4%). The demographic and laboratory results of SLE patients and their corresponding control group are displayed in Table 1. SAA levels and SAA/ALB were significantly increased in SLE patients compared to the healthy control group, with median values of 22.11 (16.6–29.5) mg/L and 0.74 (0.49–0.95) mg/L, respectively. In contrast, albumin levels were significantly lower in SLE patients, with a median value of 34.0 (30.0–35.0) g/L (P < .001). A significant positive correlation was observed between SAA and the SLEDAI score (r = 0.818, P < .001). In contrast, SAA showed a significant negative correlation with C3 (r = –0.531, P = .006) and C4 (r = –0.472, P = .01) (Figure 1). No significant correlation was found between SAA and other laboratory parameters, including ESR, CRP, haemoglobin, total leukocyte count, platelet count, neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, ANA, anti-dsDNA, protein/creatinine ratio, 24-hour urinary protein, and serum albumin (P > .05). Serum albumin levels were significantly and negatively correlated with the platelet-to-lymphocyte ratio (r = –0.587, P = .002) and SLEDAI (r = –0.506, P = .010). However, no significant correlations were found between serum albumin and ESR, CRP, haemoglobin, total leukocyte count, platelet count, ANA, anti-dsDNA, complement components (C3 and C4), protein/creatinine ratio, 24-hour urinary protein, or SAA (P > .05). SAA/ALB showed a significant negative correlation with C3) r = –0.460, P = .021 and a significant positive correlation with SLEDAI (r = 0.855, P < .001), 24 hours urinary protein (r = 0.704, P = .011) (Table 2).
Demographic and Laboratory Data of Patient and Control Group.
Correlation of SAA, Serum Albumin and SAA/ALB Ratio with SLEDAI.
Correlation Between SAA/ALB Ratio with Different Parameters in the Patient Group.
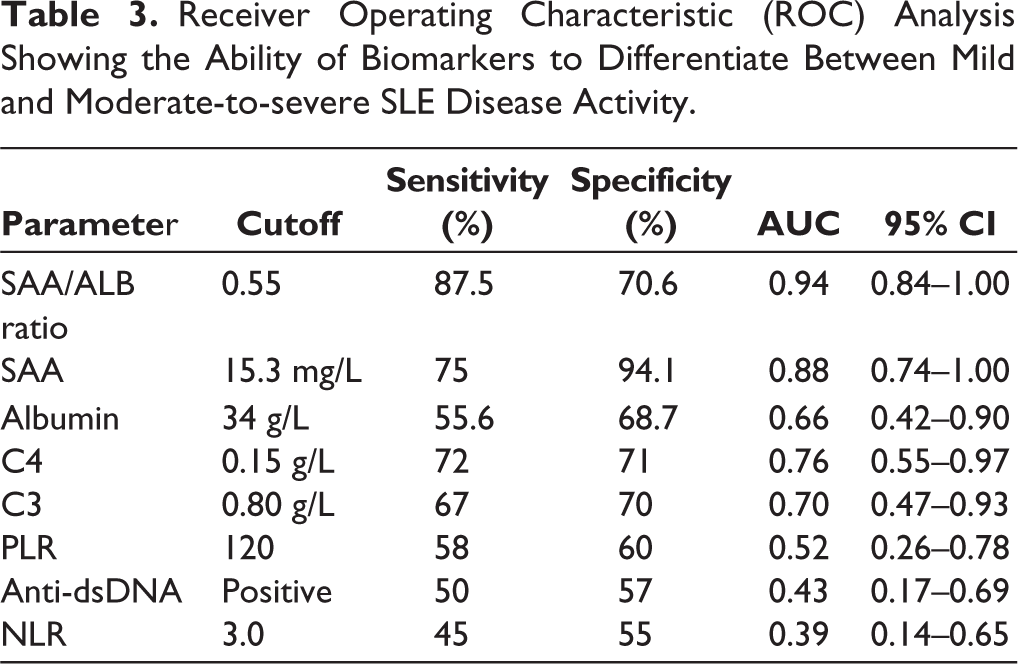
ROC analysis was performed to evaluate the ability of biomarkers to differentiate mild disease from moderate-to-severe disease activity (SLEDAI ≥ 6). The SAA/ALB ratio demonstrated the highest diagnostic performance at a cutoff value of 0.55. SAA also showed good diagnostic ability at a cutoff of 15.3 mg/L. Conventional biomarkers such as PLR, anti-dsDNA, and NLR showed lower diagnostic ability (Table 3).
Receiver Operating Characteristic (ROC) Analysis Showing the Ability of Biomarkers to Differentiate Between Mild and Moderate-to-severe SLE Disease Activity.
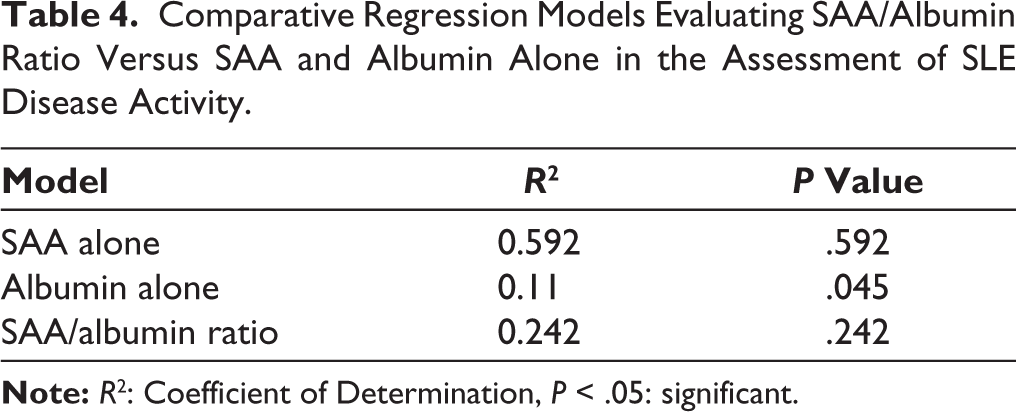
Comparative multivariable logistic regression models were used to evaluate the explanatory power of the SAA/albumin ratio versus its individual components. SAA/albumin ratio demonstrated the best performance (P < .05) (Table 4).
Comparative Regression Models Evaluating SAA/Albumin Ratio Versus SAA and Albumin Alone in the Assessment of SLE Disease Activity.
Discussion
The findings of this study support the clinical relevance of SAA, serum albumin, and SAA/ALB as valuable biomarkers in assessing disease activity in patients with SLE. Elevated levels of SAA and the SAA/ALB ratio were significantly associated with increased SLEDAI scores, reinforcing their potential as indicators of active disease. These results are consistent with prior studies,6,8 which highlighted the responsiveness of SAA as an acute-phase reactant in autoimmune inflammation. Zhao and his colleagues previously evaluated the SAA/ALB ratio in Chinese SLE patients. 6 Disease susceptibility, clinical manifestations, severity, and immunological profiles may vary across different racial populations. 14 Therefore, assessment of this biomarker in a different ethnic group enhances its potential clinical utility. The effectiveness of SAA in reflecting disease activity may be attributed to its rapid hepatic induction by pro-inflammatory cytokines such as IL-1, IL-6, and TNF-α, which are known to be elevated during disease flares in SLE. 3
Furthermore, the hypoalbuminemia observed in this study emphasises the role of albumin as a negative acute-phase protein. Albumin levels showed significant inverse correlations with disease activity and inflammatory markers. These observations are consistent with previous findings,9,5 where decreased albumin levels were associated with systemic inflammation in active SLE. Renal protein loss due to lupus nephritis could be linked to hypoalbuminemia. However, due to the cross-sectional design of our research, reduced albumin alone cannot distinguish between these mechanisms.
SAA/ALB ratio appears to integrate the strengths of both biomarkers, providing a clue for capturing active inflammation. This ratio demonstrated strong correlations with clinical and laboratory parameters, including 24-hour urinary protein, indicating possible renal involvement. These findings align with earlier evidence7,11 supporting the utility of SAA-derived ratios in evaluating disease activity, particularly in lupus nephritis. The ratio reflects not only systemic inflammation but also its potential renal consequences. The SAA/ALB ratio could be considered a marker associated with renal involvement rather than a definitive indicator. Albumin drop accounts for the negative acute-phase response of albumin due to renal loss or hepatic suppression, while SAA rises due to systemic cytokine production (IL-1, IL-6). 15
The significant correlation between the SAA/ALB ratio and C3, but not C4, could be because C3 is a central component of all pathways, while C4 is primarily linked to the classical pathway; C3 often serves as a more sensitive marker of overall consumption or production. Also, C3 is synthesised during acute-phase responses in higher quantities than C4. Many SLE patients have low baseline C4 due to ‘null alleles’, which makes it a less reliable marker of current inflammation than C3. 16
Unlike ESR and CRP, which did not show significant correlation with disease activity in our study, SAA and SAA/ALB ratio provided more reliable and clinically informative results. Previous studies suggested that ESR and CRP have low sensitivity for mucocutaneous and even some vascular flares.1,5 It is well documented that CRP remains low despite active disease. SAA is known to be a more sensitive acute-phase reactant than CRP in SLE. 17 Furthermore, ESR is a slow-reacting marker influenced by plasma viscosity and anaemia, whereas the SAA/ALB ratio provides a more dynamic indicator of current metabolic and inflammatory status, making it a sensitive marker complementary to traditional clinical indices reflecting more intense systemic inflammation and could assist in stratifying severity. 18
ROC curve analysis further confirmed the diagnostic value of both SAA and SAA/ALB ratio, showing high sensitivity and specificity in distinguishing between mild and moderate-to-severe disease. SAA/ALB ratio reflects systemic inflammatory burden. The ratio is shown to have better explanatory power for SLEDAI than its components alone. This proves the ratio is a superior marker than each test alone.
These results advocate for the clinical adoption of these markers for the diagnosis of disease flares. Consistent with earlier studies,7,11 the incorporation of SAA-based ratios into routine practice may enhance the detection of activity and treatment adjustments.
Although the SLEDAI remains the gold standard for assessing disease activity, it requires a comprehensive clinical and laboratory evaluation. By contrast, the SAA/ALB ratio is a simple, blood-based biomarker that could serve as a practical adjunct or even a surrogate marker, particularly in outpatient settings or resource-limited areas. 2
In summary, our findings suggest that the SAA/ALB ratio is a sensitive, practical, and informative marker of disease activity in SLE. It outperforms traditional inflammatory markers and correlates well with both systemic manifestations and renal involvement, offering significant promise for use in clinical practice.
Study Limitations
Future longitudinal studies are recommended, specifically designed to assess predictive value for flares or treatment response. The relatively small sample size represents a limitation of this study. A larger number of patients could help to adjust for confounding factors. Larger prospective and multi-centre studies are recommended to establish its place in the clinical management algorithms of SLE. Comparative studies evaluating SAA/ALB against other emerging biomarkers (e.g., IL-6 and Type I interferon signatures) and histopathological renal involvement may help determine its relative utility and specificity in assessing SLE activity.
Conclusions
The findings of this study demonstrate that the SAA/ALB ratio is significantly associated with disease activity in patients with SLE. This ratio correlates strongly with the SLEDAI score and shows superior diagnostic performance compared to SAA or albumin alone. As an available and inexpensive laboratory parameter. SAA/ALB ratio may serve as a valuable adjunctive biomarker for evaluating disease activity and guiding clinical decision-making in SLE. Further prospective studies with larger cohorts are recommended.
Footnotes
Acknowledgements
The authors thank the individuals who participated in this study.
Data Availability Statement
The datasets generated and/or analysed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the Research Review Board of the Faculty of Medicine, Ain Shams University, Cairo, Egypt (approval no. MS 705/2023).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent was obtained from all participants prior to their inclusion in the study.