
Abstract
Background:
Fibromyalgia (FM) is a rheumatic illness that is characterised by widespread chronic pain, fatigue and psychiatric disorders, including depression and bipolar disorders, which may occur concomitantly with FM.
Aim of the Work:
To evaluate the frequency of bipolar disorder types in FM patients and to assess the impact of their types on the functional status.
Patients and Methods:
This study enrolled 55 female patients with FM and 55 age and sex-matched controls. Functional status was evaluated using the Fibromyalgia Impact Questionnaire (FIQ). All participants were assessed for psychiatric disorders using the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I), the Hamilton Depression rating scale (HDRS), the Young Mania Rating Scale (YMRS) and the Hypomania Symptom Checklist (HCL-32).
Results:
Bipolar disorder II was diagnosed in 12.7% of FM patients but in none of the control group. According to SCID-I, irritability as a symptom of a hypomanic episode was more frequent in FM (n = 39, 70.9%) patients versus two (3.6%) controls (P < .0001). Dysthymic disorder symptoms were reported only in FM (n = 21, 38.1%). Only one FM patient reported delusions and psychotic symptoms. Depression was diagnosed with 78.2% of FM patients, compared to 7.3% of controls (P < .0001). Hypomanic symptoms were present in 72.7% of FM patients and in 3.2% controls only (P < .0001). There was a significant correlation between the FIQ and mood disorders and hypomania (P < .0001, P < .02).
Conclusion:
Bipolar disorder II is more frequent in FM patients than in healthy controls, contributing to the exacerbation of the disease symptoms and increased functional impairment.
Introduction
Fibromyalgia (FM) is a complex syndrome characterised by chronic musculoskeletal pain, often accompanied by persistent fatigue, sleep disturbances, anxiety, depression and cognitive dysfunction. 1 The aetiology of FM remains unclear, but is widely influenced by a combination of genetic, environmental and psychological factors. 2 Stressful life events are believed to play a crucial role in the onset and progression of FM. 3 The pathogenesis of FM involves alterations in brain signals, including central sensitisation. 4 Dysfunction of inhibitory signals and abnormalities in the level of neurotransmitters are another mechanism of pain augmentation. 5 Cytokines may play a role in its pathogenesis; IL6 and IL8 were found to be higher in patients with FM. 6 The journey of the FM patient is often complicated with other comorbidities, rendering their quality of life markedly impaired. 7 FM is frequently associated with a high prevalence of psychiatric disorders, particularly major depressive episodes and panic disorders. 8
Bipolar disorder is a severe mental health condition characterised by extreme mood swings, including manic, hypomanic and depressive episodes. 9 Patients with bipolar disorders often experience significant challenges, such as a high suicide rate, sleep disturbances and disruptions in psychological traits such as self-esteem. 10 FM patients may experience both major depression and bipolar disorders, often accompanied by hypomanic symptoms. 11 These psychiatric conditions further complicate FM, as associated mood instability can exacerbate the physical symptoms and functional impairment. 12
The key connection and overlap between FM and depression is deeply rooted and bidirectional. Both share common pathophysiological mechanisms, including central sensitisation, low serotonin and norepinephrine and alteration of the hypothalamic pituitary adrenal axis. Polymorphism in the serotonin transporter (5-HTT) gene is involved in both major depressive disorder and FM. 1 The bidirectional relationship is frequently observed in both diseases; chronic pain from FM can cause depression, and depression can also increase the risk of developing FM. 13 They also share common therapeutic approaches; antidepressants, cognitive behavioural therapy and lifestyle changes are usually advised for both conditions. 1
Managing FM, particularly in patients with co-occurring bipolar disorders, requires a nuanced approach. 13 The use of antidepressants to control pain in FM patients must be approached with caution in the presence of concomitant bipolar disorder. Antidepressants can precipitate a manic episode in an undiagnosed bipolar disorder 14 ; thus, if bipolar disorder is suspected in a FM patient, it should be combined with mood stabilisers to prevent the induction of manic episodes or mood instability. Although patients with bipolar disorder II may respond to low-dose antidepressant monotherapy, they must be closely monitored. 15 Alternatively, gabapentin and pregabalin are effective options for treating both FM and bipolar disorder symptoms, but these should be used in conjunction with well-established mood stabilisers. 16
Given the high prevalence of psychiatric comorbidities in FM patients and the complexities involved in their treatment, this study was designed to evaluate the frequency of bipolar disorders in FM patients and to assess the impact of their types on the functional status. Determining the burden of bipolar disorder in fibromyalgia patients may improve diagnostic accuracy, guide safer pharmacologic strategies, support interdisciplinary management and ultimately reduce disability and healthcare utilisation in this complex patient group.
Patients and Methods
The study included 55 FM patients diagnosed according to the 2016 American College of Rheumatology criteria 17 and 55 age- and sex-matched healthy controls. Patients were recruited from the outpatient clinic of the Rheumatology Department between June 2023 and December 2023. The patients were evaluated by a rheumatologist for confirmation of diagnosis and functional scoring, then by a psychiatrist for evaluation of mood disorders, presence of manic/hypomanic disorders and the severity of depression. Patients with severe and uncontrolled medical illnesses, autoimmune disease, neurological disorders, drug abuse and those who received electroconvulsive therapy, psychotropic medications (amitriptyline, selective serotonin reuptake inhibitors) and serotonin-norepinephrine reuptake inhibitors and any other antidepressants in the 6 weeks before the study were excluded. All subjects provided written informed consent. The research was approved by the Ethical Committee of Cairo University Hospitals (MS-15-2023) on 11 November 2023. We calculated the sample size based on the hypothesis stating that the prevalence of bipolar disorder (BD) is significantly higher in FM patients (~ 20%) compared to a prevalence of around 1% in the general population. We used a two-sample proportions test with a power 90% and a significance level of 5%.
Clinical and socio-demographic data were collected, a full history was taken, and a clinical examination was performed. The functional status of FM patients was assessed using the Arabic version of the Fibromyalgia Impact Questionnaire (FIQ). 18 The FIQ consists of 10 questions. The first question includes 11 items related to physical functioning, each rated on a four-point Likert scale. Items 2 and 3 inquire about the number of days the patient felt well and the number of days they were unable to work due to FM symptoms. Items four through 10 are visual analogue scales where the patient rates work difficulty, pain, fatigue, morning tiredness, stiffness, anxiety and depression. Higher scores indicate greater dysfunction.
All FM patients and control participants were assessed for psychiatric disorders using the Structured Clinical Interview for DSM-IV-TR Axis I Disorders (SCID-I), Hamilton Depression Rating Scale (HDRS), Young Mania Rating Scale (YMRS) and Hypomania Symptom Checklist (HCL-32) questionnaires.
Psychiatric disorder assessment involves a structured evaluation of an individual’s mental health to diagnose potential psychiatric conditions. This process includes interviews, observation and standardised tests to gather information.
SCID-I: Lifetime psychiatric diagnosis of psychiatric and mood disorders was made using the SCID-I (mood disorders module). 19 The SCID-I was used to provide a comprehensive diagnostic profile or rule out psychiatric disorders according to DSM-IV criteria. Individuals diagnosed with mood disorders were further evaluated for bipolar spectrum disorder. The SCID-I provides a categorical diagnosis as the psychiatrist records whether the criteria for each disorder are met.
The following related scales were assessed: HDRS 20 is a widely used tool to measure the severity of depression over the past week, and higher scores indicate more severe symptoms. YMRS 21 assesses the severity of manic episodes and measures manic symptoms, including irritability, speech patterns and thought processes. Higher scores indicate severity. HCL-32 is self-administered, consisting of 32 items used to identify symptoms of hypomania and the Arabic version was used. 22 Higher scores also indicate the likelihood of bipolar disorder.
Psychiatric diagnoses were established using the Structured Clinical Interview for DSM, which served as the gold standard for diagnostic classification. Screening instruments for mood disorders were administered only as preliminary tools to identify the presence of depressive and hypomanic symptoms.
Statistical Analysis
It was done using the Statistical Package for the Social Sciences, version 28. Comparisons were performed using the chi-square, the Wilcoxon test or analysis of variance. Correlations were performed with Pearson’s and Spearman’s correlation. Regression analysis was done. P ≤ .05 indicated significance. Receiver operating characteristic (ROC) curve analysis was used to measure sensitivity and specificity.
Results
The current study included 55 female FM patients and 55 healthy female controls. The mean age of the FM patients was 34.3 ± 8.1 years, and for the control group was 34.49 ± 7.47 years. The BMI index was 26.7 ± 4.6 and for controls was 26.1 ± 3.55. The characteristics of the patients are presented in Table 1. According to SCID-I, mood disorder symptoms, including those associated with hypomanic episodes, showed highly statistically significant differences between FM patients and controls, with all P values being <.0001. Irritability was more frequent in FM patients (n = 39, 70.9%) versus two controls (3.6%) (P < .0001). Dysthymia (milder, yet longer-lasting form of major depression) 19 was present in FM (n = 21, 38.1%) and in none of the controls. One patient reported delusions and psychotic symptoms, and eight (14.5%) had suicidal ideation.
Characteristics of the Female FM Patients and Controls.
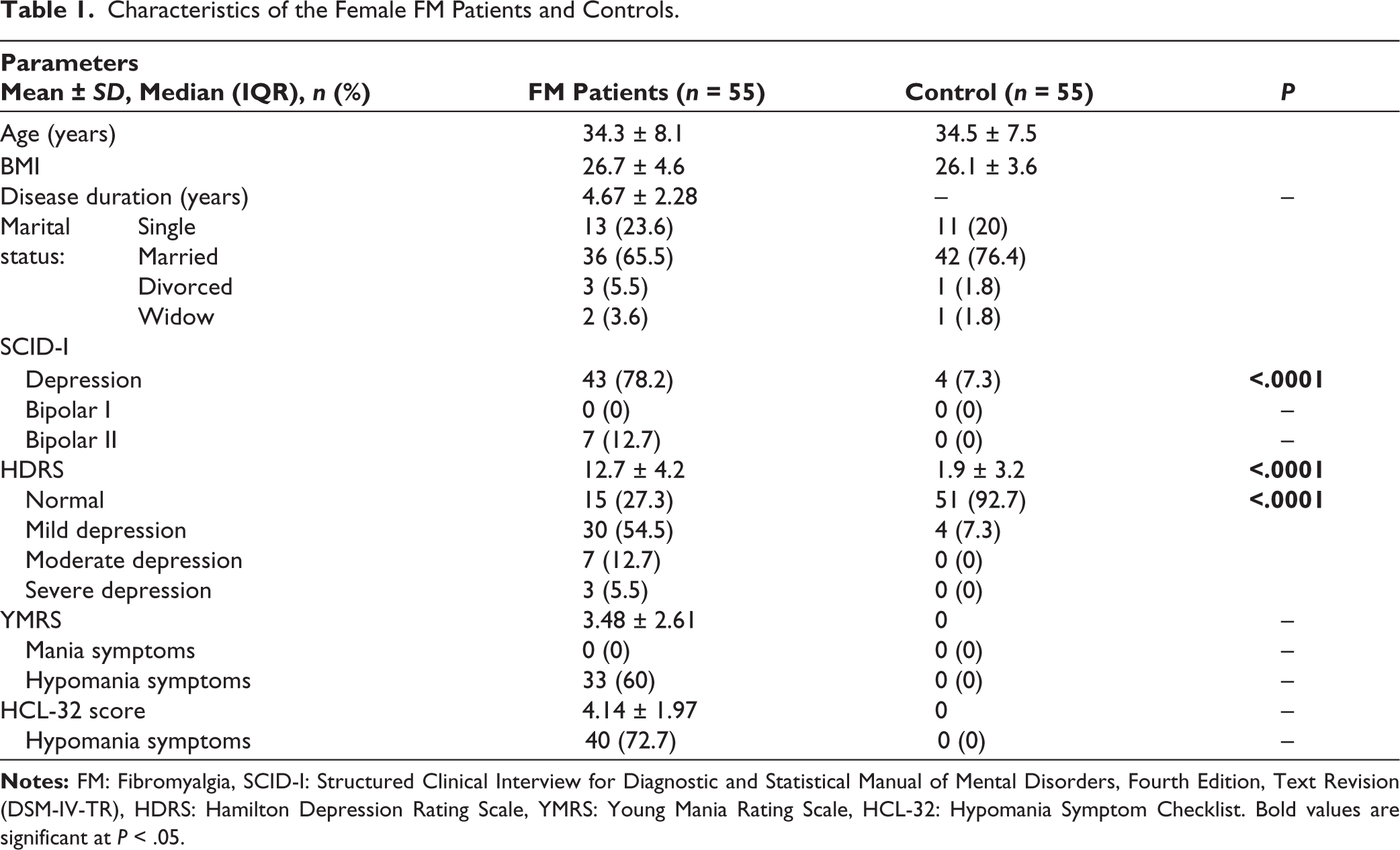
The HDRS mean score of FM patients was 12.7 ± 4.2, while that of controls was 1.9 ± 3.2 (P < .0001). Depression was found in 40 (72.7%) FM patients; 30 (54.5%) had mild depression, seven (12.7%) moderate and three (5.5%) severe. In control, only four (7.3%) had mild depression. No mania cases were diagnosed in either the patients or the control groups by YMRS. The HCL-32 revealed that 40 FM patients had hypomania symptoms compared to none of the controls. The mean score for hypomania symptoms in FM patients was 4.1 ± 1.97.
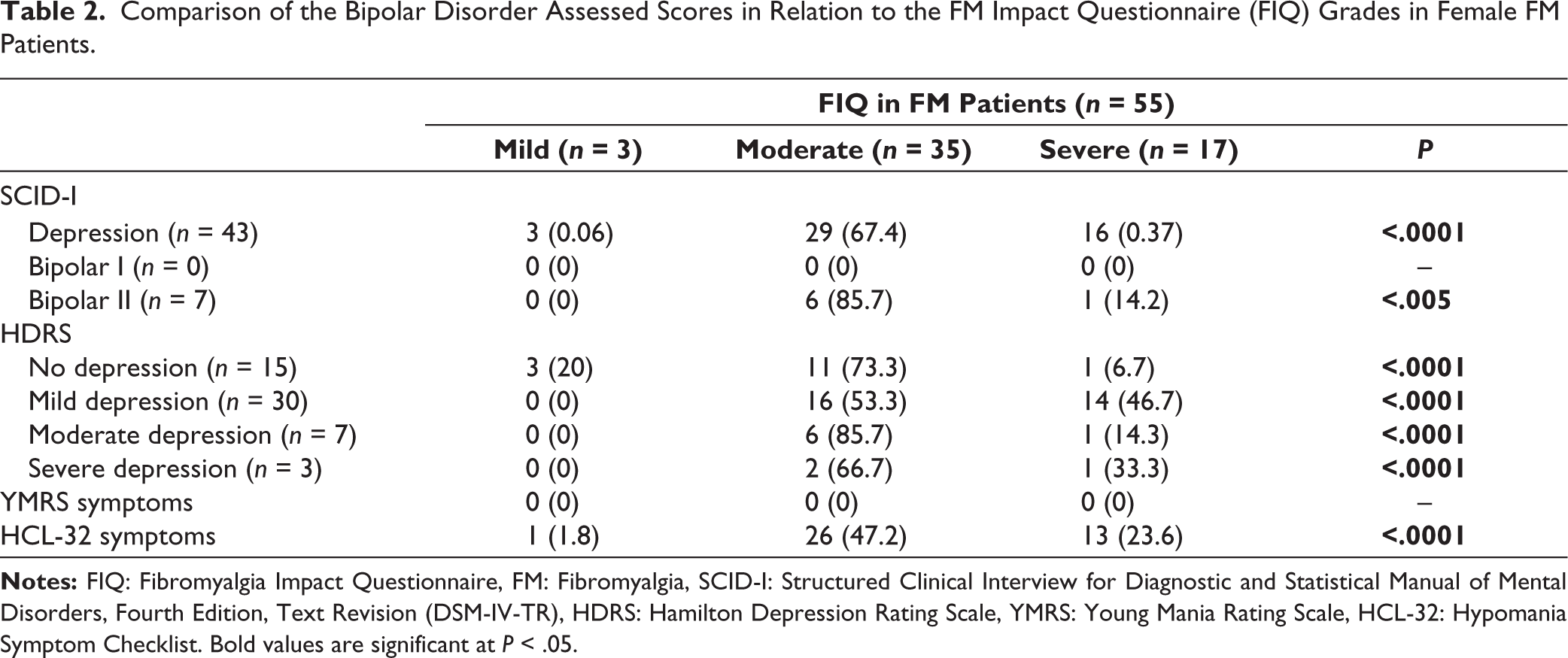
There was a significant association between psychiatric conditions and FIQ (Table 2). The FIQ was significantly related to depression (P < .0001), bipolar disorder II (P < .005), severity of depression (P < .0001) and hypomania (P < .0001). There was also a significant linear correlation between FIQ and HAD-M, YMS and HCL-32 (Table 3).
Comparison of the Bipolar Disorder Assessed Scores in Relation to the FM Impact Questionnaire (FIQ) Grades in Female FM Patients.
Correlation Between FIQ with HDRS, YMRS and HCL in 55 FM Patients.
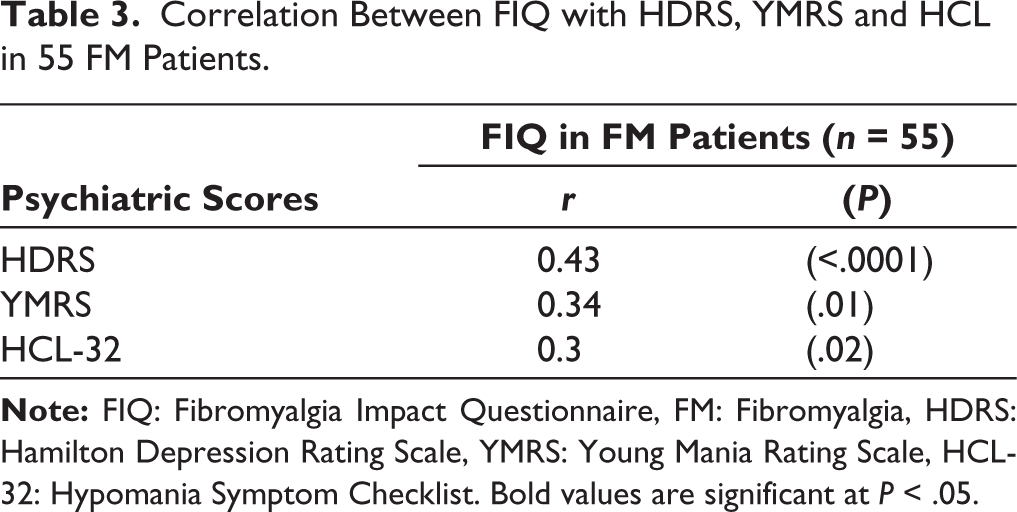
There was no correlation between FIQ with age (r = −0.11, P = .42) or BMI (r = 0.02, P = .87).
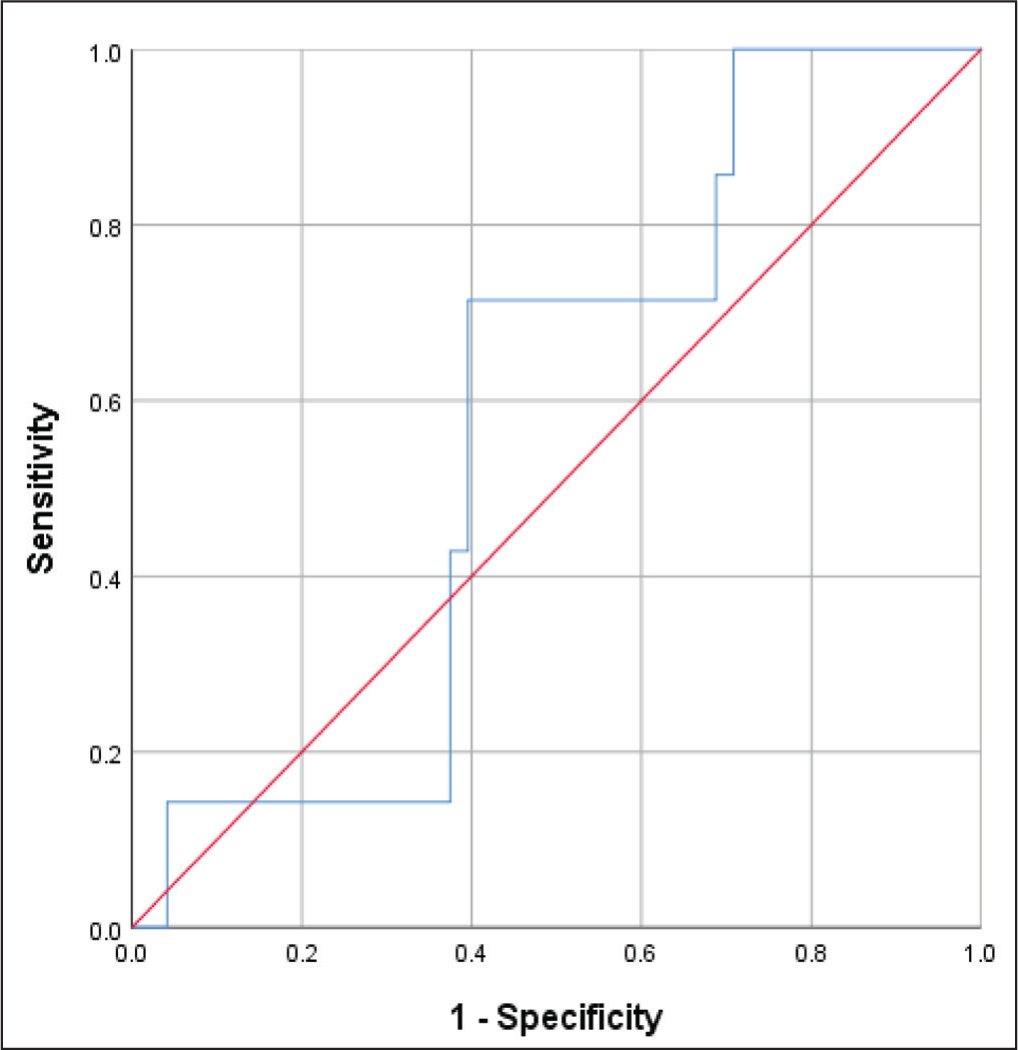
The ROC analysis showed that a FIQ cutoff of 58.17 could significantly predict depression with 76% sensitivity and 80% specificity (AUC = 0.84, P < .012) and at the same cutoff predicts bipolar II disorder with 85.7% sensitivity and 31.2% specificity (AUC = 0.57, P < .53) (Figures 1 and 2).
ROCs Analysis for FIQ to Predict Depression in 50 Cases (Including the Bipolar II). At FIQ 58.17, Sensitivity 76% and Specificity 80% at AUC = 0.84 and P = .01 for Depression.
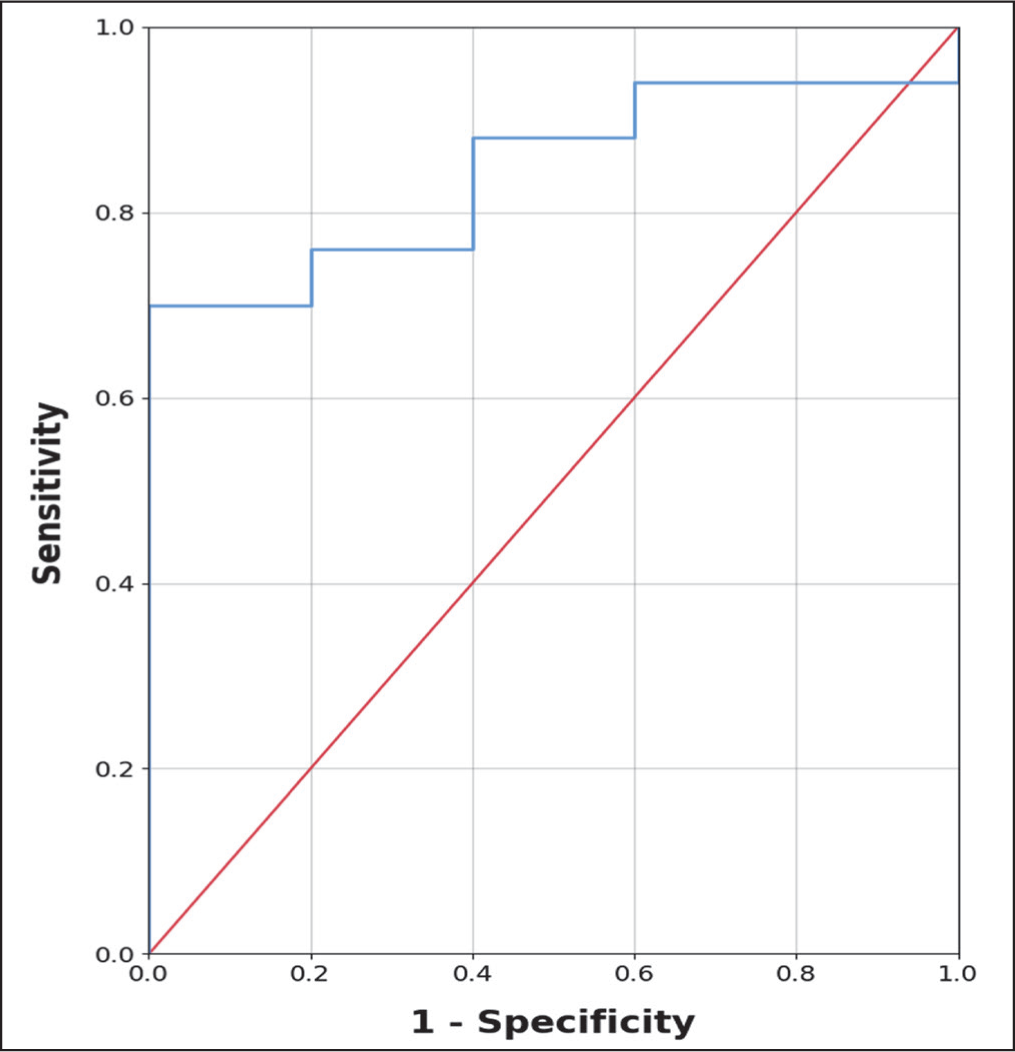
ROC Analysis for FIQ to Predict Bipolar Patients in Seven Cases. At FIQ 58.17, Sensitivity 85.7% and Specificity 31.2% at AUC = 0.57 and P = .53 for Bipolar II.
Discussion
Patients with FM frequently present with psychiatric symptoms and disorders, with about half experiencing major depression. 23 Coexistence with bipolar disorders may exacerbate FM symptoms such as pain, fatigue and insomnia. 24 In FM patients, major depression often occurs within the bipolar spectrum, accompanied by hypomanic symptoms, suggesting that bipolar disorder II is more commonly observed in FM patients than bipolar disorder I. 25 This study aimed to evaluate the frequency of bipolar disorders in FM patients and to assess the impact of FM on the functional outcome.
In the current study, a major depressive episode was diagnosed in 78.2% of FM patients using the SCID-I, while only 7.3% of controls were diagnosed with depression. The prevalence of depression in FM patients varies across studies. Alciati et al. reported that 50% of FM patients experienced major depressive episodes. 11 Gota et al. found a significant difference in HDRS scores between FM patients and controls, with depression in 60% of FM patients, 26 while Berkol et al. found depression in 70% of FM patients. 27 Wilke et al. reported that 78.1% of FM patients were clinically depressed, highlighting the severe impact of FM on mental health. 28 Gormsen et al. explored the relationship between FM and depression, emphasising the bidirectional relationship between pain intensity and sleep disturbances, which exacerbates both conditions and leads to higher levels of fatigue, daytime sleepiness and depressive symptoms. 29 The variation in depression prevalence among FM patients could be due to the multifactorial aetiology of depression and differing study methodologies. Both conditions have been linked to neurotransmitter imbalances and hypothalamic pituitary adrenal axis dysfunction. 15
In this work, 12.7% of FM patients were diagnosed with bipolar disorder II. The frequency of bipolar disorders in FM patients varies widely. Arnold et al. 30 reported a 12.8% lifetime prevalence of bipolar disorder among FM patients in the USA in a study from two community-based rheumatology practices, while Wilke et al. 28 found a 25.2% prevalence. Carta et al., 31 Alciati et al. 32 and Kudlow et al. 24 reported even higher rates, with bipolar disorder II diagnosed in 29.7%, 27% and 21.7% of FM patients, respectively. Alciati et al. 11 reported a 46.6% comorbidity rate of bipolar disorder in FM patients.
Hypomanic symptoms were identified in 72.7% of FM patients. A significant relation was found between the presence of hypomania symptoms and the FIQ. Depression often dominates bipolar disorders, leading to misdiagnosis as major depressive disorder. It is crucial to differentiate between bipolar disorders and major depressive disorder to ensure appropriate treatment, as FM patients frequently exhibit hypomanic symptoms that impact their mood and behaviour.32,33 Arnold et al. reported higher rates of mood fluctuations, including hypomanic symptoms, in FM patients compared to healthy controls. 30 They concluded that FM not only involves chronic pain but also involves mood disturbances.
This study also found that 15% of FM patients reported suicidal ideation. In a large meta-analysis including 394,087 FM patients, the suicide ideation prevalence was 29.6%. The combination of chronic pain and fatigue from FM, along with severe mood instability, characterised by depressive episodes and hypomanic symptoms from bipolar disorders, intensifies psychological distress and suicidal risk. 34
Although bipolar disorder I was not diagnosed in this study, Dell’Osso et al. 33 reported it in 6.3% of FM patients, and Arnold et al. 30 found it in 8.5%. Bipolar disorder I occurs in a subset of FM patients and contributes to mood disturbances.
Present findings revealed a significant relationship between mood disorders, including bipolar disorders II and depression and the functional outcome of FM patients, as measured by the FIQ. The relationship between mood disorders and FM severity has been well-documented. Wilke et al. 28 reported that higher levels of depression are significantly related to greater FM symptom severity. 28 Bipolar disorders exacerbate FM symptoms, including pain intensity, fatigue, sleep disturbances, cognitive issues and overall worsening of the clinical presentation of FM, contributing to greater functional impairment. 33
Several hypotheses have been proposed to explain the pathophysiological link between bipolar disorders and FM. Dysregulation in central neurotransmission, specifically in serotonergic and norepinephrine signalling, has been suggested to occur in both FM and mood disorders. 28 Experimental pain studies and functional brain imaging indicate that the increased pain perception in FM is related to enhanced sensory processing and decreased grey matter in areas involved in inhibitory pain modulation. These abnormalities in brain structure and function are also observed in bipolar disorders. 15 Wallace and Gotto 35 suggested that musculoskeletal pain in bipolar disorder patients may represent a pseudofibromyalgia caused by somatisation.
Diagnosing and treating FM and bipolar disorders together presents significant challenges due to the complexities of symptom overlap, potential interactions and the overall impact on the patient’s quality of life. Our study highlights the vitality of the multidisciplinary approach involving rheumatologists, psychiatrists, psychologists and physical therapists to manage both conditions effectively. The overlap in symptoms, such as chronic pain, fatigue and mood instability, necessitates confirming the FM diagnosis and identifying any comorbid psychiatric conditions.
This study has several limitations. First, the relatively small sample size resulted in the identification of only one patient with psychotic features. Second, recruitment from a single tertiary centre may limit the generalisability of the findings to broader populations. Third, the inclusion of only female patients restricts extrapolation to male patients with FM. Finally, the cross-sectional design precludes causal inferences and does not allow determination of temporal relationships between FM and psychiatric comorbidities. Larger, multicenter longitudinal studies are warranted to validate these findings and to more reliably assess these psychiatric conditions among FM patients.
In conclusion, bipolar disorder II is frequent in FM patients. The presence of mood instability, hypomanic symptoms and depression was related to a worse functional score. Current findings reinforce the importance of psychiatric evaluation in patients with FM to ensure early detection and management of bipolar disorders. On prescribing Serotonin-Norepinephrine reuptake inhibitors (SNRIs) to patients with FM, the risk of developing a manic episode is taken if this patient turns out to have bipolar disorder. Larger studies with more diverse groups should be conducted to further explore the prevalence, risk factors and the ideal methods of evaluation of these patients.
Footnotes
Authors’ Contribution
Author one conceived the study idea and design. Author two conducted patient interviews/screenings for bipolar symptoms and wrote the first draft of the manuscript. Author three assisted with the literature review, verified the FM diagnostic criteria and critically reviewed the manuscript for intellectual content. The author four supervised the entire project, provided final approval of the version to be published. All authors read and approved the final manuscript.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent and Ethical Approval
All subjects provided written informed consent to participate and publish. The research was approved by the Ethical Committee of Cairo University Hospitals (MS-15-2023).