
Abstract
Background
Tattoo-acquired hepatitis B virus (HBV) infection is an under-recognized source of acute hepatic insult. Tattooing has emerged as a non-traditional yet significant source of HBV transmission, particularly when done from unregularized parlors. HBV can serve as an acute insult precipitating acute-on-chronic liver failure (ACLF) in patients with underlying chronic liver disease, such as nonalcoholic steatohepatitis (NASH). ACLF refers to a reversible clinical syndrome having high short-term mortality, characterized by acute hepatic insult leading to liver decompensation in patients with underlying chronic liver disease. 1 The condition can be precipitated by various acute events, including viral infections. This case report describes a rare instance of tattoo-acquired hepatitis B infection precipitating ACLF in a patient with asymptomatic undiagnosed NASH.
Case Presentation
A 34-year-old male, with a body mass index of 24.4 kg/m² and no significant medical history, presented with jaundice, nausea, vomiting, and fever after undergoing a tattoo procedure a few weeks prior. Liver function tests revealed elevated transaminases, high bilirubin levels, and prolonged prothrombin time. Hepatitis B surface antigen (HBsAg) was positive, while tests for other hepatitis viruses, including hepatitis A, C, and E, were negative. Imaging and liver biopsy indicated underlying NASH with fibrosis but no cirrhosis. The patient was treated with antivirals, antibiotics, and diuretics, showing significant improvement by the time of discharge.
Conclusion
Tattoo-related HBV infection can precipitate ACLF in individuals with silent chronic liver disease. This case underscores the importance of public awareness, regulation of tattooing practices, and vigilance for NASH, even in non-obese individuals.
Introduction
Hepatitis B virus (HBV) is responsible for a significant proportion of acute-on-chronic liver failure (ACLF) cases, particularly in the Asia-Pacific region. The World Health Organization (WHO) estimates that over 296 million people live with chronic HBV infection globally, with unsafe injections, blood transfusions, and tattooing listed as transmission risks. 2
Tattooing can lead to HBV infection when aseptic precautions are not followed. Studies have identified an increasing prevalence of HBV among individuals receiving tattoos from unlicensed or informal settings. In India, the under-regulation of tattoo parlors poses an overlooked public health challenge.
ACLF is a clinical syndrome defined by acute hepatic insult in a patient with pre-existing chronic liver disease, leading to liver decompensation manifesting as jaundice, coagulopathy, ascites, and/or encephalopathy. The Asia-Pacific Association for the Study of Liver (APASL) recognizes ACLF as an acute event manifesting as jaundice or coagulopathy, superimposed on previously diagnosed or undiagnosed chronic liver disease, which may or may not involve cirrhosis. 3 This case report presents a unique scenario of tattoo-acquired hepatitis B infection precipitating ACLF in a patient with asymptomatic undiagnosed nonalcoholic steatohepatitis (NASH). We discuss the role of hepatitis B as an acute precipitating factor in the background of NASH and the potential consequences of unsafe tattooing practices.
Case Presentation
Patient Information
A 34-year-old male with a body mass index (BMI) of 24.4 kg/m² and no history of diabetes, hypertension, or alcohol consumption presented to the hospital with a 1-month history of jaundice, preceded by a 2-day prodrome of nausea, vomiting, and fever. He reported having recently received a tattoo about 4 weeks before the onset of symptoms and was concerned about the possibility of a bloodborne infection. Three weeks after the onset of jaundice, he developed ascites and pedal edema.
Clinical Findings
On admission, the patient was jaundiced with signs of ascites but no evidence of encephalopathy. Physical examination revealed a smooth, non-tender, and firm liver spanning 15 cm. Other systemic findings pertaining to the cardiovascular, nervous, and musculoskeletal systems were within normal limits.
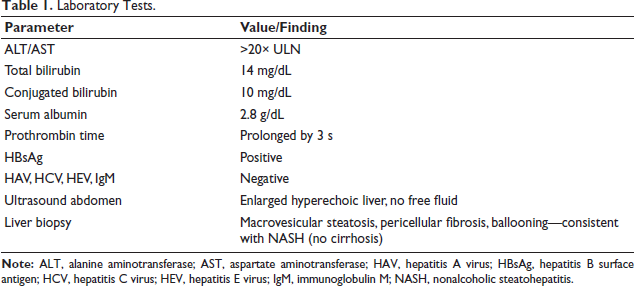
Laboratory Tests
Laboratory tests are revealed in Table 1.
Laboratory Tests.
Diagnostic Focus and Assessment
Further investigation, including liver biopsy, was performed to assess the underlying cause of chronic liver disease. The biopsy findings were consistent with NASH with advanced fibrosis but without cirrhosis.
Liver Biopsy
The histological features included macrovesicular steatosis, mild hepatocellular ballooning, pericellular fibrosis, and portal fibrosis with lymphocytic infiltrates.
These findings indicated underlying NASH without cirrhosis. The acute insult of hepatitis B infection, acquired potentially through the tattoo procedure, was considered the precipitating factor for the development of ACLF.
Management and Treatment
The patient was diagnosed with ACLF, triggered by hepatitis B infection superimposed on underlying NASH. The management strategy included antibiotics, antivirals for hepatitis B infection, and diuretics for ascites control, along with dietary modification focusing on protein optimization. Over time, the patient showed marked clinical improvement. His bilirubin levels decreased to 2.5 mg/dL, aspartate aminotransferase (AST) and alanine aminotransferase (ALT) returned to normal, and his prothrombin time normalized. Ascites resolved, and the patient’s liver function progressively improved, returning to a compensated state.
Nursing Management
Management of Infection
Nursing care for infection control in ACLF focuses on early identification of sepsis and the implementation of standard precautions to prevent healthcare-associated infections. In this case, the patient presented with signs of systemic inflammation and was at risk of secondary bacterial infections. Nurses played a key role in monitoring temperature, white blood cell counts, and cultures. Strict aseptic techniques were followed during all invasive procedures. Empirical antibiotics were administered promptly as per sepsis protocols, and nurses ensured timely delivery and documentation. 4
This nursing intervention contributed to early sepsis identification, resulting in timely antibiotic initiation and a favorable outcome.
Management of Jaundice
Managing jaundice in ACLF involves both physical and psychological support. Nurses monitored bilirubin levels and skin/mucosal integrity daily. Patient comfort was enhanced through frequent skin care, use of light cotton clothing, and environmental adjustments. Nutritional support, particularly low-fat, high-protein diets, was promoted under dietitian guidance. Education was provided regarding the cause of jaundice and recovery expectations. 5
These nursing interventions enhanced recovery and promoted patient comfort.
Management of Fluid Overload
Patients with ACLF are prone to third-space fluid shifts, leading to edema and ascites. Nurses assessed for pedal edema, daily weight changes, abdominal girth, and monitored input–output strictly. Fluid and sodium restrictions were reinforced. Diuretic therapy was administered as prescribed, and renal function was closely observed. Patient positioning (semi-Fowler’s) was adjusted to reduce discomfort from ascites and improve ventilation. 6
Timely monitoring enabled daily assessment of the patient’s condition, allowing for appropriate dose adjustments and prevention of significant electrolyte imbalances.
Monitoring Hepatic Encephalopathy
The nursing team regularly assessed mental status using tools like the Glasgow Coma Scale and West Haven Criteria to have a close watch on the development of signs of deterioration, which facilitated prevention of the development of hepatic encephalopathy. 7
Discussion
Hepatitis B Infection Through Tattooing
Hepatitis B is primarily transmitted through contact with infected blood or bodily fluids. 8 While the infection is commonly associated with intravenous drug use and unprotected sexual contact, non-traditional modes of transmission, such as tattooing, are becoming increasingly recognized. Tattooing with non-sterile needles and equipment can lead to the transmission of bloodborne pathogens like hepatitis B, as seen in this case. This highlights the importance of ensuring that proper hygiene and sterilization procedures are followed in tattoo parlors to minimize the risk of hepatitis B and other infections.
ACLF in NASH
While ACLF is often associated with cirrhosis, it can occur in patients with chronic liver diseases, such as NASH, that have not progressed to cirrhosis. 9 The presence of underlying NASH in this patient contributed to the development of ACLF after a superimposed acute insult. This case emphasizes the need to consider NASH as an underlying chronic liver condition, even in the absence of cirrhosis, especially in the context of acute hepatic decompensation.
Prevalence of NASH and Hepatitis B in India
NASH is an increasingly common cause of liver disease in India, with studies showing a significant rise in its prevalence due to lifestyle changes, particularly among non-obese, non-diabetic individuals. 10 Hepatitis B remains a major public health concern in India, with significant efforts needed to prevent its transmission through unsafe practices, including tattooing.
Conclusion
This case emphasizes the need for greater awareness about HBV transmission through tattooing and the critical role of identifying underlying chronic liver conditions like NASH. It calls for stricter regulation of tattoo parlors, proper sterilization practices, and public education on the risks associated with tattoos. Screening for silent NASH in healthy individuals may also be warranted in selected settings.
Footnotes
Acknowledgments
The author thanks the medical and laboratory teams involved in the diagnosis and management of this patient.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The type of study does not require institutional ethical clearance.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Patient consent has been obtained and anonymity is ensured.