
Abstract
Objective:
To analyse the structural and clinical shifts in surgical activities within a high-volume gynaecological department in Kharkiv, operating under frontline conditions during the full-scale war (2020–2025).
Material and Methods:
This is a retrospective clinical analysis of a database comprising 5,115 recorded operations. The study compares pre-war baseline activity (2020–2021) with wartime activities (2022–2025). Key variables included surgical access (minor, laparoscopic, vaginal, laparotomy), diagnostic profiles, patient age, and somatic comorbidities.
Results:
Total surgical volume nearly doubled during the conflict, increasing from 605 procedures in 2021 to a peak of 1,329 in 2023. Endometrial pathology and abnormal uterine bleeding remained the primary drivers of admission, accounting for 52.6% of cases. ‘Minor’ diagnostic procedures (D&C, polypectomy) proved essential as an oncological filter; analysis revealed that many verified endometrial adenocarcinomas (G1-G3) were postoperatively identified in cases initially presenting with benign findings like polyps or hyperplasia. Reconstructive vaginal surgery for pelvic organ prolapse (POP) saw a dramatic five-fold increase, rising from 20 cases in 2020 to consistently over 100 cases annually by 2023–2025. The patient demographic shifted significantly toward a geriatric population, with an average age peaking at 64.7 years in 2024 and successful interventions performed on patients up to 89 years of age.
Conclusion:
The Kharkiv Municipal Perinatal Centre successfully adapted to frontline pressures by transitioning into a specialised high-intensity centre. The facility prioritises minimally invasive reconstructive surgery and early oncology detection for an ageing, somatically burdened population, effectively evolving into a multidisciplinary surgical hub.
Keywords
Introduction
Changes in the wartime landscape induced a transformation of the health care system in Ukraine. Kharkiv is a frontline city from the very beginning of the Russian invasion. The wartime stress and environmental pollution caused a considerable shift in female reproductive system disorders.[1] The accessibility of gynaecological care in the area of armed conflict is a challenge for the population. However, recent studies demonstrated obvious progress in the field. Pelvic gynaecological surgery in Ukraine is evolving under the dual pressures of war and modernisation. This branch of gynaecology is undergoing rapid transformation, shaped by global surgical advances and the profound disruptions of war. Key themes include modernisation of technology, a heavy burden of benign and malignant pelvic disease, high complication and infection rates, and an increasing emphasis on fertility preservation and complex oncologic care.[2,3]
Minimally invasive technologies are increasingly adopted across Ukrainian hospitals because of lower complication rates, faster recovery, and better cost-effectiveness.[4] However, heterogeneous generations of laparoscopic equipment and a lack of standardised indications and contraindications create risks of diagnostic and technical errors. International studies show that laparoscopic and robot-assisted approaches in gynecologic oncology can safely enable fertility-sparing procedures and reduce morbidity in carefully selected patients.[5] For Ukraine, progressive integration of advanced laparoscopy and, where feasible, robotics into oncologic and benign pelvic surgery is a clear direction, contingent on investment, training, and protocol development.
The full-scale invasion has dramatically disrupted surgical services. The problem of internally displaced persons is very significant. Within Ukraine, western and high-volume referral centres have absorbed large numbers of patients from combat regions, reconfiguring case-mix and stretching surgical capacity.[6] These dynamics both expose vulnerabilities and create opportunities for sustained international partnerships, protocol harmonisation, and shared training.
Qualitative work on Ukrainian surgical education highlights resilience but also major structural weaknesses: limited operative exposure, unstructured didactics, insufficient simulation, and gender discrimination, all exacerbated by wartime conditions.[7] These deficits directly affect the ability to safely deliver complex pelvic gynecologic surgery, especially minimally invasive and reconstructive procedures. Strengthening residency curricula, mentorship, and international collaborations will be crucial for post-war recovery and modernisation.
Global trends emphasise preserving reproductive potential in both benign and malignant gynecologic diseases. FIGO guidance and major reviews recommend tailored, fertility-sparing surgery for conditions such as pregnancy loss, fibroids, endometriosis, hydrosalpinx, and adenomyosis, with routine use of adhesion-reduction strategies and cautious tissue handling.[8] The current epidemiological studies revealed the heavy case-mix (endometriosis, fibroids, cancer), and relatively high complication and infection rates.[9] Therefore, the following progress depends on modernising equipment, standardising perioperative and infection-control protocols, strengthening oncologic and fertility-sparing pathways, and deeply reforming surgical education and system organisation during and after the war.
The study was focused on the trends and variables of surgical activities of the gynaecological department of Kharkiv Perinatal Centre.
Material and Methods
This study was a retrospective clinical analysis of surgical activities and diagnostic variables within the gynaecological department of the Kharkiv Perinatal Centre. The study covers 6 years from 1 January 2020 to 3 December 2025, encompassing 5,588 pro-treated patients. All women included in the research were divided into clinical groups according to the year of treatment. A total of 619 patients were included in Group I (treated surgically in 2020). There were 605 women in Group II (2021). There were 718 women in Group III (2022). There were 1,522 patients in Group IV (2023). Group V (2024) combined 1,122 observations of operated women. Group VI (2025) included 1,002 patients.
Data Collection and Source
Material Data were extracted from specialised clinical registries, including surgical intervention logs, pathohistological report registers, and comprehensive patient discharge records. All available data from the hospital automated system were analysed, including passport, anamnesis, objective examination, instrumental and laboratory indicators, surgical interventions, and results of pathomorphological studies. The longitudinal nature of the database allowed for a comparative analysis between the pre-war baseline period (2020–2021) and the wartime period (2022–2025), during which Kharkiv operated as a frontline city.
Study Population and Demographic Variables
The study cohort included all women admitted for elective and emergency gynaecological surgical care. Key variables recorded for each patient included:
Age: With a specific focus on the growing geriatric population (up to 89 years of age).
Body mass index (BMI): High-risk patients with Class III obesity (BMI ≥ 40 kg/m²) were specifically monitored due to their surgical complexity.
Comorbidities: Primary focus was placed on cardiovascular diseases (hypertension, ischaemic heart disease), metabolic disorders (Type 2 diabetes), and secondary conditions such as anaemia.
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS for Windows version 25.0, Chicago, Illinois, USA). Fisher’s exact test (for 2 × 2 tables only) was used as a significance test for qualitative data. A P value of <.05 was considered statistically significant.
Results
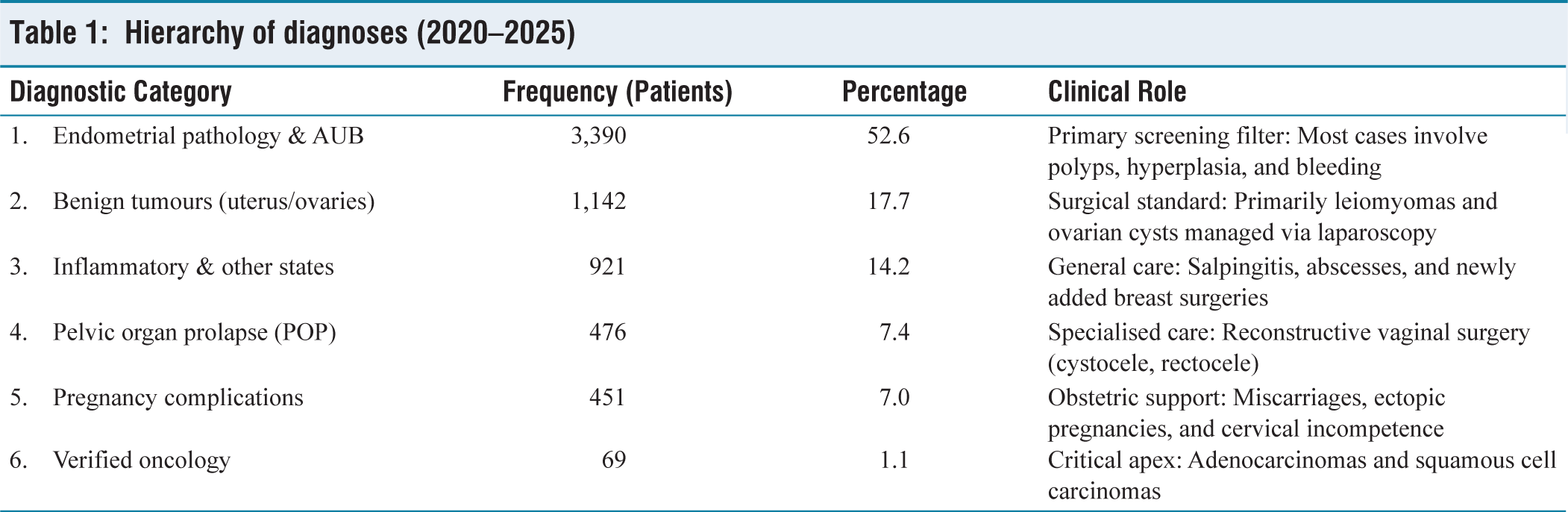
The structure of gynaecological diagnoses is presented in Table 1. It follows a ‘Broad Pyramid’ model [Figure 1]. At its base are high-volume diagnostic and screening cases, while the apex consists of rare but critical oncological conditions. In the meantime, there is a structural breakdown based on the 5,588 patients treated during this period.
Hierarchy of diagnoses (2020–2025)
Visual representation (ASCII diagram)
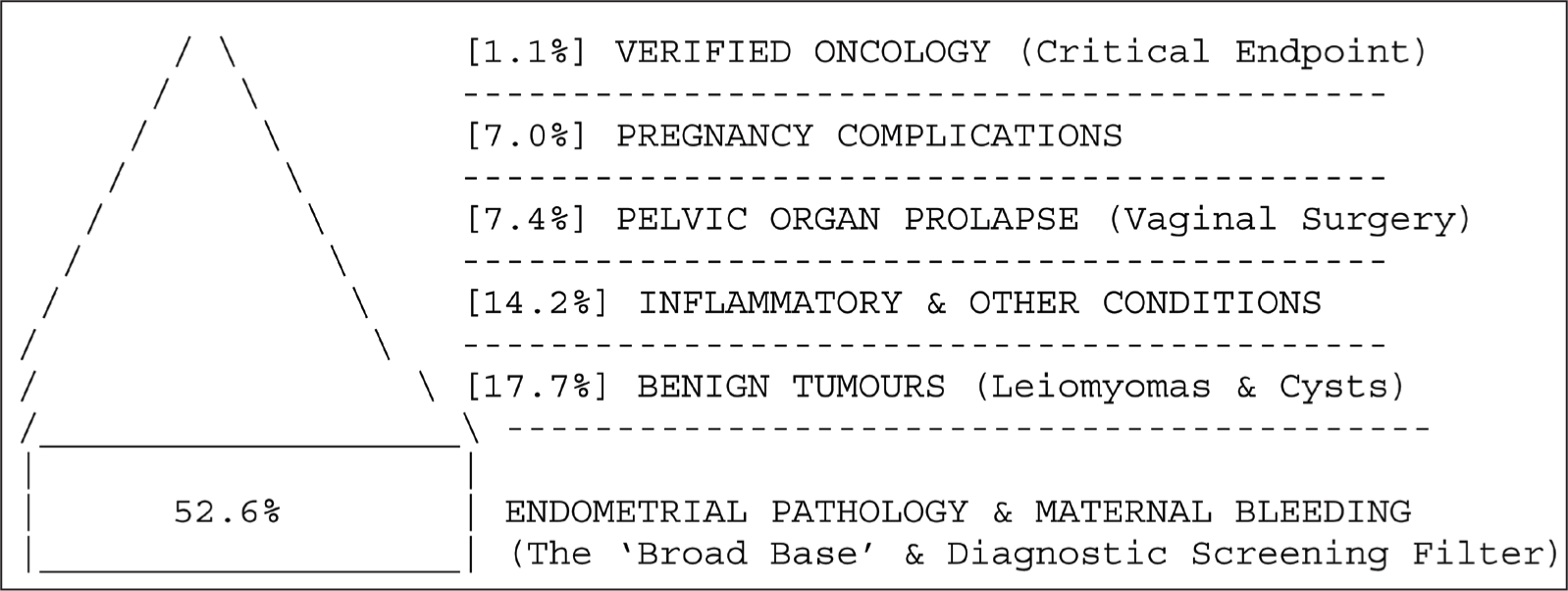
Key Insights into the structure:
The screening filter: Over half of all patients (52.6%) enter the department due to endometrial issues. As noted in the registries, many of these ‘minor’ cases (polyps/hyperplasia) eventually lead to the detection of the small percentage (1.1%) of hidden cancers. Surgical specialisation: Categories 2 and 4 (Benign Tumours and pelvic organ prolapse [POP]) represent the technological core of the facility, focusing on laparoscopy and reconstructive vaginal procedures. Wartime shift: The structure has become ‘older’ at the base, with a significant increase in the volume of geriatric patients presenting with both Category 1 (bleeding) and Category 4 (prolapse) diagnoses concurrently.
Based on the surgical and clinical records from 2020 to 2025, the diagnostic structure is categorised by the primary clinical profile and the corresponding surgical intervention. The following tables reflect the number of cases and their percentage relative to the total number of patients treated (‘Base’) for each year.
Diagnostic Structure by Year (2020–2025)
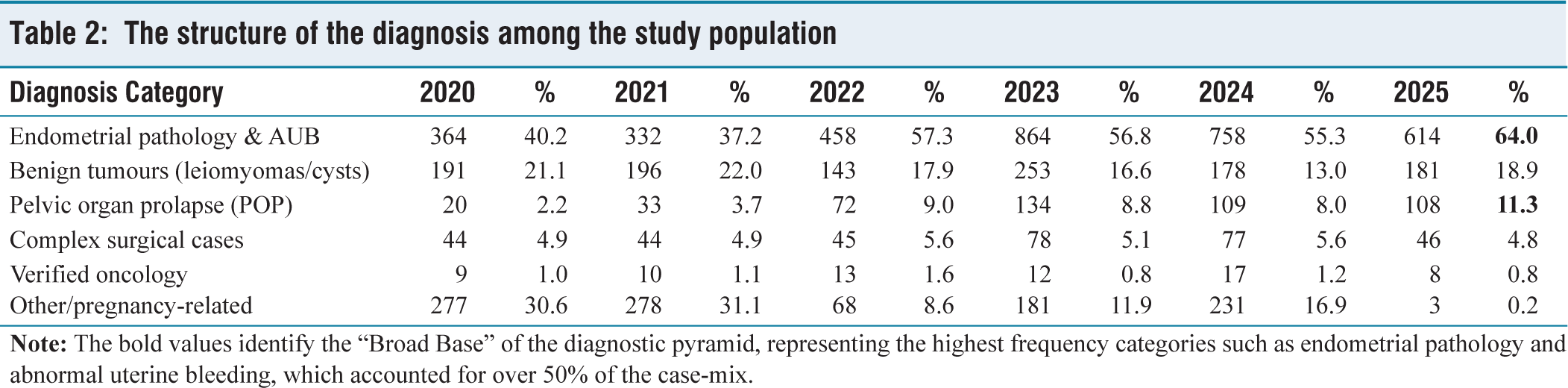
2020–2021: Baseline Period: During these years, the department handled a stable volume of general gynaecological cases with a focus on endometrial diagnostics and laparoscopic treatment of benign tumours [Table 2]. 2022–2023: Growth and Scaling. The year 2022 saw the beginning of a significant shift toward reconstructive vaginal surgery, while 2023 marked the peak of surgical intensity with over 1,300 operations performed. 2024–2025: Specialisation and Modern Trends. The current period shows a high reliance on ‘Minor’ diagnostic interventions (reaching 64% in 2025) and a steady increase in reconstructive procedures for the ageing patient population.
The structure of the diagnosis among the study population
Based on the analysed data, the facility has undergone a significant transformation in its surgical volume and the complexity of cases it manages, particularly during the years of the full-scale war [Table 3]. The structural data shows a clear shift from general gynaecological care toward a high-intensity centre specialising in reconstructive surgery and early oncology detection.
Surgical interventions by type and year (Abs. and %)
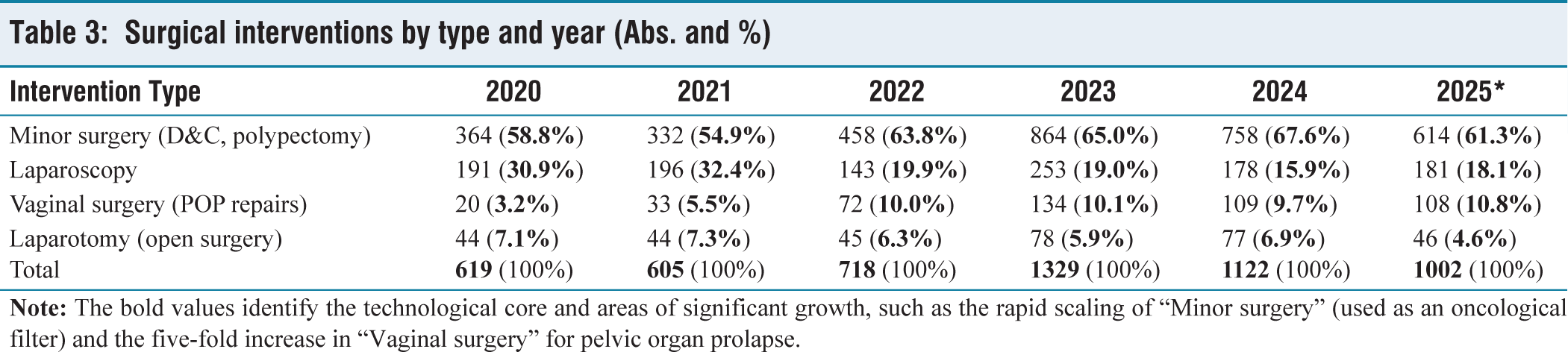
The data showed a major scaling of vaginal surgeries (POP repairs) as the facility expanded its specialised care [Table 4]. We compared the earliest stable year (2020) to the peak of surgical intensity (2023). The two-tailed P value was <.0001. The increase in the proportion of vaginal surgeries (from 3.2% to 10.1%) was extremely statistically significant. This confirms a fundamental shift in the department’s clinical profile toward reconstructive urogynecology. During the war years, the reliance on minor surgeries (dilatation and curettage [D&C], polypectomy) as a screening tool increased. We compared the pre-war baseline (2021) to the highest recorded proportion (2024) [Table 4]. The two-tailed P value was <.0001. The increase in the proportion of minor interventions (from 54.9% to 67.6%) was extremely statistically significant. Fisher’s test evaluated whether the facility successfully maintained its move toward minimally invasive laparoscopy over traditional open surgery (laparotomy) despite the added complexity of wartime geriatric patients [Table 4]. The two-tailed P value was .8143. The result was not statistically significant. While the total volume of surgeries increased, the ratio between open surgery and laparoscopic access remained stable (18.7% laparotomy in 2020 vs. 20.2% in 2025). This indicated that despite an ageing population with more complex pathologies, the department successfully preserved its high-tech standard for benign tumour treatment without regressing to more invasive open procedures.
Summary of Fisher’s exact test results

Discussion
Main Changes During the War (Post-February 2022). The most striking changes in the facility’s operations occurred from late 2022 through 2025, reflecting broader social and demographic shifts caused by the war.
Doubling of Surgical Intensity
The most immediate change was the massive scaling of activity. Total operations rose from 605 in 2021 to a peak of 1,329 in 2023. This indicates that the facility became a critical hub for gynaecological care as other medical resources may have been redirected or displaced.
The Ageing ‘Geriatric’ Patient Profile
During the war years, the average age of patients trended upward, peaking at 64.7 years in 2024 [Model History]. The registers show a high volume of patients aged 75–89. This shift suggests that older women, who remained in the region or were displaced to it, required urgent care for conditions like postmenopausal bleeding and advanced prolapse.
Increased Clinical Complexity and Comorbidity
The wartime cohort presents with significantly higher levels of comorbidity. Surgeons are increasingly operating on patients with severe obesity (BMI ≥ 40 kg/m²), advanced cardiovascular disease (hypertension, heart failure, and previous strokes), and Type 2 diabetes with complications.
Expansion into Multidisciplinary Care (Breast Surgery)
A major development in 2024 and 2025 is the integration of breast cancer surgery. The facility expanded its scope to include radical mastectomies (e.g., Madden technique) and sectoral resections. This suggests a move toward providing comprehensive ‘one-stop’ surgical care for female patients facing multiple oncological or surgical risks.
Emergence of Stress-related and Rare Cases
The records from the war period include unique or rare cases, such as bowel resections performed during complex pelvic surgeries and patients presenting with conditions potentially exacerbated by stress or lack of regular screening, such as advanced prolapse and ‘hidden’ cancers.[10] Modern pelvic surgery is currently undergoing a transformative period characterised by a shift toward minimally invasive techniques, an increasing focus on reconstructive vaginal surgery, and the management of an ageing patient population with significant somatic burden.
The data revealed a dramatic scaling of surgical activity, with total interventions nearly doubling from 605 in 2021 to a peak of 1,329 in 2023. The primary driver of this volume was endometrial pathology, which accounted for over half of all admissions (52.6%). These ‘minor’ diagnostic procedures, such as D&C and hysteroscopic polypectomy, serve as a critical oncological filter; records indicate that nearly 75% of verified malignancies, primarily endometrial adenocarcinomas, were initially masked as benign conditions like polyps or hyperplasia.[11] Parallel to diagnostic screening, there is a clear trend toward technological specialisation.[12–14] Finally, the impact of the war has necessitated a broadening of the surgical scope: significant growth in surgical volume; shift toward reconstructive and vaginal surgery; and managing the high-risk geriatric patient.
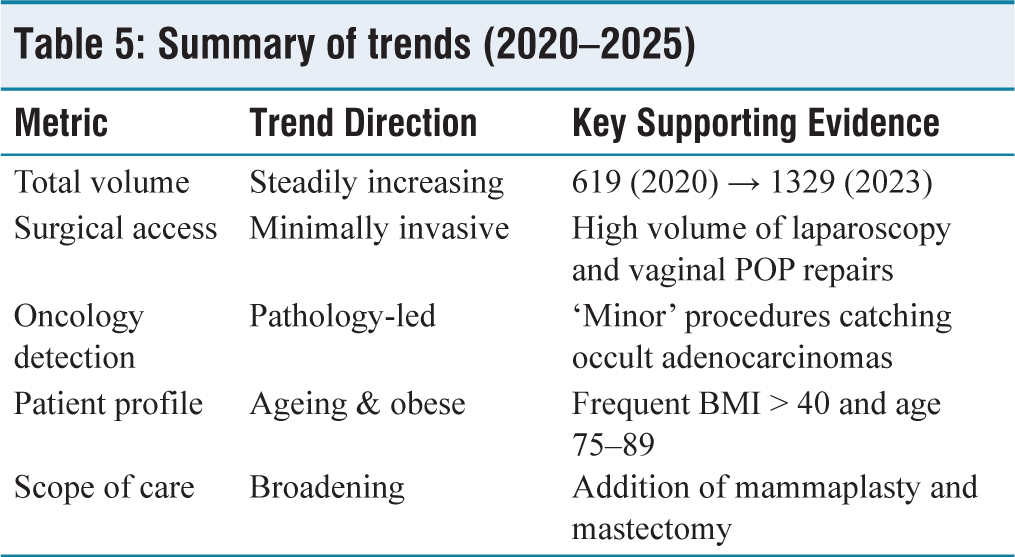
Summary of Trends (2020–2025). Pelvic gynaecological surgery in Ukraine is evolving under the dual pressures of war and modernisation. Key trends include rising use of minimally invasive techniques, high complication burdens, and strong emphasis on fertility preservation and oncologic care [Table 5]. The main trend in the field was for the evolution of specialised surgical care under extreme regional and demographic pressure.
Summary of trends (2020–2025)
Conclusion
The war transformed the facility from a standard gynaecological department into a high-volume specialised centre managing a significantly older, more physically fragile population with a broader range of surgical needs (including breast surgery) and a massive reliance on minimally invasive vaginal and laparoscopic techniques to ensure rapid recovery. The resilience of the Kharkiv Perinatal Centre is demonstrated by its ability to adapt to frontline pressures by providing high-tech, minimally invasive, and life-saving oncological care to a physically fragile and ageing population. This retrospective analysis provides a clinical blueprint for the survival and specialisation of surgical services in regions affected by active military conflict and demographic shifts.
Footnotes
Acknowledgements
The authors appreciate the help of the staff of Kharkiv Municipal Perinatal Centre.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical approval was required and obtained for this research from the Research Council and Ethical Committee of Kharkiv National Medical University, approval number No. 54.0925p.
Informed consent
Informed consent was required and obtained from all patients included in the study for the use and publication of their data.
Credit author statement
IL created a design of the research, compiled the material, analysed the obtained data, wrote and revised the manuscript.
SK compiled the material and analysed the obtained data.
OR analysed the obtained data and revised the manuscript.
AR compiled the material and analysed the obtained data.
MCh analysed the obtained data and revised the manuscript.
AH analysed the obtained data, wrote and revised the manuscript.
YuA compiled the material and analysed the obtained data.
Data availability statement
Available from Igor Lakhno.
Use of artificial intelligence
N/Y.