
Abstract
Background
Type 1 diabetes (juvenile diabetes) is a chronic metabolic disorder that causes the pancreas to make little or no insulin in children. Symptoms of juvenile diabetes can develop in just a few months. It has a major impact on the quality of life of children and the lived experiences of their parents, particularly mothers.
Methodology
A mixed-method convergent parallel design was used, and a sample size of 60 children with type 1 diabetes was selected for the quantitative approach. A semi-structured focus group interview was conducted with 20 mothers to assess the lived experiences of mothers of children with diabetes. Socio-demographic data, the clinical profile of type 1 DM children and PedsQL™ Generic Core Scale were used for the quantitative approach.
Result
Almost equal proportions (38%) of children had good and average quality of life, as per children’s self-reports and parent proxy reports. However, about 18% of children reported that they had a poor quality of life, while 13% of parents reported that their children had a poor quality of life. Three themes were extracted from the lived experiences of mothers: sharing experiences of care; personal, psychosocial, and schooling concerns; and barriers to quality care for diabetic children.
Conclusion
In the present study, the majority of diabetic children diagnosed with type 1 diabetes had a good quality of life, as per diabetic children’s self-reports and parents’ proxy reports. Quality of life was found to be good in the social domain in comparison with other domains. Mothers of children with diabetes dealt with the challenges of managing physical symptoms, had concerns about their children’s future, and faced various personal, psychosocial, and financial management issues. Therefore, by identifying these experiences and challenges, we can say that mothers of diabetic children need a unique and flexible program on diabetes management.
Introduction
Type 1 diabetes mellitus (juvenile diabetes) is an autoimmune disorder characterized by a complete deficiency of human insulin due to immunological destruction of pancreatic cells (beta cells). 1 It requires regular blood sugar monitoring and insulin administration throughout life. This disorder has a significant impact on children’s lifestyles and daily living in different aspects. Type 1 diabetes management requires a balanced diet and exercise to maintain a healthy lifestyle and prevent related complications. 2 The average prevalence of juvenile diabetes in India is about 10.2 per 100,000 population, which is alarming for the health system. 3
The risk of diabetes is 15 times higher in first-degree relatives, and the risk remains 6% until the third decade of life. 4 Compared to girls, boys have a higher incidence rate, and a bimodal peak has been observed; the first peak is observed from the age of 4 to 6 years, and the second peak is observed from the age of 10 to 14 years. Three sets of prevalence data in different settings revealed that 17.93 cases per one lakh children in Karnataka, 3.2 cases per one lakh children in Chennai, and 10.2 cases per lakh children in Karnal (Haryana) had type 1 diabetes. Type 1 diabetes mellitus among children has increased with a trend of 3%–5% per year. 5 Diabetes mellitus permanently changes children’s lives. Patients’ self-care, consisting of daily insulin injections, self-monitoring of blood glucose, and a diabetic diet, has a huge impact on quality of life. The World Health Organization defines QoL as “an individual’s perception of their position in life in the context of the culture and value system in which they live and in relation to their goals, expectations, standards and concerns.” 6
Diabetic children face different challenges that include both physical and mental health problems. Some of the psychological problems related to diabetes are adjustment disorders, depression, anxiety and eating disorders. 7 Children with diabetes face challenges related to absenteeism from school, homesickness due to hospitalization and growth and development. Moreover, hypoglycemia and higher HbA1c levels could be fatal to the developing brain of children and are directly related to depression, so early diagnosis and treatment are important to control complications in diabetic children. 8 Furthermore, QOL is an important aspect of diabetes management because poor quality of life leads to diminished self-care, which in turn leads to worsened glycemic control and increased risk for complications: blindness, end-stage renal disease, limb amputations, and increased mortality due to coronary artery disease, cerebrovascular disease, or peripheral vascular disease. 9 Dynamic and continuous awareness about the management and prevention of diabetes-related complications is necessary to ensure a good quality of life in diabetic children. However, caregivers face many challenges due to a lack of awareness about diabetes management and thus go through a lot of stress. 10 Among all the caregivers, mothers are affected more than other family members, and this leads to physical and psychological issues among them. 11 An overwhelming experience, constant vigilance, and a holistic environment of care are essential while caring for patients with type 1 diabetes mellitus. Thus, the management of diabetes is a time-consuming activity that requires modifications in the daily life of diabetic children along with their family members. 12 Mothers of diabetic children should know the normal and life-threatening conditions and complications related to this disease. A healthy home atmosphere can be useful to provide care, warmth, support, and a healthy lifestyle for children with diabetes. 13 Moreover, the care of diabetic children should not be restricted to hospitals and nursing homes. Therefore, to enhance a safe and effective social environment for diabetic children, responsibilities are often extended to family members and teachers. Children with diabetes should be managed and treated in school the same way they are treated at home. They should be medically safe at school and get equality in educational opportunities; therefore, they should not be excluded from extracurricular activities in school. 14
When a child falls ill, the whole attention of family members shifts to the child; in this situation, no one in the family thinks about the condition of the parents, especially the mother who cares 24/7 for the child. A study showed that the prevalence of parental psychological distress is around 20%–30%, and 59%–74% of parents of newly diagnosed type 1 diabetic children have anxiety and depressive symptoms. 15 Hence, it is important to recognize the problems faced by mothers and their lived experiences.
Although diabetes does not have a cure, effective management with daily self-care can result in tremendous results among children. Interventions for management include a multifactorial team approach, such as a team of physicians, nurses, and dietitians; however, without the participation of parents, it can be difficult to attain effective self-care for diabetic children. 16 This study will unveil the kind of problems faced by mothers so that they can be dealt with in a better way.
Diabetic children need a great deal of energy to maintain a QOL as other children without diabetes do. Readiness for school and college can create anxiety among diabetic children; therefore, a strategic plan of action for this phase is required. If children are adequately educated and trained to deal with this problem, their QOL will surely improve. 17 Moreover, mothers of children suffering from type 1 diabetes mellitus also present with various doubts and concerns regarding their children’s health, and this indicates the need for conducting a mixed-method study so that, in this context, a proper understanding of this issue can help in future policy making.
Materials and Methods
Study Design: Mixed-method Study, Convergent Parallel Design
Location and duration of the study: a convenience sampling technique was used to select the hospitals for the study. The study was conducted from September 2018 to May 2019 at the outpatient departments of four selected hospitals.
Quantitative Study
Sample and Sampling Criteria
Children aged 2–18 years diagnosed with type 1 diabetes for more than 6 months visiting outpatient departments of the selected hospitals were included in the study. Children diagnosed with type 1 diabetes were selected using a total enumerative sampling technique. Quantitative sample size was calculated by using Statulator online calculator, and 60 children with type 1 diabetes were enrolled from different hospitals.18, 19 Children diagnosed with type 1 diabetes (duration of more than 6 months) visiting the outpatient department of selected hospitals were included in this study. Diabetic children with other major unmanageable diseases, children and parents who could not understand and speak Hindi or English, and those not willing to participate in the study were excluded.
Data Collection Procedure and Tools
Part A: Socio-demographic profile of children and mothers of diabetic children included baseline information of the diabetic children including their mothers’ age, gender, habitat, class, number of siblings, birth order, educational status of parents, health status of the mother, religion, type of family, occupational status, current marital status of the mother, monthly income of the family (INR), and number of family members. Part B: the clinical profile of the children comprised clinical data such as medical diagnosis, other investigations, treatment, and complications.
Part C: PedsQL™ Generic Core Scale (pediatric quality of life): This tool has been applied and tested to assess the quality of life of diabetic children worldwide and in India; it was tested on diabetic children from Kerala state. The Hindi version (PedsQL 4.0) of the tool was used as it was reliable and tested with internal consistency (α = 0.88 for the children’s report and α = 0.89 for the parents’ report). This tool consists of four domains, and every domain has different items, such as physical functioning (8 items), emotional functioning (5 items), social functioning (5 items), and school functioning (5 items). PedsQL 4.0 Generic Core Scale presented in parallel formats (child self-report and parent proxy report). The child self-report questionnaire was divided into three different age groups, that is, 5–7 years, 8–12 years, and 13–18 years. The parent proxy report included a questionnaire for ages 2–4 years (toddler), 5–7 years (young child), 8–12 years (child), and 13–18 years (adolescent). A five-point Likert response scale was used across the child self-report for ages 8–18 years and the parent proxy report. A three-point scale was utilized for the younger age groups of 2–4 years and 5–7 years’ parent proxy report (Table 1).
PedsQL™ Generic Core Scale (Pediatric Quality of Life).

Data Analysis
The data were analyzed using SPSS Statistics version 23 (IBM Corporation, USA), and descriptive statistics (for the categorical distribution of the demographic characteristics of the children and parents’ profiles as percentages and frequencies) and inferential statistics (one-way ANOVA) were used to analyze the data.
Qualitative Research
Sample and sampling technique: The study included mothers whose children, aged 2–18 years, were previously diagnosed with type 1 diabetes for a period of at least 6 months and were visiting the outpatient departments of the chosen hospitals. Data were obtained from mothers of diabetic children till data saturation, which was achieved after interviewing 20 mothers of diabetic children. Data saturation was evidenced by repeated themes and subthemes until no new information was obtained from different settings and different groups of participants. Written informed consent from the mothers was obtained for each interview, photograph, and audio and video recording. The anonymity of the subjects and the confidentiality of the information were maintained throughout.
Data Collection Procedure
The socio-demographic profile data sheet was filled out to obtain demographic details of the participants; thereafter, a semi-structured focus group interview was conducted to assess the lived experiences of mothers of diabetic children. Semi-structured, open-ended questions were introduced. The first two questions were general questions, which were used as icebreakers or to make the mothers comfortable. The remaining questions focused on assessing their opinions and experiences in caring for their diabetic children. The responses were videotaped. Bracketing was done before collecting data through self and peer review and a nonjudgmental approach to the participants.
Validity and Reliability
The content validity of the data collection tools was obtained from five subject experts. Lincoln and Guba’s criteria were utilized for establishing the level of trustworthiness. Credibility (the researcher’s “reflective commentary” and videotaping were done to capture information accurately), confirmability (interview transcriptions were checked by an independent person for objectivity), dependability (peer debriefing/scrutiny), and transferability (detailed reporting of the research process and thick description of findings) were maintained.
Data Analysis and Interpretation
Data were analyzed into various steps: Immediate debriefing after the focus group interview was done, and notes were made during the interview. Viewing and listening to the video and transcribing the content as written notes. The content of the video was matched with the notes, and nonverbal behavior was also considered. Thereafter, transcription and translation of the verbatim into English from Hindi, and the English transcripts were checked by an independent person for objectivity. Coding of data in RQDA software and thematic analysis: accurate themes and subthemes were generated.
Results
Socio-demographic Profile of Diabetic Children
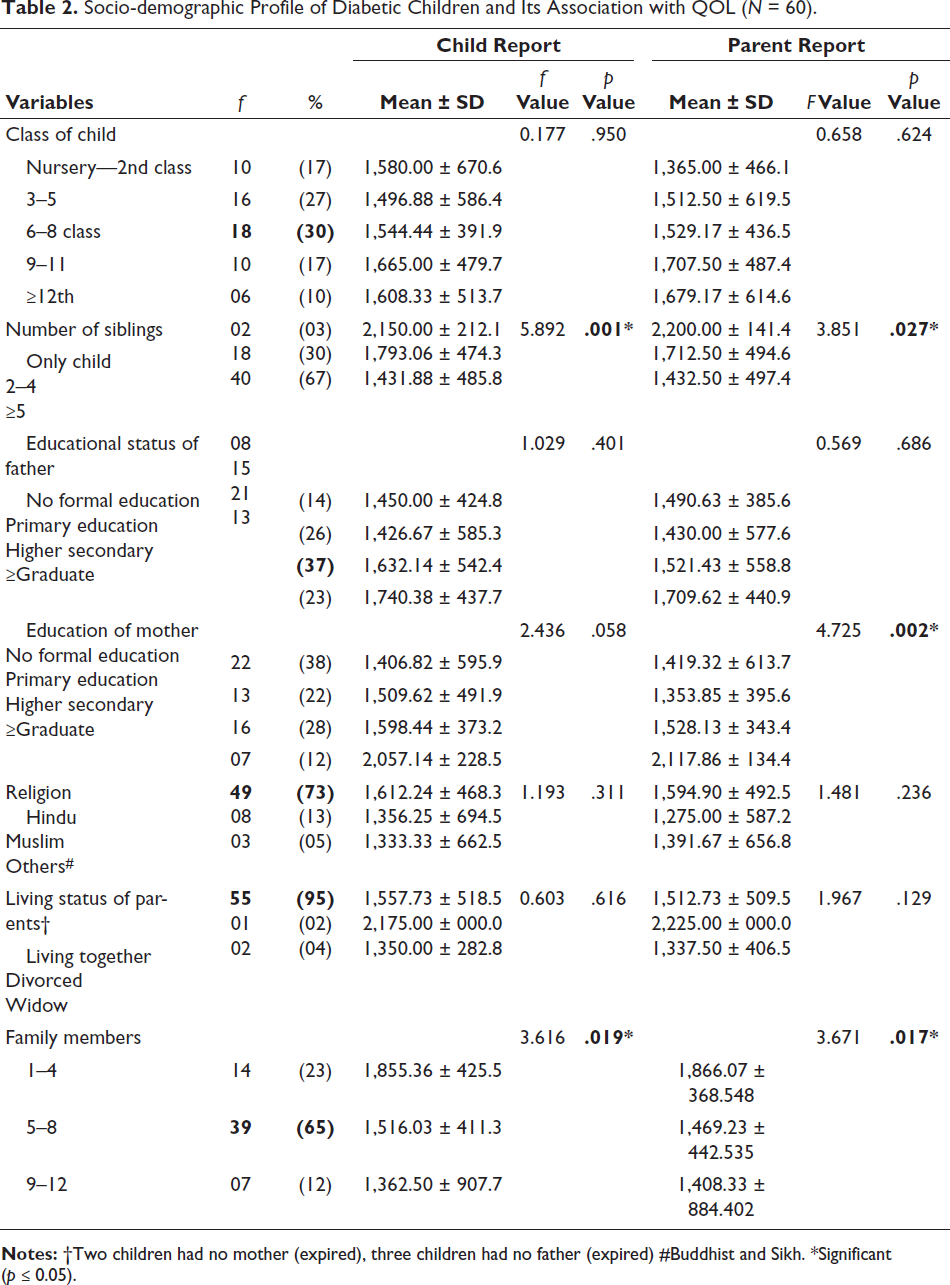
As per age, more than half (60%) of the children were 13–18 years old, and more than half (62%) were males. About two-thirds (73%) of the children were Hindu by religion. Around 52% of the children were from urban areas, while the remaining 48.3% were from rural areas. About two-thirds (73%) of the children were from nuclear families. Regarding class, less than one-third of the children had an education between the 6th and 8th standards (Table 2).
Socio-demographic Profile of Diabetic Children and Its Association with QOL (N = 60).
Of the mothers chosen for the interview, the majority (90%) were between the ages of 25 and 45 years; three-fourths of the mothers (75%) belonged to the Hindu religion and had nuclear families. About 55% were from urban habitats, while 45% were from rural habitats. Half of the mothers (50%) did not have any formal education, and 90% were homemakers. Also, a majority of mothers (90%) had no chronic illness. Nearly 5% of mothers were widows.
Association of Quality of Life of Diabetic Children with Socio-demographic Profile
A statistically significant association was found between the number of siblings and quality of life (p = .001) and the number of family members and quality of life (p = .019). Children who had a smaller number of family members and no siblings had a higher mean score of quality of life.
Clinical Profile of Diabetic Children
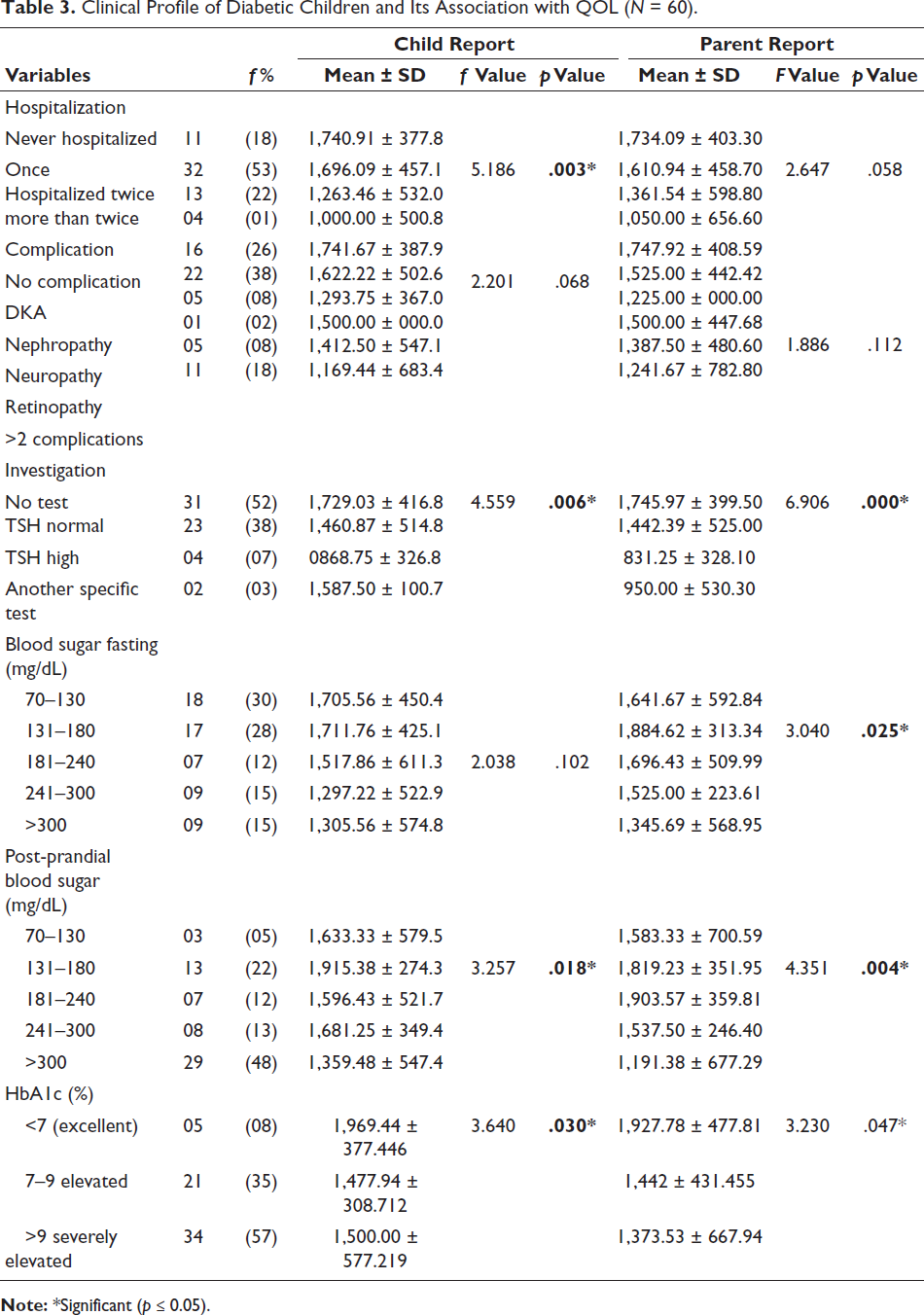
Most of the diabetic children (65%) were admitted once to the hospital, followed by 27% who were admitted twice. Nearly 8% of diabetic children were admitted more than two times to the hospital. As per blood sugar, fasting blood sugar was normal in less than one-third (30%), while post-prandial blood sugar was elevated in nearly half (48%) of diabetic children. As per spot urine albumin level, the majority of diabetic children (96%) had normal urine albumin levels, while 4% were positive. As per serum creatinine level, three-fourths (73%) of the children had normal levels, while slightly more than one-fourth had elevated levels, at almost 26%. As per TSH level, the majority (85%) of children had levels within the normal range. As per treatment, slightly less than half (42%) of the children were taking long-acting insulin. More than half (57%) of the children had severely elevated HbA1c levels (>9%), followed by 35% of children with moderately elevated HbA1c levels (7%–9%), and only 8% of the children had normal HbA1c levels (<7%).
Association of Quality of Life of Diabetic Children with Clinical Profile
As per the children’s report: A statistically significant association was found between quality of life and history of hospitalization (p = .003), number of investigations (p = .06), post-prandial blood sugar level (p = .018), and HbA1c level (p = .03). Whereas as per the parents’ report, the weight of the child (p = .027), investigations done (p = .01), fasting (p = .025), and post-prandial blood sugar level (p = .004) were significantly associated with quality of life (Table 3).
Clinical Profile of Diabetic Children and Its Association with QOL (N = 60).
Quality of Life of the Children
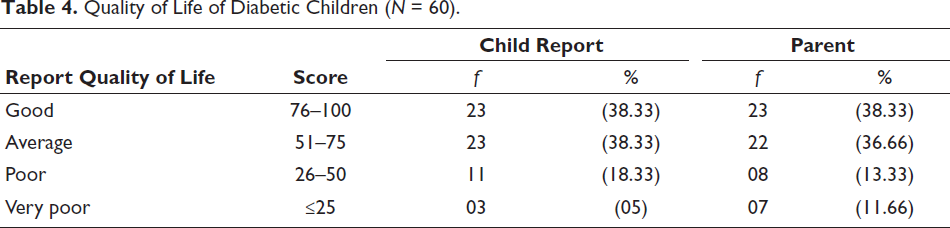
Almost an equal proportion (38%) of children had a good to average quality of life as per children’s self-report and parent proxy report. In addition, 5% of children reported a very poor quality of life and, according to parents, only 2% of children had a very poor quality of life (Table 4).
Quality of Life of Diabetic Children (N = 60).
Domain-wise Quality of Life of Diabetic Children
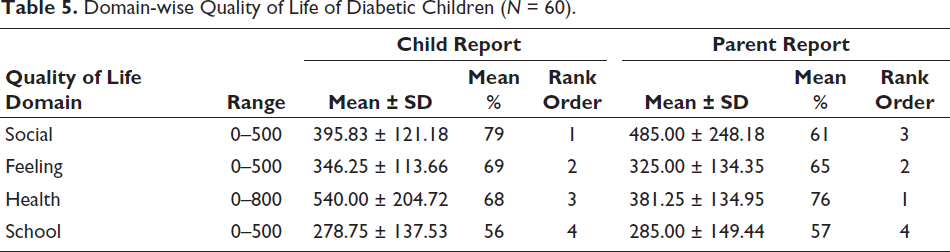
As per children’s self-report, the social domain’s quality of life was good as compared to other domains, with a mean percentage of 79%, but according to parents’ report, the quality of life was good as compared to other domains. The school life of children was the most affected domain with a mean percentage of 57% (Table 5).
Domain-wise Quality of Life of Diabetic Children (N = 60).
Lived Experiences of Mothers of Diabetic Children
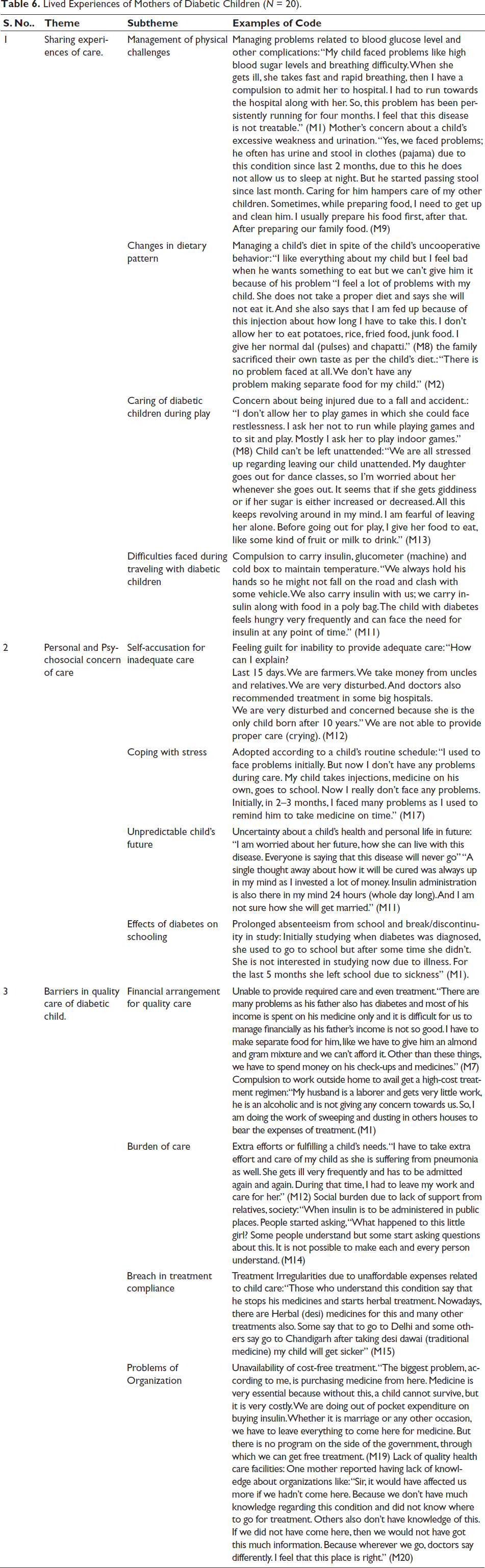
Most of the mothers shared experiences regarding the care of their diabetic children, which included management of the physical challenges of the child, care of diabetic children during play, and changes in the dietary patterns of children as well as those of the whole family. Along with the maternal role, these mothers consequently had a caregiver’s role. Along with this, mothers of diabetic children, as well as their family members, faced various kinds of personal, school, social, and psychosocial issues, which is a matter of concern. Due to the illness and financial reasons, there were often breaches in the treatment of these children; it was also highlighted by mothers that this breach was mainly due to the high cost of treatment and lack of support from the government. The detailed verbatim of mothers is presented in Table 6.
Lived Experiences of Mothers of Diabetic Children (N = 20).
Final Conclusion of Both Strands
Data presented in Table 7 compares the findings of both qualitative and quantitative data of the study.
Final Conclusion of the Qualitative and Quantitative Data.
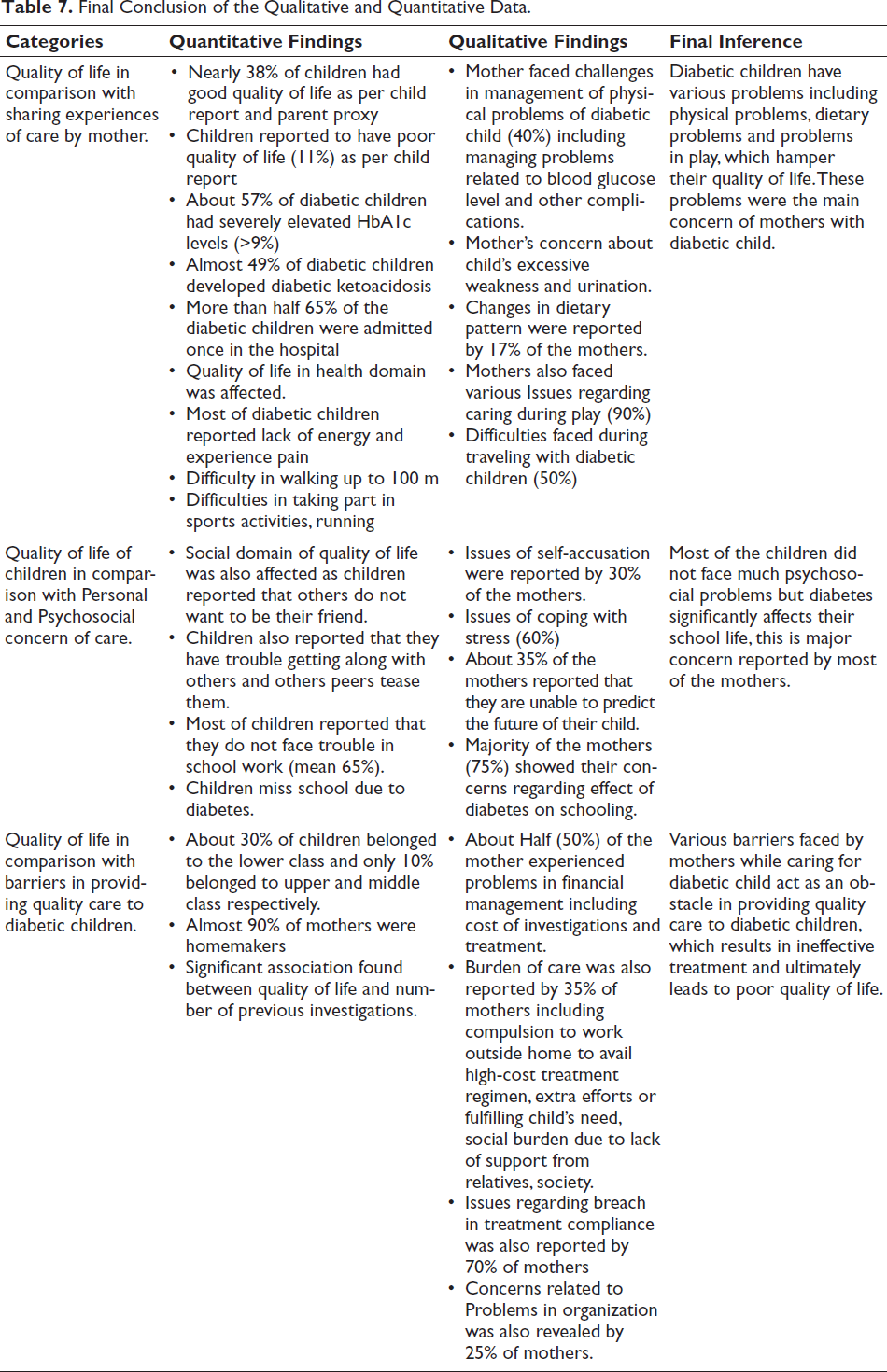
Quality of Life in Comparison with Sharing Experiences of Care by Mother
Quality of life of children in the health domain was directly affected, as quantitative findings showed an increase in about 57% of diabetic children who had severely elevated HbA1c levels (>9%) and difficulty in walking 100 m, and their mothers were directly affected as they faced challenges in the management of physical problems of diabetic children (40%), including managing problems related to blood glucose levels and being concerned about the child’s excessive weakness and urination.
Quality of Life of Children in Comparison with Personal and Psychosocial Concern of Care
Social domain of quality of life was also affected, as children reported that others did not want to be their friends and peers teased them and missed school due to sickness, but 65% reported that they did not face trouble with schoolwork. In the qualitative findings, the majority of the mothers (75%) showed their concerns regarding the effect of diabetes on schooling, uncertainty about the child’s future, and self-accusation for the child’s health deterioration.
Quality of Life in Comparison with Barriers in Providing Quality Care to Diabetic Children
The majority of the children’s families were from a lower economic status, which led to problems in managing the cost of investigation and treatment. Barriers faced by mothers, such as compulsion to work outside the home to avail the high-cost treatment regimen, extra efforts in fulfilling the child’s needs, and the social burden due to lack of support from relatives and society, resulted in ineffective treatment and ultimately led to poor quality of life.
Discussion
Children with type 1 diabetes face many challenges in their day-to-day lives due to complications and the complexity of their treatment. Hence, type 1 diabetes has a direct impact on the quality of life of children. The clinical parameters have a direct effect on the quality of life. This study showed that HbA1c is significantly associated with the quality of life of children as reported by both children and their parents. Children who have HbA1c levels ≥7 had a good quality of life. Fasting as well as post-prandial blood sugar levels of children with type 1 diabetes were associated with quality of life. Similarly, Ausli et al. reported that HbA1c has a direct effect on health-related quality of life and glycemic control was significantly associated with better quality of life (p < .01). 21 Nansel et al. also reported that diabetic specific quality of life was associated with HbA1c level. A significant association was found between the number of family members, the number of siblings, and the quality of life of children in this study (p > .05). Studies also reported that parents’ educational status was significantly associated with quality of life (p = .02). 17 Özyazıcıoğlu et al. also reported that the educational status of parents has a direct effect on the quality of life of children, and the number of siblings had a negative effect on the quality of life of children (p > .05). 22
Good quality of life among type 1 diabetic children was reported by 38% of diabetic children and their parents. In contrast to this, Özyazıcıoğlu et al. stated that children had a good score (79.91) on the PedsQL tool, which denoted that they had a good quality of life. 19 Petersson et al. in their study revealed that there was a direct impact of comorbidities on health-related quality of life, but in the present study, no such association was found (p = .068). 23
In the present study, it was found that the mean score of quality of life was high in the social domain (395.83 ± 121.18) and feeling domain (346.25 ± 113.66) but low in the health-related domain (278.75 ± 137.53). Similarly, Emmanouilidou et al. (2017) stated that the mean scores of the social domain and affective domain related quality of life, was good. 24 Abdul et al. found that scores of school function (73.5) were lowest as compared to other domains, and these results are in congruence with those of this study. 25
Lived Experience of Mothers with Diabetic Children
This study revealed that mothers of children with type 1 diabetes face several problems and challenges while caring for their children in their day-to-day lives. Various themes and subthemes emerged from this qualitative approach. Most of the mothers reported that they have difficulties in managing the physical problems of their children, financial crisis, and sending their children to school. Along with this, they face various personal and psychosocial problems.
Schmidt conducted a survey on type 1 diabetes and found that mothers reported that their children were having problems maintaining adequate dietary regimens and faced problems while handling high blood glucose levels. 26
Family members also showed special concern for their child during play as one of the mothers stated “I don’t allow her to play games in which she could face restlessness. I ask her not to run while playing games; sit and play, and mostly, I ask her to play indoor games.”
Khandan et al. documented similar findings in which they stated that mothers have to deal with various complications, such as increased blood sugar levels and recurrent hospitalization, while caring for their children. 13
Déa et al., in their article on the experiences of mothers with diabetic children, documented that mothers face various problems while caring for their diabetic children. Likewise, in this study, one mother said, “I felt bad, very bad, because she was very young and I knew how much she was going to suffer, especially during the administration of injection insulin. I cried a lot.” 27 The school life of children is also affected, as one mother said, “Now due to illness, she is not interested in study and from last 5 months she has left the school.”
Mothers often go through financial crises and thus are unable to ensure proper treatment for their children, which makes them feel guilty. Some mothers experience a very stressful life as they have to bear all the expenses of treatment alone, which places a severe burden of care on them. One of the mothers while explaining her financial problems said, “We spent almost 5.5 lakh rupees on his treatment; we went everywhere then was referred here and here also we spent a lot, underwent many expensive private investigations of even 8–9 thousand.” (M5)
Mothers have to make extra efforts while caring for their diabetic children when compared to other children. One of the mothers stated, “Extra effort and special care is needed during her play; while making food, we have to make separate food for her.” (M15)
One mother explained, “I didn’t inform anyone around our neighborhood of her problem because people talk nonsense. She will not get married.” (M16)
Iversen et al (2018) also classified the issues faced by mothers of diabetic children as similar themes, like diabetes’s life-changing situation, always being vigilant, difficulties in going somewhere. These themes are demonstrated in various speeches, like “I really think about this all the time, in the way that I must always be available on phone calls from the kindergarten.” 28
Final Conclusion of the Qualitative and Quantitative Data
Quality of life of children in the health domain was directly affected, as quantitative findings depict an increase of about 57% of diabetic children who had severely elevated HbA1c levels (>9%) and difficulty in walking 100 m. My child faced problems like high blood sugar level and breathing difficulty. When she got ill, she takes fast and rapid breathing then I have compulsion to admit her in hospital. (M1)
Yes, we faced problem, he often passed urine and stool in clothes (pajama) due to this condition since last 2 months. (M9)
Social domain of quality of life was also affected, as children reported that others do not want to be their friends and peers tease them and that they missed school due to sickness, but 65% reported that they do not face trouble with schoolwork. In the qualitative findings, the majority of the mothers (75%) showed their concerns regarding the effect of diabetes on schooling, uncertainty about the child’s future and self-accusation for the child’s health deterioration. Abolhassani also identified that mothers lived with uncertainty and fear regarding their child’s future. 29
Mothers of diabetic children also faced problems related to the unavailability of cost-free treatment and had to resort to out-of-pocket expenditures as mothers reported, “treatment of diabetes is very costly, and there is no facility or solution regarding diabetes.” (M7).
There is a need for collaboration between family members and healthcare providers (multidisciplinary team) to decrease some burdens from the mother’s shoulders. The present study depicts not only the unique relationship of the mother and child but also highlights the difficulties and issues that mothers face in their day-to-day lives while caring for their children. These challenges and issues somehow affect the quality of life of these children.
Limitations of the Study
The findings of this study may have limited generalizability because of the small sample size, geographical location, and unique context. Also, the time duration after the diagnosis ranged from 6 months to more than 10 years, and this could be considered a potential for recollection bias as memories can be impacted by the passage of time.
Conclusion
In this study, it was found that a majority of children diagnosed with type 1 diabetes had a good quality of life, as per diabetic children’s self-reports and parents’ proxy reports. Clinical parameters like elevated HbA1c and blood sugar levels directly affected the quality of life of children. The quality of life was good in the social domain in comparison to other domains. In addition, it was found that the mothers of diabetic children faced various challenges while caring for their children. They faced challenges while managing physical symptoms, were concerned for their child’s future, dealt with personal and psychosocial issues, and encountered financial burdens. Therefore, by identifying these experiences and challenges, we can conclude that mothers of diabetic children need a unique and flexible program on diabetes management.
Footnotes
Acknowledgements
Hospitals included were All India Institute of Medical Sciences, Rishikesh (AIIMS); SPS Government Hospital, Rishikesh; Shri Mahant Indresh Hospital, Dehradun; and Ramakrishna Mission Hospital, Haridwar.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Permission was obtained from selected hospitals and Institute Ethical Committee. Informed consent and assent were taken from participants of the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.