
Abstract
Background and Aims:
Adverse drug reactions (ADRs) are noxious and unintended responses occurring at normal therapeutic doses and remain a major cause of morbidity in hospitalised patients. Systematic evaluation of ADR patterns and causality is essential to strengthen pharmacovigilance and improve medication safety.
Objectives:
To evaluate the pattern and causality of ADRs reported in a quaternary care hospital; to compare causality assessment using the Naranjo algorithm and the WHO-UMC scale; and to identify commonly implicated drug classes and patient demographics.
Methods:
A retrospective observational study was conducted using ADR reports submitted to the Clinical Pharmacy Department of a quaternary care hospital in Navi Mumbai between January 2022 and December 2024. Data from 221 ADR reports were analysed for demographics, suspected drugs, route of administration, severity, outcomes and causality assessment. Descriptive statistics were used.
Results:
Of 221 ADRs, females were slightly more affected than males, and patients aged 41–60 years accounted for the largest proportion. Antibiotics were the most frequently implicated drug class, followed by iron preparations and antineoplastic agents. The intravenous route was most associated with ADRs. The WHO-UMC scale categorised most reactions as probable, whereas the Naranjo algorithm classified the majority as possible. Most patients recovered completely with supportive management; no mortality was reported.
Conclusion:
ADRs continue to be an important cause of morbidity in hospitalised patients. Antibiotics and parenteral iron formulations were the leading contributors. Differences between causality assessment tools underscore the need for improved documentation and harmonised evaluation to strengthen institutional pharmacovigilance.
Introduction
According to the World Health Organisation (WHO), an adverse drug reaction (ADR) is defined as ‘a response to a drug which is noxious and unintended, and which occurs at doses normally used in humans for the prophylaxis, diagnosis or therapy of disease or for the modification of physiological function’.[1] ADRs—unwanted and harmful responses to medications occurring at normal therapeutic doses—remain a significant concern in inpatient care and are associated with both direct patient harm and increased utilisation of healthcare resources.[2,3] Recent multicentre and population-based analyses indicate that a nontrivial proportion of urgent hospital admissions continues to be attributable to ADRs, with contemporary estimates often in the several-percent range depending on the population studied and the detection methods employed.[2,4]
In India, the expansion of the Pharmacovigilance Programme of India (PvPI) and the growth of designated ADR monitoring centres have strengthened reporting infrastructure; however, underreporting and variable data completeness persist as major challenges for accurate estimation of ADR burden and causality evaluation.[5] Hospital-based pharmacovigilance, therefore, remains vital for detecting local patterns, including commonly implicated drug classes and route-specific risks and for implementing targeted mitigation strategies such as antimicrobial stewardship and standardised protocols for parenteral therapies.[6]
Causality assessment is a central component of pharmacovigilance. The WHO-Uppsala Monitoring Centre (WHO-UMC) system relies on structured expert judgement, whereas the Naranjo algorithm provides a quantitative, point-based approach for estimating the probability of ADRs. Comparative studies have demonstrated only moderate agreement between these methods, supporting the combined use of standardised causality tools and improved clinical documentation to enhance reproducibility and reliability of ADR assessment.[7] For parenteral formulations, particularly modern intravenous iron preparations, recent meta-analyses and large observational datasets suggest that severe anaphylactic reactions are rare; however, infusion-related hypersensitivity reactions and cutaneous manifestations occur at measurable rates, underscoring the need for careful administration and immediate availability of emergency management measures.[3,8,9]
The present study aimed to characterise ADRs reported to a quaternary care hospital during the study period, to compare causality assessments with current literature and to identify practice-based interventions to improve medication safety.
Materials and Methods
Study Design and Setting
A retrospective observational study was conducted at a quaternary care teaching hospital in Navi Mumbai, India.
Study Period
ADR reports submitted between 1 January 2022 and 31 December 2024 were included.
Data Source and Eligibility Criteria
All ADR reports documented in the Clinical Pharmacy ADR database during the study period were screened. Reports with complete patient demographics and suspected drug information were included. Duplicate and incomplete reports were excluded.
Data Collection
Data were extracted using a structured proforma capturing age, gender, suspected drug(s), route of administration, organ system involved, severity, management, outcome and causality assessment using the WHO-UMC and Naranjo scales.
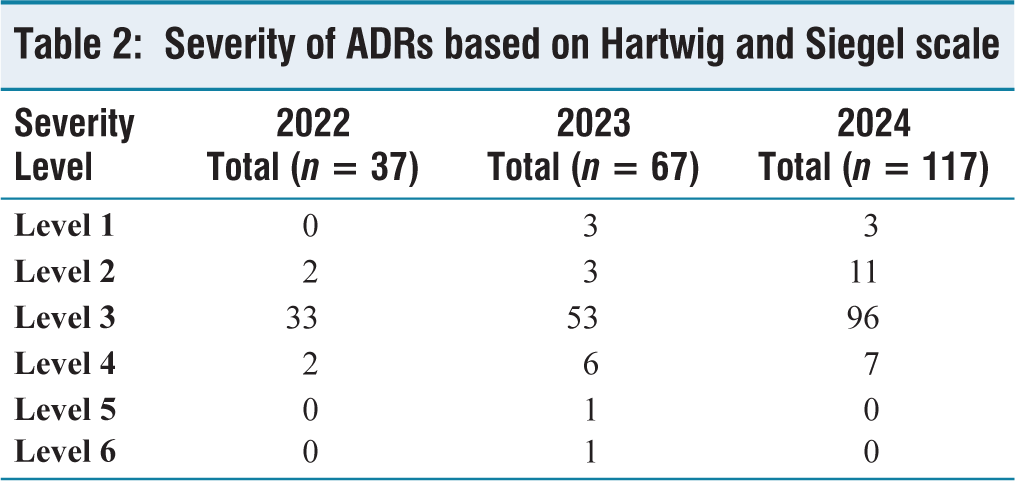
ADR reports were obtained from the Clinical Pharmacy ADR database, where reports are routinely documented by clinical pharmacists as part of institutional pharmacovigilance activities. ADR severity was assessed using the Hartwig and Siegel severity scale, which classifies reactions into mild, moderate and severe based on clinical outcomes and required interventions. Preventability assessment was not performed as part of routine ADR documentation during the study period.
Sample Size
A total of 221 ADR reports met the inclusion criteria and were analysed.
Statistical Analysis
Data were entered into Microsoft Excel and analysed using descriptive statistics, expressed as frequencies and percentages. As the study was retrospective and exploratory in nature, based on spontaneously reported ADRs without predefined comparative groups, inferential statistical analysis was not performed. The objective was descriptive characterisation rather than hypothesis testing.
Ethical Considerations
The study was approved by the Institutional Ethics Committee. As anonymised retrospective data were used, informed consent was waived.
Results
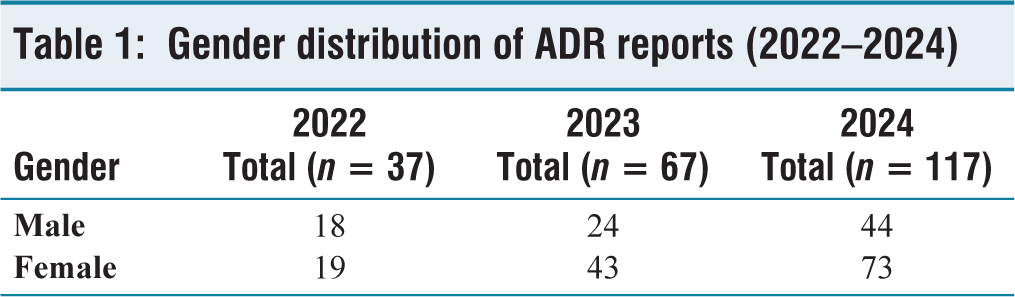
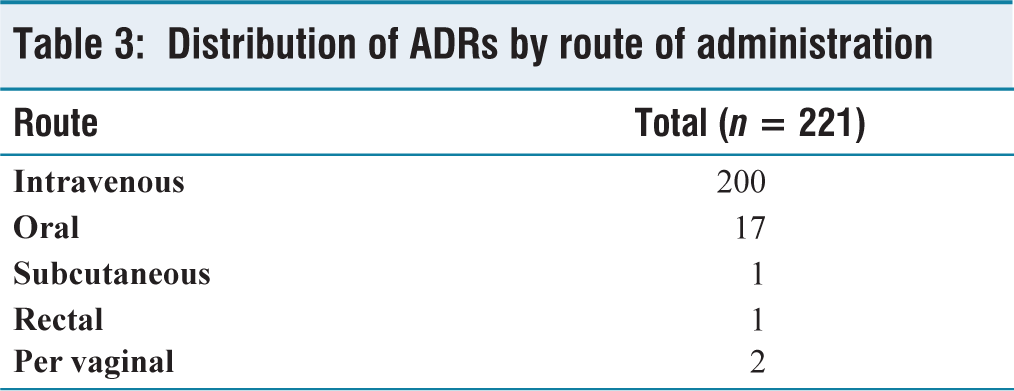
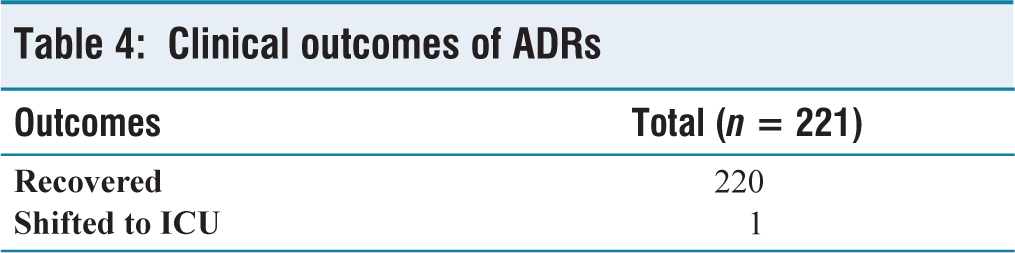
A total of 221 ADRs reported between January 2022 and December 2024 were analysed. The highest proportion of ADRs was observed in patients aged 41–60 years, followed by those aged 21–40 years, while elderly patients (>60 years) accounted for a smaller share of reports. A slightly higher proportion of ADRs occurred in females compared to males across all 3 years [Table 1]. Most ADRs were of moderate severity (Level 3), requiring medical intervention without resulting in permanent harm. Severe reactions were uncommon, and no fatal outcomes were reported [Table 2]. With respect to drug administration, the intravenous route was most frequently associated with ADRs, accounting for the vast majority of cases, whereas oral and other routes contributed minimally [Table 3]. Clinical outcomes were favourable in almost all patients. The majority recovered completely following appropriate management, while only one patient required transfer to the intensive care unit, and no mortality was observed [Table 4]. Exploratory subgroup evaluation showed that intravenous administration was predominantly associated with moderate-severity reactions (Level 3), particularly among antibiotic and iron preparation groups. Middle-aged adults (41–60 years) represented the largest reporting group across most drug classes. However, formal subgroup statistical testing was not undertaken due to the descriptive design.
Gender distribution of ADR reports (2022–2024)
Severity of ADRs based on Hartwig and Siegel scale
Distribution of ADRs by route of administration
Clinical outcomes of ADRs
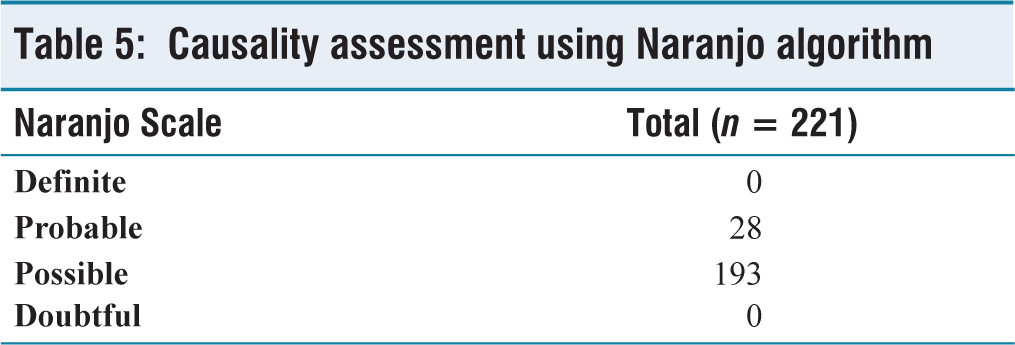
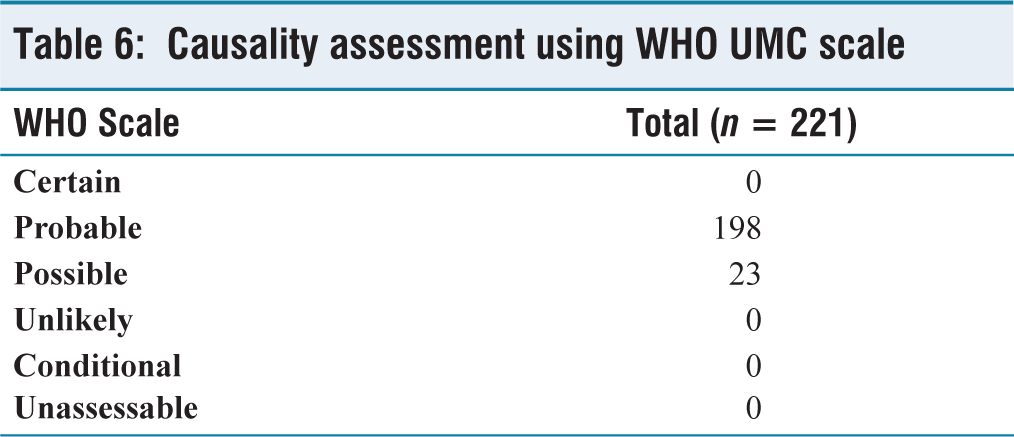
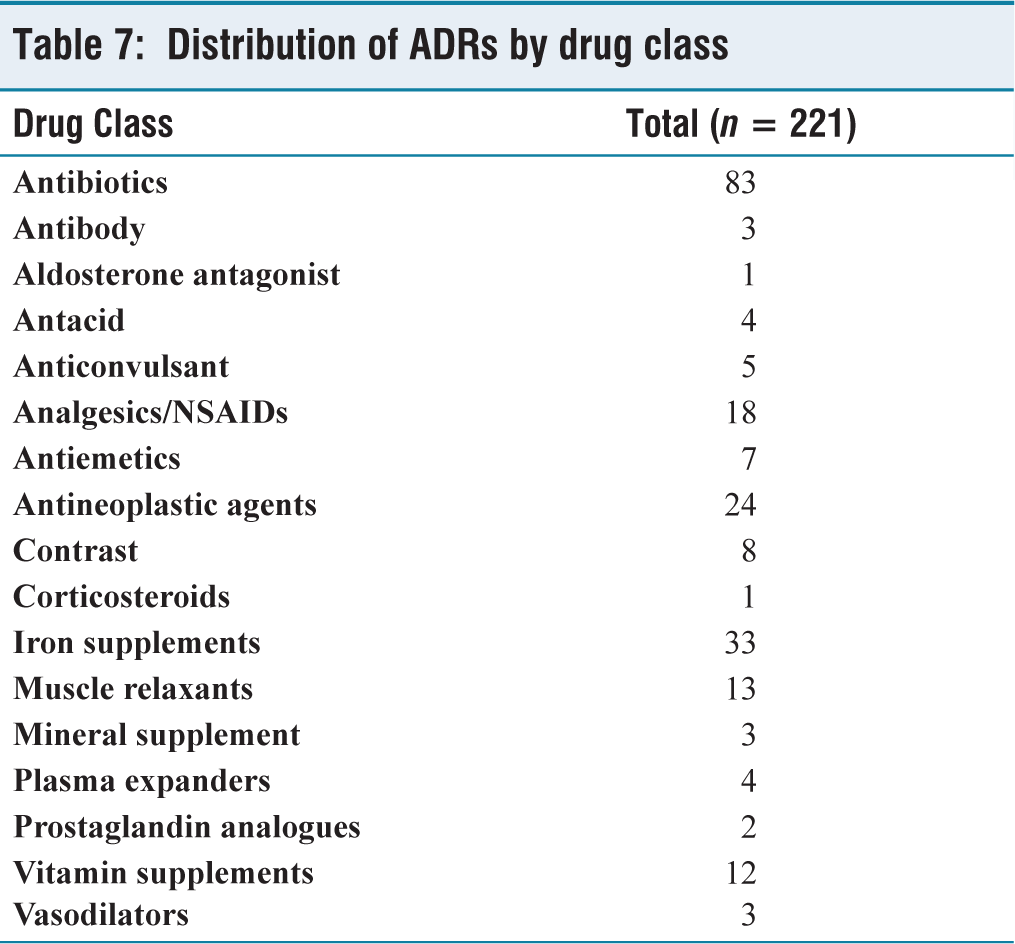
Causality assessment demonstrated variability between tools. Using the Naranjo algorithm, most ADRs were classified as possible, whereas assessment by the WHO-UMC scale categorised the majority as probable, reflecting methodological differences between the two approaches [Tables 5 and 6]. Analysis of suspected drugs revealed that antibiotics were the most frequently implicated drug class, followed by iron supplements and antineoplastic agents. Other drug classes, including analgesics/NSAIDs, muscle relaxants and vitamin supplements, accounted for fewer reports [Table 7].
Causality assessment using Naranjo algorithm
Causality assessment using WHO UMC scale
Distribution of ADRs by drug class
An increasing trend in ADR reports was observed over the 3-year period (37 in 2022, 67 in 2023 and 117 in 2024). This rise likely reflects improved awareness, strengthened pharmacovigilance practices and enhanced reporting culture within the institution rather than a true increase in ADR incidence. Increased involvement of clinical pharmacists and structured ADR monitoring initiatives during the study period may have contributed to improved detection and documentation.
Discussion
In this institutional series (n = 221 ADR reports), antibiotics were the most frequently implicated drug class, followed by intravenous iron preparations and antineoplastic agents. This distribution aligns with hospital-based studies identifying antimicrobials as common triggers of ADRs, likely reflecting high inpatient antibiotic exposure and empiric prescribing practices in tertiary and quaternary care settings.[2–4]
Analgesics/NSAIDs (n = 18) and muscle relaxants (n = 13) were additional contributors, predominantly causing moderate reactions involving gastrointestinal and cutaneous manifestations. Although less frequent than antibiotics and iron preparations, these findings highlight the need for cautious prescribing, particularly in patients with polypharmacy or comorbid conditions.
The predominance of intravenous administration and skin/subcutaneous involvement is consistent with reports describing infusion-related reactions associated with parenteral agents, including modern intravenous iron formulations. While severe anaphylaxis is rare, hypersensitivity reactions occur at measurable rates, emphasising the importance of careful administration and readiness for emergency management.[3]
National and international data indicate that ADR-related hospitalisations remain a measurable healthcare burden, with persistent challenges in detection, reporting and data completeness. Reports from the PvPI similarly identify antibiotics and parenteral drugs as frequently implicated classes, supporting the need for strengthened institutional pharmacovigilance practices.[2]
The higher proportion of ADRs among females and middle-aged adults is consistent with existing literature and may reflect differences in pharmacokinetics, pharmacodynamics, healthcare-seeking behaviour and comorbidity-related polypharmacy.[8]
Most ADRs were moderate in severity and resolved with supportive management, with no mortality observed. These findings emphasise the importance of early recognition, standardised management protocols and ongoing staff training to prevent progression to severe outcomes.
Differences between WHO-UMC and Naranjo causality assessments observed in this study are consistent with prior reports of moderate agreement. The WHO-UMC scale, based on clinical judgement, classified more ADRs as probable, whereas the Naranjo algorithm may underestimate causality in retrospective datasets lacking rechallenge information. Complementary use of both tools may improve consistency and reliability in pharmacovigilance practice.[5]
Based on these findings, key institutional strategies include improving ADR documentation quality, implementing electronic ADR reporting systems, strengthening antimicrobial stewardship programmes and standardising protocols for high-risk parenteral therapies with focused staff training.[10]
This study has several limitations. Being retrospective in nature, it is subject to incomplete data and potential reporting bias. Underreporting of ADRs cannot be excluded, and a preventability assessment was not performed.
Conclusion
ADRs remain an important cause of morbidity in hospitalised patients. Antibiotics and intravenous iron formulations were the most commonly implicated drugs. Strengthening pharmacovigilance systems, improving the quality of ADR reporting and promoting multidisciplinary involvement—particularly of clinical pharmacists—are essential to reduce preventable drug-related harm.
Supplemental material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors acknowledge the support of the Department of Clinical Pharmacy and Pharmacovigilance team, Apollo Hospitals, Navi Mumbai.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethical approval was obtained from the Institutional Ethics Committee, Apollo Hospitals Navi Mumbai (IEC Application No: AHM-ACD-018/03-25).
Informed consent
As this was a retrospective study using anonymised data, informed consent was waived by the Institutional Ethics Committee.
Credit author statement
Concept and study design: Dr Nafhathulla K, Dr Beulah Mariam Jacob, Dr Vijay Niranjan Daberao.
Data collection and curation: Dr Beulah Mariam Jacob, Dr Nafhathulla K.
Data analysis and interpretation: Dr Beulah Mariam Jacob, Dr Nafhathulla K.
Manuscript drafting: Dr Beulah Mariam Jacob, Dr Nafhathulla K.
Critical revision of manuscript: Dr Nafhathulla K, Dr Beulah Mariam Jacob, Dr Vijay Niranjan Daberao.
Final approval of manuscript: All authors.
Credit note for the authors
All authors meet the ICMJE criteria for authorship and take full responsibility for the integrity and accuracy of the work.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Use of artificial intelligence
No artificial intelligence tools were used in the preparation of this manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.