
Abstract
Background
Preterm neonates are not able to breastfeed due to immature sucking swallow reflexes and are kept on an alternative method of feeding until they are able to do so. The time to reach full oral feeds and breastfeed, the duration of feeding, and spillage are important parameters that need to be observed so that a baseline value can be provided, which can help healthcare professionals see the progression and appropriateness of feeding preterm neonates.
Objective
To assess the duration of feeding, spillage, weight changes, days to reach full oral feeds, full breastfeed, and length of hospitalization among preterm neonates.
Material and Methods
A descriptive study was carried out on 106 preterm neonates in the step-down unit of the NICU, PGIMER, Chandigarh. The variables under study were duration of feeding, spillage, weight changes, days to reach full oral feeds, days to reach full breastfeed, and length of hospitalization. The tools for data collection used were a socio-demographic profile along with a clinical profile of neonates, a neonatal assessment, and an observation sheet to record spillage and duration of feeding. The methods of data collection used were observation and biophysiological methods. Weight was assessed by the infant weighing scale present in the unit (in grams) and to measure spillage, a bib was used, and its pre- and post-feeding weight was measured on a diaper weighing machine. The values are expressed in grams. The data were collected from July 2021 to November 2021. The data are analyzed using the SPSS version 23.0.
Results
The results showed that neonates took an average of mean ± SD (range) 15.0 ± 3.12 (10−26) min to complete one feeding session, and spillage was around 1.37± 0.3 (0.8−2.3) g. The transition time to full oral feeds was 8.01 ± 7.21 (1–44) days, and the average time to reach full breastfeed was 26.7 ± 12.1 (5−56) days.
Conclusion
The present study has provided valuable data on duration of feeding and spillage that serves as a guide for the amount of milk that can be added to the prescribed feed. The information is also helpful in educating the parents to be patient while feeding the baby and wait for at least 3 weeks to 2 months to reach full breastfeed. Gestational age at birth and birth weight affect (negative correlation) the time to reach full oral feeds, breastfeed, and length of hospital stays (p < .05).
Introduction
A preterm neonate, as per the World Health Organization (WHO), is defined as a baby born before 37 weeks of completed gestational. 1 Prematurity is considered a global health problem by the WHO. India ranks among the first 10 countries with the highest number of preterm births. In India, about 3.5 million babies are born prematurely out of 26 million live births. The preterm death rate is even higher, at approximately 3.3 lakh per year. 2 Maintaining adequate nutrition in these preterm neonates is a big challenge, as direct breastfeeding is not possible in preterm neonates due to a lack of coordination and maturation of sucking, swallowing, and breathing reflex; until then, they are started on alternative methods of feeding. 3 WHO has recommended the use of a cup, Katori spoon or paladai for feeding the low-birth-weight babies who have not developed mature oro-motor reflexes. In addition to this, it is recommended to use infant cues to determine the frequency and duration of feeding. 4 Studies have shown that these methods lead to problems like increased feeding duration, spillage, and unintentional adverse effects. McKinney et al. did a systematic review of the cup feeding method in neonates and highlighted the problems of duration of feeding and spillage with this method. 5 Therefore, the duration of feeding and spillage are important factors that should be taken into consideration while the neonates are put on alternative feeding methods.
Previous studies have tried to find out the effect of perinatal factors on the outcome of these neonates. Patwardhan et al. carried out “a prospective cohort study and found that gestational age and weight at the time of birth were inversely related to time to reach full oral feeds” (p < .0001). 6 Similarly, another study was conducted by Yea shwu et al. to find out the predictors that affect the time to reach full oral feeds found that birth weight and neonatal illnesses like broncho-pulmonary dysplasia (BPD) and necrotizing enterocolitis (NEC) were significant predictors of post-menstrual age (PMA) to reach full oral feeds (p < .005). 7 However, the effect of duration of feeding and spillage has not been explored much in the previous studies. Therefore, a need was felt to assess these parameters. So, the present study aims to assess these variables to provide valuable information regarding these parameters that can be utilized in the care of preterm neonates.
Objectives
The aim of this study was to assess the duration of feeding, spillage, days to reach full oral feed, full breastfeed, weight changes, and length of hospital stays, and their relationship with selected sociodemographic variables among preterm neonates.
Material and Methods
The study was conducted in the neonatal unit of PGIMER, Chandigarh, for a duration of 6 months (June 2021−December 2021). It is a step-down unit of the NICU. Preterm neonates are shifted here from the NICU, and these preterm neonates are fed with a Katori spoon until they are able to breastfeed. The total enumeration sampling technique was used to enroll the participants. The inclusion criteria consisted of neonates with ≤34 weeks of gestation at the time of birth who were fit to start oral feeds. Based on gestational age, ability to coordinate sucking, swallowing, and breathing, and being declared fit to start oral feeds by a physician. Neonates with congenital birth defects of the gastrointestinal and nervous systems were excluded from the study. The primary investigator enrolled the study participants who met the inclusion criteria after getting informed written consent from their parents. A total of 106 neonates and their mothers/caregivers who met the eligibility criteria were enrolled in the study.
After the enrollment, demonstrations to the mother on how to feed the baby with a Katori spoon were given by nurses, and they provided feeds to the neonates until the mothers were confident to do so. Once the mothers start feeding independently, they continue to provide feeding round-the-clock under the supervision of nurses. The data collection started when mothers were about to start feeding with alternative methods.
Tools used for data collection were (a) socio-demographic profile along with the clinical profile of neonate and (b) neonatal assessment and observation sheet.
The observation method was used to assess the duration of feeding, spillage, and time to reach full oral feeds. The days to reach full oral feeds were estimated from day 1 after starting feeds with the Katori spoon until the day the neonate can take 150 mL/kg/day. Similarly, length of hospitalization and days to reach full breastfeed were calculated from the first day of enrollment until discharge of the neonate, and until the neonate was able to take full breastfeed for consecutively 3 days. The duration of feeding was assessed for half of the total feeding sessions, where 25% of the observations were made by the mother and the remaining 25% by the primary investigator. The count of spillage was made only from the 25% of observations made by the investigator, so as to ensure that every neonate is being observed daily by the investigator. To assess spillage, a pre-weighted bib was placed under the neck of the neonate at the time of feeding and weighed after the feeding. The spillage was calculated by subtracting the pre-feeding weight of the bib from the post-feeding weight. The weight (in grams) of the neonate was assessed as per unit protocol at the time of enrollment, weekly, and at the time of discharge by the nurses using an infant weighing scale. The value of continuous variables is expressed in mean ± SD (range). Descriptive and inferential statistics were used for data analysis. All data were analyzed using the SPSS version 23.0 statistical software for Windows, and statistical significance was set at p ≤ .05.
Results
A total of 106 neonates and their mothers/caregivers were enrolled in the study. Out of 106 neonates, half (54.7%) were boys, and the remaining were girls. Nearly half (62.3%) of the neonates were born between 28 and 32 weeks of gestation, with the mean ± SD (range) of 29.92 ± 2.020 (25–34) weeks. The birth weight was 1224.19 ± 304.01 (676–2128) g, with a majority (73.6%) of neonates having birth weights between 1000 and 2000 g. However, the post-natal age and weight at enrollment were found to be 33.07 ± 1.714 (30–39) weeks and 1357.7 ± 220.56 (1023–1994) g (Table 1).
Socio-Demographic and Clinical Profile of the Preterm Neonates (N = 106).
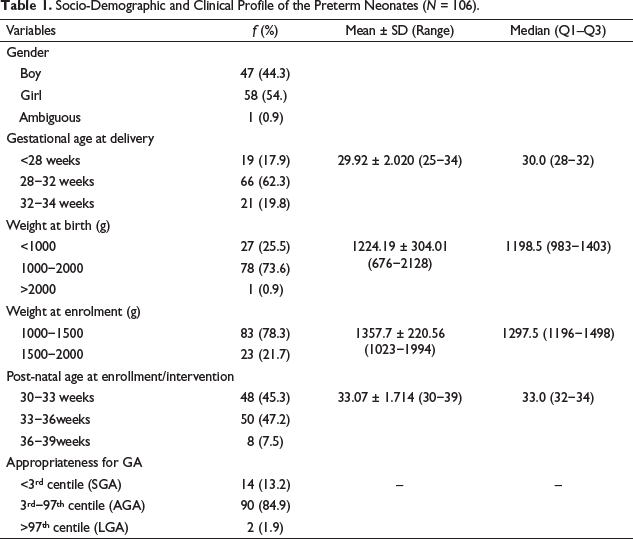
It was also found that the majority (84.9%) of neonates were appropriate for gestational age. The duration of feeding was assessed for 25% of feeding by mothers as 15.0 ± 3.12 (10–26) min, and 25% was recorded by the first investigator as 14.6 ± 2.8 (11–25) min, and the findings were homogenous at the .005 level of significance. It was recorded in the treatment chart for neonates. The spillage amount for 25% of observations was found to be 1.37 ± 0.3 (0.8–2.3) g (Table 2).
Discharge and Feeding Outcome of the Preterm Neonates (N = 106).
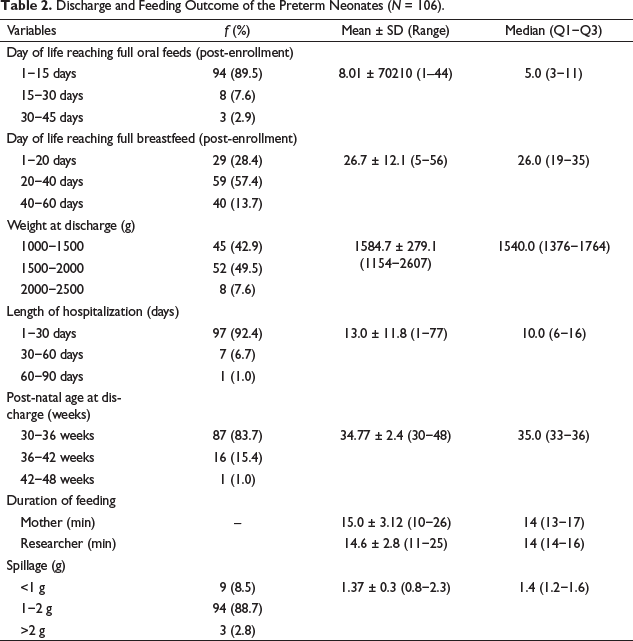
The day of life reaching full oral feeds, full breastfeeding and duration of hospital stay were calculated from the time of enrollment. The duration to reach full oral feeds was 8.0 ± 7.2 (1−44) days. The mothers were given recording sheet to note down duration of feeding and were taught by researcher how to record the same. The weekly telephonic follow-up were done till the baby start taking full breastfeed. It was found that nearly half 108 (57.4%) of neonates took full breastfeed in 26.7 ± 12.1 (5−56) days. The length of hospital stay was found 13.0 ± 11.8 (1−77) days.
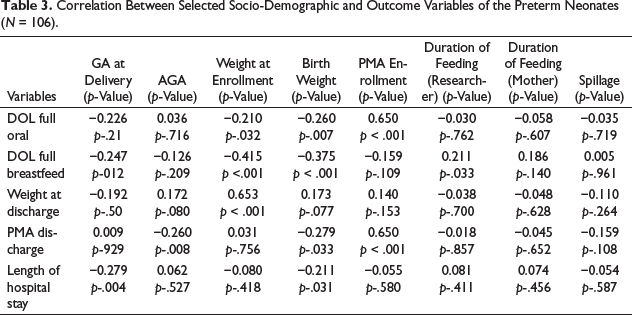
Gestational age at birth and weight at enrollment have a negative relationship with discharge and outcome variables (p < .005). This means that the higher the birth weight, the shorter the time to reach full oral feeds or breastfeed, and the shorter the length of hospitalization (Table 3).
Correlation Between Selected Socio-Demographic and Outcome Variables of the Preterm Neonates (N = 106).
Discussion
Preterm neonates lack the ability to breastfeed; therefore, they are started on alternative methods of feeding. The recommendations for feeding depend on the gestational age and oral skills of preterm neonates. Therefore, when the neonates are started on spoon/paladai feeds, the duration of feeding, spillage, and the number of days to reach full oral feeds are some parameters that need to be monitored to understand the transition from oral feeds to breastfeed and also to assess whether the feeding approach used by healthcare professionals is appropriate as per the condition of the neonates. The present study was conducted to observe these parameters in 106 preterm neonates. Mothers provided feeding to neonates. The methods of data collection were observation, measurement of spillage, and biophysiological methods. The data were collected over a 6-month period.
The PMA at the time of enrollment was 33.07 ± 1.714 (30–39) weeks, and it was found that once a preterm neonate is started on oral feeds from gavage feeds, the mean transition time is 8 days. The PMA to achieve full oral feeds was 35.8 weeks. The results are similar to the findings of the study done by Brun et al., in which they found that neonates born before 32 weeks of gestation reache full oral feeds at 36 6/7 weeks of PMA. 8
It was observed that preterm neonates completed the feed given in an average time of 14.6 ± 2.8 (11−25) min and spilled nearly 1.37 ± 0.3 (0.8−2.3) g of milk. A nearly similar amount of spill was reported in a study done by Manjinder et al. comparing spoon feed with paladai as 1.5 ± 2.5 g (spoon), 1.3 ± 2.8 g (paladai). 9 However, in previous studies, duration of feed and spillage were only measured qualitatively by asking mothers/caregivers.10, 11 It has also been suggested by previous research that if a neonate spends more than 20 min feeding, the energy expenditure increases, which can result in a decrease in weight gain. 12
In the present study, it was observed that the length of hospitalization was 13.0 ± 11.8 (1−77) days, and the PMA at discharge was 34 weeks. However, contrary to these findings, Maier et al. reported that a length of hospitalization of more than 63.6 (54–0–70.1) days. 13 The shorter duration of stay in the present study could be due to our referral system to the state-level neonatal care unit (SNCU) after stabilizing the neonate.
In the index study, we also analyzed factors that affect full oral feeds and length of hospitalization, and it was found that low gestational age at delivery, birth weight, and PMA at enrollment are the contributory factors for the delay in time to reach full oral feeds and the long hospital stay. Similar findings have been reported by Jackson et al. 7 and Murki et al. 14
The present study added to the existing knowledge related to time to reach full oral feeding, breastfeeding, and length of hospital stay.
Conclusion
The present study concluded that days to reach full oral feeding, full breastfeeding, and length of hospitalization correlate with the clinical picture of the neonates; therefore, for the neonates who are sick, who have a lower gestational age at birth, and who have a low birth weight, healthcare professionals should be more vigilant while giving feed. The duration of feeding and spillage should be considered while feeding the neonates with alternative methods of oral feedings.
Recommendations
The findings of the study suggest that the preterm neonates fed with a Katori spoon or any other cup require an additional 1.5−2 mL of extra milk to the recommended feed to meet the loss of feed that happens due to the spillage. In addition, the nurses must educate the mothers, that if the neonate takes more than 10–15 min during a single oral feeding session, the remaining feed must be given through an orogastric tube to ensure the conservation of energy and adequate weight gain of the neonate.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval to conduct study was taken from Institutional Ethics Committee.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed written consent was taken from mothers before enrolling the neonates to study.