
Abstract
Introduction:
Scrub typhus (ST), a re-emerging vector-borne disease caused by Orientia tsutsugamushi (O. tsutsugamushi), is an important cause of acute febrile illness in India. Clinical features are often non-specific, and eschar is infrequently detected, making laboratory confirmation essential. As background seroprevalence and antigenic variability differ regionally, this study aimed to define an appropriate immunoglobulin M (IgM) enzyme-linked immunosorbent assay (ELISA) cut-off for accurate diagnosis.
Results:
ROC analysis demonstrated excellent diagnostic performance with an area under the curve (AUC) of 0.954 (95% CI: 0.935–0.969; P < .0001). An OD cut-off value of >0.4854, derived using the Youden index, yielded a sensitivity of 98.65% and a specificity of 93.2%. No false positives were observed among healthy controls, while limited cross-reactivity (6.8%) was noted among controls, particularly dengue and other acute undifferentiated febrile illness groups.
Conclusion:
A region-specific ST IgM ELISA cut-off OD value of >0.4854 provides excellent diagnostic accuracy in our setting, ensuring maximal case detection with acceptable false-positive rates in this high-prevalence setting. Adoption of this optimised threshold can improve clinical decision-making and early institution of appropriate therapy in endemic areas.
Keywords
Introduction
Scrub typhus (ST) is a re-emerging vector-borne disease caused by Orientia tsutsugamushi (O. tsutsugamushi).[1] Previously, it was confined to endemic areas such as South Asia, Southeast Asia, East Asia, the Pacific Islands and Northern Australia, collectively known as the ‘tsutsugamushi triangle’. However, it is no longer restricted to this region and is increasingly being reported throughout India, accounting for 30%–40% of all acute febrile illnesses requiring hospitalisation.[2] ST often presents with indeterminate symptoms, making clinical diagnosis extremely challenging. The presence of eschar is pathognomonic; its prevalence ranges from 7% to 80% of cases.[1,3] Its clinical manifestations range from mild illness to life-threatening disease, with an increasing mortality rate of 50% in the absence of appropriate treatment.[4] Studies recorded that ST is an important cause of acute encephalitis syndrome, acute febrile illness, acute respiratory distress syndrome and acute kidney injury from different geographical locations.[5,6] Although the immunofluorescence assay is the gold standard method in the diagnosis of ST, we still rely on serological diagnosis by enzyme-linked immunosorbent assay (ELISA).[7] Geographic-based cut-off values for diagnosis are necessary due to the wide range of endemic patterns of the disease and antigenic variants observed in various regions of India.[8] This study aimed to determine a geographically appropriate IgM ELISA cut-off value for ST diagnosis in a district of Southern India using ROC curve analysis with a diverse control population, including healthy individuals and patients with potentially cross-reactive febrile illnesses.
Material and Methods
This cross-sectional study was conducted at the Microbiology Department of a tertiary care teaching hospital in Southern India between August 2024 and July 2025. The study protocol was approved by the Institutional Ethics Committee (Protocol ID: 20246971; dated 31 July 2024), and all procedures were performed in accordance with the Declaration of Helsinki. The minimum required sample size was estimated separately for cases and controls using standard formulas for diagnostic test evaluation, assuming an expected sensitivity and specificity of 95% for ST IgM ELISA, with a precision of 5% and a 95% confidence level; this yielded approximately 73 cases and 73 controls and to improve precision, enable subgroup analysis and account for exclusions, the sample size was increased to 370 cases and 250 controls.
Case Definition
An individual exhibiting a titer of ≥1:80 against the OXK antigen by the Weil-Felix test was defined as a probable case of ST. Whereas individuals who tested positive by IgM ELISA or real-time polymerase chan reaction (qRT-PCR) or both were considered as confirmed cases. Controls were individuals who tested negative for ST by both IgM ELISA and qRT-PCR.[9]
A total of 620 participants were included in the study, comprising:
Cases (n = 370): Based on the above case definition, individuals with clinical suspicion of ST presenting with acute fever (≥5 days duration) and at least two of the following: Severe headache, myalgia, maculopapular rash, lymphadenopathy or presence of eschar and individuals who tested positive by IgM were considered as confirmed cases. Consecutive eligible patients attending the medicine outpatient and inpatient departments were enrolled using a convenience sampling strategy.[10] Case selection bias may have arisen due to reliance on differential diagnosis, as patients presenting with similar clinical features of dengue, malaria, pneumonia, leptospirosis and typhoid may have been differentially investigated, leading to potential underdiagnosis or exclusion of ST cases. ELISA-based diagnosis of ST may introduce potential bias due to variability in antibody response, cross-reactivity and timing of sample collection.[11,12] Controls (n = 250): Healthy volunteers with no acute or chronic illness and negative anti-O. tsutsugamushi IgM ELISA results (n = 130), patients with chronic liver disease to assess non-specific reactivity (n = 20), dengue IgM-positive cases to evaluate serological cross-reactivity (n = 50) and patients with acute undifferentiated fever due to other confirmed etiologies (n = 50). These control groups were selected using purposive sampling.
Exclusion Criteria
Individuals with a previous history of head injury, hypertension requiring treatment, organophosphate or other poisoning, pregnancy, immunosuppressive therapy or those unwilling to provide informed consent were excluded.
After obtaining written informed consent, 3–5 mL of venous blood was collected aseptically from each participant. Serum was separated by centrifugation at 3,000 rpm for 10 minutes and stored at −20°C until testing. All samples were processed within 1 week of collection.
Serum samples were tested for anti-O. tsutsugamushi IgM antibodies using the ST IgM ELISA (lot No. EL 6164, InBios International, Inc., Seattle, USA). This kit employs a unique recombinant antigen mixture representing multiple strains of O. tsutsugamushi. The assay was performed according to the manufacturer’s instructions. Optical density (OD) values were measured at 450 nm using an ELISA reader, with results recorded to four decimal places. Positive and negative controls provided in the kit were included in each ELISA run, and only runs meeting acceptance criteria (controls within specified ranges) were considered valid.
Statistical analysis was performed using SPSS version 25.0 (International Business Machines (IBM) Statistical Package for the Social Sciences (SPSS) Inc., Chicago, IL, USA) and MedCalc Statistical Software version 22.009 (MedCalc Software Ltd., Ostend, Belgium). Descriptive statistics were calculated for demographic and clinical variables. Continuous variables were expressed as mean ± standard deviation or median (interquartile range) as appropriate. Categorical variables were presented as frequencies and percentages.
Receiver operating characteristic (ROC) curve analysis was performed to determine the optimal cut-off value for the IgM ELISA OD values. The area under the curve (AUC) was calculated with 95% confidence intervals. The optimal cut-off was determined using the Youden index (J = sensitivity + specificity − 1). Sensitivity, specificity, positive likelihood ratio (LR+) and negative likelihood ratio (LR−) were calculated with 95% confidence intervals for various cut-off values.
Positive and negative predictive values were calculated for the study prevalence. A P < .05 was considered statistically significant.
Results
The study included 620 participants with a mean age of 35.68 ± 16.18 years (range: 1–90 years). Among the 370 ST cases, 232 (62.7%) were male, and 138 (37.3%) were female. Eschar, the pathognomonic sign, was identified in only 29 of 370 cases (8.0%).
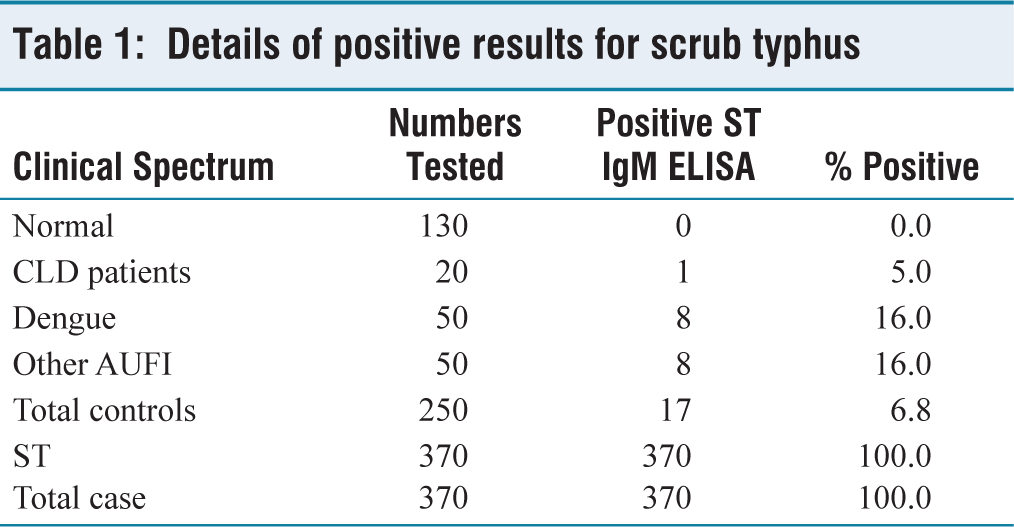
Among the 130 healthy controls, no false-positive results were observed, yielding a specificity of 100% in the healthy population. In contrast, cross-reactivity was detected among controls, with IgM ELISA positivity observed in 1 of 20 patients with chronic liver disease (5.0%), 8 of 50 dengue IgM-positive cases (16.0%) and 8 of 50 patients with acute undifferentiated fever of other etiologies (16.0%). Overall, 17 of 250 control participants (6.8%) demonstrated false-positive results [Table 1]. All 370 clinically suspected ST cases tested positive by IgM ELISA at the optimised cut-off, corresponding to a sensitivity of 98.65%.
Details of positive results for scrub typhus
Receiver Operating Characteristic Curve Analysis
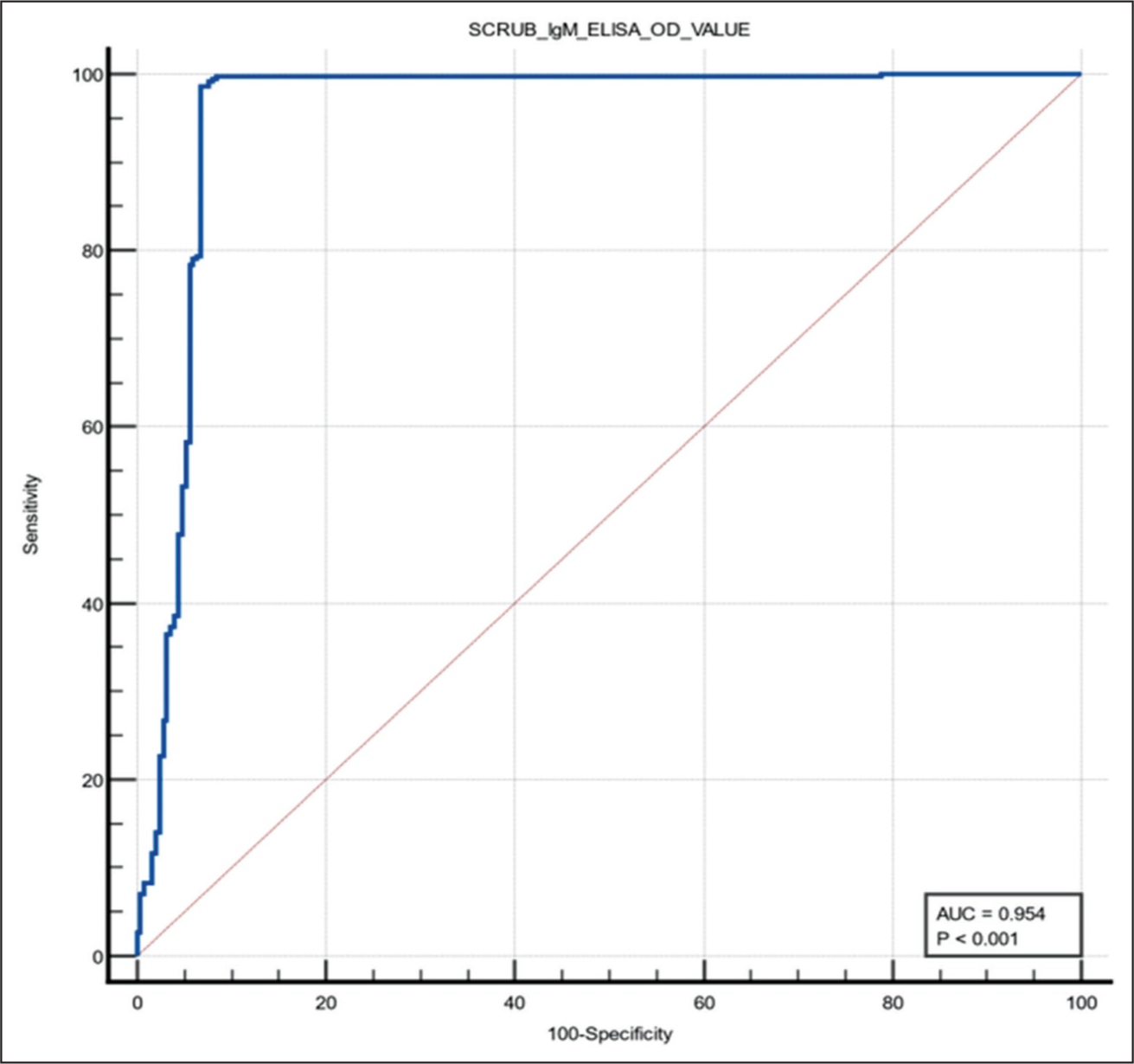
ROC curve analysis of the ST IgM ELISA, performed using the OD values from all 620 samples (370 cases and 250 controls), demonstrated excellent diagnostic performance with an AUC of 0.954 (95% CI: 0.935–0.969; P < .0001) [Figure 1]. Optimisation using the Youden index (J = 0.9185) identified an optimal OD cut-off value of >0.4854, which yielded a sensitivity of 98.65% and a specificity of 93.2% across a heterogeneous population comprising ST cases and diverse control groups (healthy individuals, chronic liver disease, dengue IgM-positive cases and other acute undifferentiated febrile illnesses).
Receiver operating characteristic curve for scrub typhus IgM ELISA. The ROC curve demonstrates excellent diagnostic performance with an AUC of 0.954 (95% CI: 0.935-0.969; P < .0001). The optimal cut-off value of >0.4854, determined using Youden index optimisation, is marked on the curve, achieving 98.65% sensitivity and 93.2% specificity
At the identified threshold, the assay demonstrated strong discriminatory power, with an LR+ of 14.51 (95% CI: 9.17–22.96) and an LR− of 0.014 (95% CI: 0.0061–0.035). At the observed study prevalence of 59.6%, the positive predictive value was 95.6%, while the negative predictive value was 100.0% [Tables 1 and 2].
Discussion
ST is showing a recent comeback in our country, as demonstrated by reports from different parts of India in the last two decades. A substantial index of suspicion is needed in individuals presenting with fever during the monsoon months.[13]
Though it is possible to cultivate O. tsutsugamushi from blood, it requires expertise and dedicated biosafety level 3 laboratory facilities.[14] Serological testing is the mainstay for diagnosing ST. The Weil-Felix test, one of the earliest and most affordable methods, is limited by low sensitivity and good specificity as observed by Sahu et al.[15] Other techniques, including passive hemagglutination, ELISA and indirect immunofluorescence antibody (IFA) assays, are employed to detect antibodies against O. tsutsugamushi.[16]
However, antibodies typically appear 1–2 weeks after infection; these tests have little therapeutic utility. A ≥4-fold increase in Ab titer is highly diagnostic; however, the possibility of false-positive results cannot be excluded in cases with a four-fold increase from a low titer. Additionally, it is clinically challenging to perform follow-up studies to assess Ab titers. Even if Ab titers are monitored, a ≥4-fold increase might not be demonstrated in individuals with high early titers.[17]
IgM ELISA seems to be a promising substitute technique for serological diagnosis with comparable sensitivity and specificity to IFA. It does not require technical know-how or costly equipment such as fluorescence microscopes, and it has no subjectivity problems. Regionally suitable cut-offs must be established, employing healthy volunteers.[7] But, ELISA is impacted by variables such as background antibody levels and strain makeup.[18]
The wide range of cut-off values reported across various regions of India (0.5–1.0) highlights the need to establish region-specific thresholds. These variations reflect differences in local seroprevalence and background immunity, circulating antigenic variants, co-endemic infections and various population demographics and risk factors.[8]
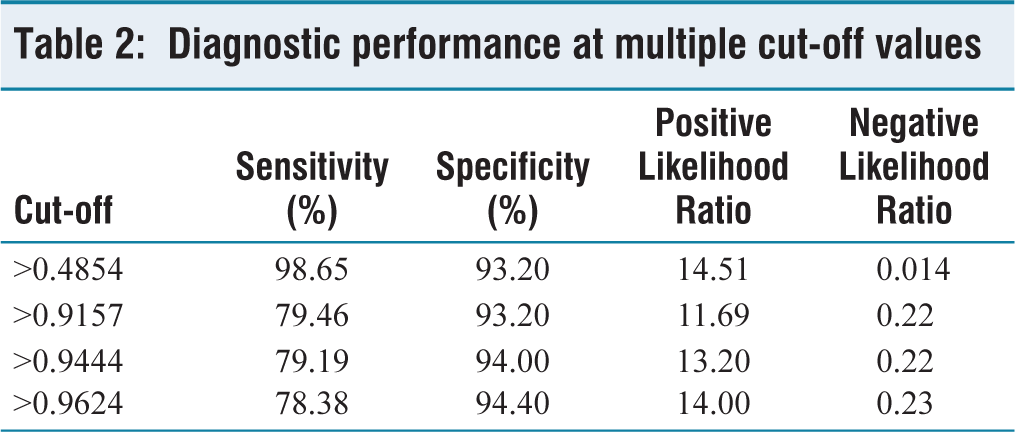
In this context, the present study derived a region-specific cut-off value of >0.4854 for ST IgM ELISA in our setting, demonstrating excellent diagnostic performance with an AUC of 0.954 and achieving 98.65% sensitivity with 93.2% specificity. This lower cut-off maximises case detection while keeping false-positive rates at a level that can be managed with careful clinical correlation. Based on the study by Elangovan et al., when the cut-off is raised above 0.9624, it significantly reduces the sensitivity (from 98.65% to 78.38%) while specificity remains stable or shows a marginal increase (from 93.20% to 94.40%). This indicates that higher cut-off values may miss true positive cases, whereas the present study achieves a better balance between sensitivity and specificity [Table 2].[2]
Diagnostic performance at multiple cut-off values
In comparison with other Indian studies, the identified cut-off of >0.4854 is significantly lower than the values reported in Thanjavur[13] (0.728) and Vellore[2] (1.0), both located in Tamil Nadu. In contrast, a pan-India cut-off study in 2023, based on multicentre data, proposed a cut-off of 0.554, which is closer to our findings.[5] This difference may reflect higher disease endemicity and background seroprevalence in our district, which has documented a high ST burden among acute febrile illnesses. The lower cut-off ensures maximum case detection in this high-prevalence setting, critical for timely initiation of appropriate antimicrobial therapy. The diagnostic performance observed in this study, including an AUC 0.962 comparable to that reported from the Thanjavur study using the same InBios kit, suggests that the assay performs consistently across different regions, while still requiring local calibration of the cut-off.[13]
Clinically, the low eschar prevalence of just 8% among confirmed cases in our study aligns with findings from other Indian research reporting rates of 8%–58%, emphasising that depending solely on this pathognomonic sign is unreliable, particularly in darker-skinned individuals and in patients presenting later in the disease course.[1] Every patient should be reexamined after all other causes of fever have been ruled out because eschar may have been missed during the initial examination.[6]
In the present study, the overall false-positive rate of 6.8% among control subjects, primarily due to reactivity in dengue and other acute undifferentiated febrile illnesses, mirrors previous findings where an 8% cross-reactivity was attributed to non-specific IgM binding.[11] These findings emphasise that serological results should be interpreted in conjunction with clinical features and epidemiological context, particularly in settings with multiple co-circulating febrile illnesses.
This study had several strengths, including a relatively large sample of 370 suspected ST cases and 250 controls drawn from both healthy individuals and clinically relevant disease groups, allowing assessment of background seroreactivity and potential cross-reactivity. Objective cut-off determination using ROC curve analysis and the Youden index, along with an excellent AUC, demonstrated strong discriminatory performance of the assay. However, the study has several limitations, including its single-centre tertiary care setting, which may restrict generalisability, the possibility of spectrum bias from convenience and purposive sampling and the cross-sectional design, which prevents assessment of antibody dynamics over time.
To conclude, the study suggests that implementing a region-specific IgM ELISA cut-off of >0.4854 in our setting can substantially enhance diagnostic accuracy for ST in routine practice, ensuring that potentially life-threatening infections are not missed while maintaining a manageable burden of false positives. These findings should be applied to other regions with caution and ideally validated through local studies. This approach supports broader adoption of geographically tailored thresholds rather than a single uniform value. Future work incorporating multi-centre recruitment and longitudinal follow-up of antibody kinetics would further refine these estimates and strengthen the evidence base for regional cut-off determination.
Footnotes
Acknowledgements
We sincerely thank and express our gratitude for the kind sponsorship and support provided for this study by The Tamil Nadu State Research Committee, King Institute of Preventive Medicine and Research, Guindy, Chennai, Tamil Nadu.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The Tamil Nadu State Research Committee, 05032/TNSRC/PCD/2024–2025, dated 21 January 2025.
Informed consent
Written informed consent was obtained from all the study participants.
Institutional ethical committee approval number
The study was approved by the Institutional Ethics Committee, Tirunelveli Medical College (Protocol ID: 2024/6971; Date of approval: 31 July 2024).
Credit author statement
Poongodi Santhana Kumarasamy: Concept and study design, supervision, data interpretation and critical revision of the manuscript.
Burle Gowtham: Methodology, data curation, statistical analysis, drafting of the manuscript.
Julie Jayachandra Baby Roselet: Patient recruitment, sample collection, data entry, literature review.
Abrar Muhammath: Patient recruitment, sample processing, assistance in data analysis and manuscript editing.
Data availability statement
De-identified individual participant data and the study dataset underlying the results will be made available from the corresponding author on reasonable request.
Use of artificial intelligence
The authors confirm that no artificial intelligence (AI)-assisted technology was used in the drafting, writing or editing of this manuscript, data analysis or image processing. No images were generated or manipulated using AI.