
Abstract

Dear Editor,
Childhood-onset systemic lupus erythematosus commonly presents with haematological involvement, including autoimmune Hemolytic anemia, thrombocytopenia, and leukopenia. 1 Autoimmune Hemolytic anemia can be severe and difficult to manage, particularly in children with poor response to corticosteroids and intravenous immunoglobulin therapy. The coexistence of lupus-associated antiphospholipid syndrome or antiphospholipid antibody positivity may further complicate the clinical course. 2 Rituximab has emerged as a potential therapeutic option in refractory immune-mediated cytopenias. 3 We report two children with childhood-onset systemic lupus erythematosus and antiphospholipid antibody positivity who developed refractory autoimmune Hemolytic anemia and responded favourably to rituximab therapy. Informed consent was obtained from both patients’ families regarding the use of patient information for this case report publication.
A 7-year-old girl initially presented with mixed autoimmune Hemolytic anemia and thrombocytopenia (Evans syndrome). She experienced multiple relapses despite corticosteroids and repeated intravenous immunoglobulin. During her third relapse, she developed severe anemia, papilledema, and cerebral venous sinus thrombosis (Figure 1A). Autoimmune evaluation showed positive antinuclear and anti-double-stranded DNA antibodies with persistent anticardiolipin antibody positivity, consistent with childhood-onset systemic lupus erythematosus with secondary antiphospholipid syndrome. Owing to persistent bicytopenia despite corticosteroids and intravenous immunoglobulin, rituximab (375 mg/m 2 weekly for four doses) was administered (Figure 1B-timeline 1). She showed rapid haematological recovery and complete radiological resolution of thrombosis, and remains in sustained remission on follow-up.
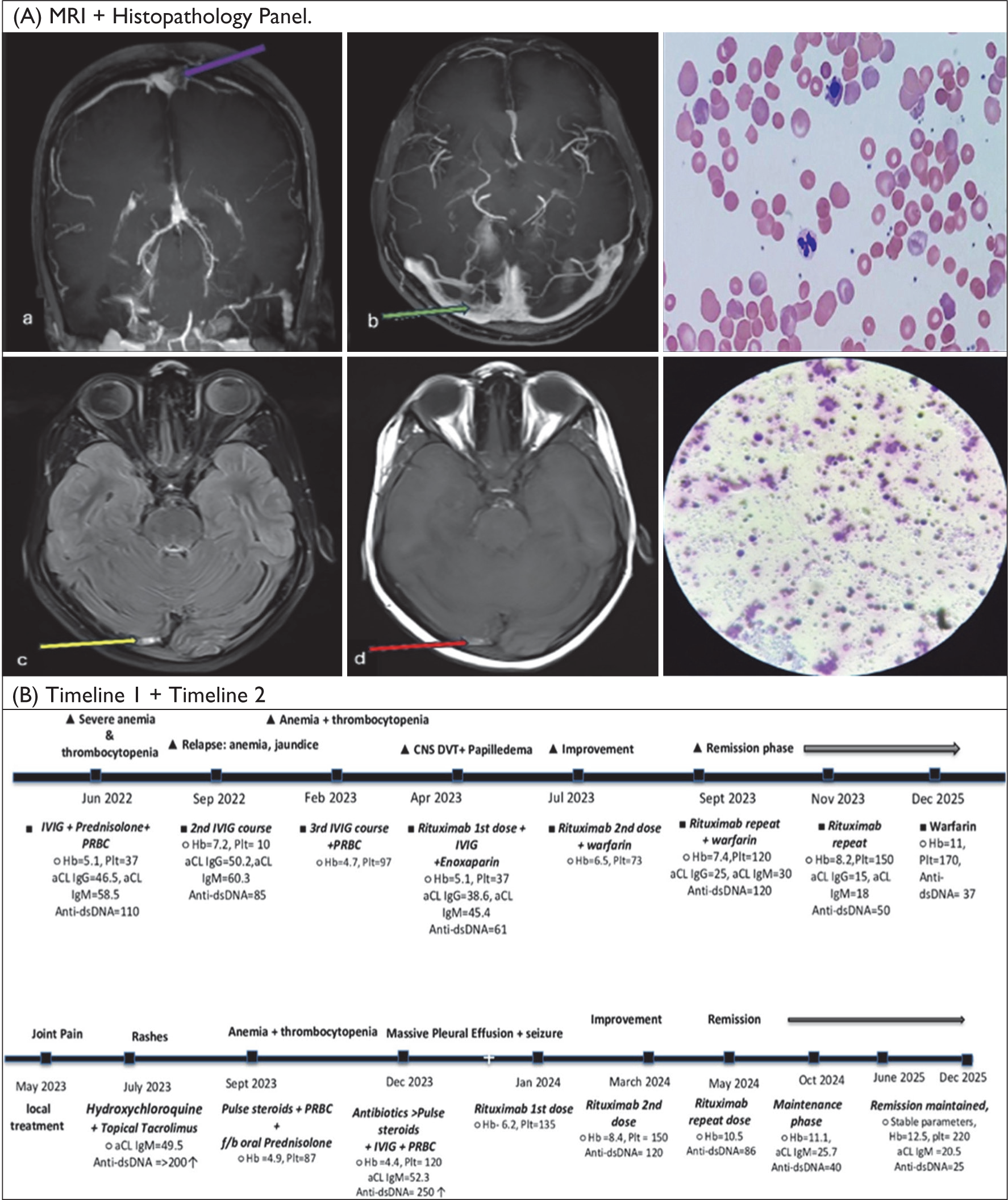
An 11-year-old boy initially presented with a 6-month history of progressive bilateral knee pain and low-grade fever, followed by oral ulcers, photosensitive rash, alopecia, and constitutional symptoms. He later developed severe anemia with bicytopenia and was diagnosed with childhood-onset systemic lupus erythematosus with autoimmune Hemolytic anemia and thrombocytopenia. He received intravenous methylprednisolone pulses with supportive care but showed persistent cytopenias and clinical worsening. The course was complicated by right-sided pleural effusion requiring intercostal drain insertion and intensive care support. Investigations confirmed Hemolytic anemia with positive direct and indirect Coombs tests, elevated reticulocyte count, positive antinuclear and anti-double-stranded DNA antibodies, and persistently elevated anticardiolipin immunoglobulin G and immunoglobulin M antibodies. He also developed seizures and behavioural changes suggestive of neuropsychiatric involvement. The clinical timeline is shown in Figure 1B-timeline 2. In view of steroid- and intravenous immunoglobulin-refractory disease, he received rituximab (375 mg/m 2 weekly), resulting in rapid clinical improvement with resolution of hemolysis, pleural effusion, and neurological stabilisation. He remains in sustained remission on maintenance therapy with corticosteroids, hydroxychloroquine, and low-dose aspirin.
Management of AIHA in pSLE remains largely extrapolated from adult data, with corticosteroids as first-line therapy and intravenous immunoglobulin reserved for severe cases. 4 However, relapsing, steroid-dependent, or refractory AIHA often necessitates second-line immunosuppression. Rituximab has emerged as an effective steroid-sparing option in refractory lupus-associated AIHA, with previous reports demonstrating sustained remission following 2–4 weekly doses. 5 Our cases further support its efficacy in children with the rare coexistence of pSLE, AIHA, and aPL positivity. Given the combined risk of Hemolytic and thrombotic complications, early recognition of this subset is essential. Rituximab may be considered early in refractory or relapsing disease. Multidisciplinary management is crucial for optimising outcomes.
Footnotes
Acknowledgements
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for publication of this case.