
Abstract
Background and Aims:
Intravenous (IV) therapy is among the most frequently performed clinical procedures in hospital practice. Despite its routine nature, IV therapy is associated with preventable complications such as blood leakage during cannulation, needle-stick injury (NSI), chemotherapy extravasation and peripheral venous catheter-related bloodstream infection (PVC-BSI).
Methods:
A modified Delphi consensus process was conducted through two expert meetings held in September and October 2025 involving nursing leaders and experts in infection control, clinical education and healthcare quality from tertiary healthcare institutions across India. A targeted narrative literature review (2010–2025) was performed using PubMed, Scopus and Google Scholar, along with relevant national and international guidelines, to identify evidence gaps and define thematic domains. Twenty-eight draft consensus statements across four domains—blood leakage, NSI, chemotherapy extravasation and PVC-BSI—were developed and evaluated through anonymous Delphi voting using a 5-point Likert scale. Consensus was predefined as ≥90% agreement, with iterative revision and re-evaluation of non-consensus statements through controlled feedback and subsequent rounds.
Results:
A total of 28 consensus statements across four thematic domains—blood spillage during IV cannulation, NSI, chemotherapy extravasation and PVC-BSI—were evaluated through the modified Delphi process. Most statements achieved strong consensus, with agreement levels ranging from 90% to 100%. Key recommendations emphasised the need for standardised operational definitions, structured competency-based training, adoption of safety-engineered devices, strengthened infection prevention practices, routine root cause analysis (RCA) and corrective and preventive action (CAPA) processes and incorporation of IV therapy-related safety events into institutional quality indicators and surveillance systems. The consensus also highlighted blood spillage during cannulation as an under-recognised IV therapy-associated safety event with important occupational, clinical and operational implications.
Conclusion:
This consensus provides evidence-informed guidance to reduce preventable IV therapy-related complications in Indian corporate hospitals, emphasising nursing leadership, governance and accountability to improve patient safety and infection prevention.
Keywords
Introduction
Intravenous (IV) therapy is among the most performed clinical interventions globally. Current literature suggests that nearly 60%–80% of hospitalised patients receive IV therapy at some point during their admission, most often through peripheral IV catheters for the delivery of fluids, medications or nutritional support.[1] Although IV therapy is a fundamental component of medical care, it is associated with a range of risks that are frequently underestimated. Minor and often overlooked complications contribute meaningfully to patient morbidity and occupational hazards for healthcare workers. Blood leakage during IV cannulation is a frequent occurrence in routine practice; however, its actual prevalence is not well documented. Audit findings and observational studies indicate visible blood leakage in approximately 10%–20% of cannulation attempts, a figure likely under-reported due to the lack of standardised definitions and formal monitoring mechanisms.[2,3]
Blood leakage during IV cannulation was defined as any visible leakage of blood from the catheter hub, insertion site or needle during or immediately after cannula insertion prior to secure connection of the IV line. Needle-stick injury (NSI) was defined as any percutaneous injury caused by a needle or sharp medical device contaminated with blood or body fluids. Chemotherapy extravasation was defined as the inadvertent leakage of vesicant or irritant drugs from the vein into surrounding tissues during IV administration, leading to potential tissue injury. Peripheral venous catheter-related bloodstream infection (PVC-BSI) was defined as a laboratory-confirmed bloodstream infection in a patient with a peripheral IV catheter in situ or within 48 h of removal, without an alternative identifiable source of infection. Additionally, visual infusion phlebitis (VIP) score escalation was defined as an increase in VIP score ≥2 from baseline, indicating clinically significant progression of phlebitis requiring intervention.[4–6]
NSIs remain a significant occupational concern, affecting an estimated 45%–58% of healthcare workers globally, with Indian hospital data reporting nearly 10 NSI incidents per 100 occupied beds annually.[7,8] While chemotherapy extravasation occurs less frequently, it is associated with considerable morbidity, with reported incidence rates ranging from 0.1% to 6% in oncology settings.[9] Additionally, PVC-BSIs have been reported in 0.03%–0.18% of peripheral IV insertions, representing a substantial clinical burden given the extensive use of peripheral venous access devices. 3 Collectively, these findings underscore a significant yet insufficiently recognised burden of IV therapy-associated complications and emphasise the need for improved prevention and surveillance efforts.
Within the Indian healthcare context, persistent challenges remain, including disparities in staff training, inconsistent compliance with infection prevention protocols and under-reporting of IV therapy-related adverse events.[10] Moreover, evidence from Indian corporate healthcare settings addressing these issues is limited. There is currently no standardised agreement on operational definitions, preventive measures or monitoring protocols for IV therapy complications.
To bridge these gaps, a Consensus Meeting was organised involving 10 experts, and the primary aim of this initiative was to develop an evidence-informed consensus to define the scope and burden of IV therapy-related complications, establish standardised prevention and reporting frameworks for blood leakage, NSIs, chemotherapy extravasation and PVC-BSIs.
Methods
This report is based on a structured, expert-driven consensus process designed to identify, categorise and develop standardised recommendations for the prevention and management of complications associated with IV therapy in Indian corporate hospitals. A consensus methodology was selected to integrate multidisciplinary perspectives in areas where empirical data are limited but clinical experience and contextual expertise are substantial.[11,12] Two structured expert meetings were conducted on 26 September 2025 and 28 October 2025.
This study employed a modified Delphi methodology to achieve expert consensus, conducted in accordance with the CREDES checklist. The process was designed to ensure methodological rigour, transparency and reproducibility through predefined steps including expert selection, structured rounds, controlled feedback and explicit consensus criteria.[13]
Delphi Design and Rationale
A modified Delphi approach was chosen to combine evidence-based inputs with expert interpretation, allowing structured consensus building in areas where high-quality primary data are limited. The modification included integration of a pre-meeting literature review and a final structured discussion round to enhance contextual relevance.
Expert Panel Selection and Eligibility Criteria
The expert panel comprised ten members representing nursing leadership, clinical education, infection control and hospital administration from tertiary corporate hospitals across India. Experts were purposively selected based on predefined eligibility criteria, including:
A minimum of 10 years of clinical, academic or leadership experience in IV therapy, infection prevention, nursing governance or quality and patient safety. Direct involvement in hospital SOP formulation, protocol implementation, staff training or infection control programmes at the institutional level; and Experience managing or auditing IV therapy-related complications within large healthcare organisations.
This ensured that panellists possessed both operational and strategic insight relevant to IV therapy safety in Indian hospital settings.
Evidence Review and Statement Generation
Prior to the meetings, the organising committee conducted a targeted narrative literature review of international and Indian publications from 2010 to 2025, focusing on IV therapy complications, safety-engineered devices, nursing education models and infection prevention strategies. A targeted narrative literature review of international and Indian publications from 2010 to 2025 was conducted. Relevant literature was identified through electronic databases including PubMed, Scopus and Google Scholar, along with key clinical practice guidelines from organisations such as the Centres for Disease Control and Prevention and the Infusion Nurses Society. Additional relevant articles were identified through manual reference screening of selected publications. The search strategy incorporated combinations of free-text terms and database-specific indexing terms (e.g., MeSH), including ‘intravenous therapy’, ‘peripheral intravenous catheter’, ‘vascular access’, ‘needle-stick injury’, ‘extravasation’, ‘phlebitis’ and ‘catheter-related bloodstream infection’, combined using Boolean operators (AND/OR) and adapted for each database. Evidence sources included clinical guidelines, systematic reviews, observational studies and relevant hospital audit data.
Based on this review, an initial list of draft consensus statements was generated for each thematic domain and was circulated to panellists in advance to support informed discussion and evidence-based consensus formation.
Delphi Rounds and Consensus Process
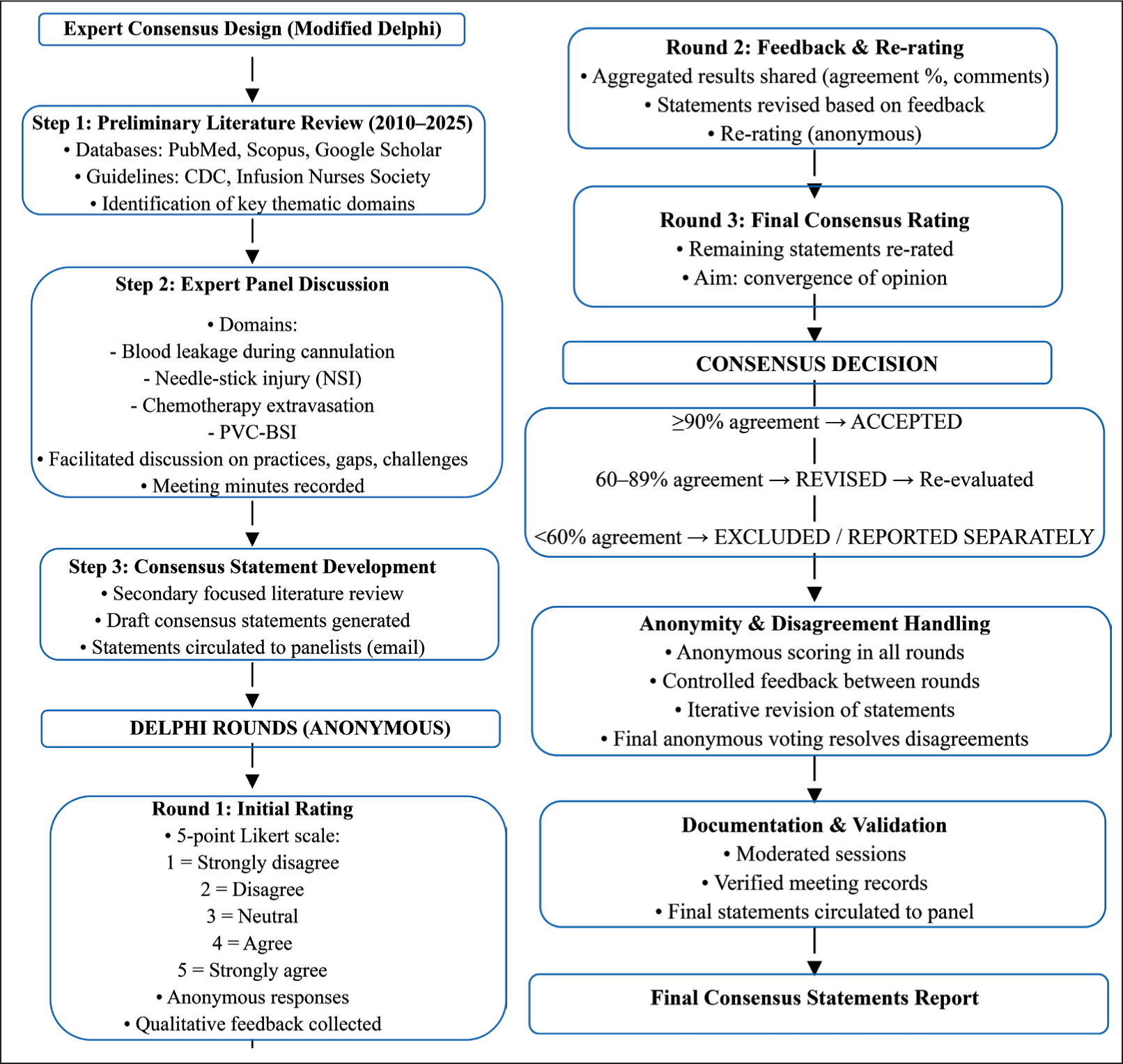
The modified Delphi process was conducted in a structured, stepwise manner integrating literature review, expert discussion and iterative consensus building.
Step 1: Preliminary Literature Review and Topic Identification
An initial targeted literature review (2010–2025) was conducted using databases such as PubMed, Scopus and Google Scholar, along with key clinical practice guidelines from the Centres for Disease Control and Prevention and Infusion Nurses Society. Based on this review, key thematic domains relevant to IV therapy safety were identified to guide expert panel discussions.
Step 2: Expert Panel Discussion and Report Generation
A structured expert panel meeting was conducted, focusing on the predefined thematic domains:
Blood leakage during cannulation NSI Chemotherapy extravasation PVC-BSI
Facilitated discussions explored current practices, gaps and contextual challenges in Indian healthcare settings. Detailed meeting minutes were recorded, and a summary report capturing key discussion points and expert opinions was generated.
Step 3: Statement Generation and Evidence Refinement
Following the panel discussion, a second focused literature review was conducted to validate and supplement expert inputs. Based on the combined evidence (literature and discussion report), a set of draft consensus statements was developed across all domains and circulated electronically (via email) to all panellists prior to Round 1.
Step 4: Round 1 (Anonymous Rating)
Panellists independently rated all statements using a five-point Likert scale:
1 = Strongly disagree 2 = Disagree 3 = Neither agree nor disagree 4 = Agree 5 = Strongly agree
Responses were collected anonymously to minimise bias and group influence. Panellists were also invited to provide qualitative feedback and suggest modifications.
Step 5: Round 2 (Controlled Feedback and Re-rating)
Aggregated results from Round 1, including percentage agreement and anonymised comments, were shared with the panel. Statements not meeting predefined consensus criteria were revised based on individual feedback and redistributed for re-rating. Anonymity was maintained during this round.
Step 6: Round 3 (Final Anonymous Consensus Round)
Statements that did not achieve consensus after Round 2 were subjected to a final round of anonymous rating using the same Likert scale. This round aimed to achieve convergence of opinion following iterative refinement.
Consensus Criteria
Consensus achieved: ≥90% agreement (ratings of 4 or 5)
Partial agreement: 60%–89% → revised and re-evaluated in subsequent round
No consensus: <60% → excluded or reported separately
Anonymity and Handling of Disagreement
Anonymity was maintained during all rating rounds (Rounds 1, 2 and 3) to reduce dominance and hierarchy bias. Controlled feedback was provided between rounds in the form of aggregated results and anonymised comments.
Differences in opinion were addressed through iterative revision of statements based on panel feedback. Persistent disagreements were resolved through final anonymous voting, ensuring that consensus was not driven solely by majority opinion or group influence. Moderation during discussions ensured balanced participation without compromising independent judgement.
Data Validation and Ethics
All sessions were moderated by the programme director and documented through structured minutes. Independent reviewers verified the accuracy of meeting records, and anonymised data were compiled into thematic summaries. The final set of consensus statements was circulated electronically for validation and minor edits by all panellists prior to inclusion in this report.
The consensus development process is summarised in Figure 1.
Modified Delphi process for development of expert consensus on IV therapy-related safety events
As this was a professional expert consensus activity without patient-level data or human subject participation, ethics committee approval was not required. All participants provided consent for the use and publication of aggregated, non-identifiable findings.
Results
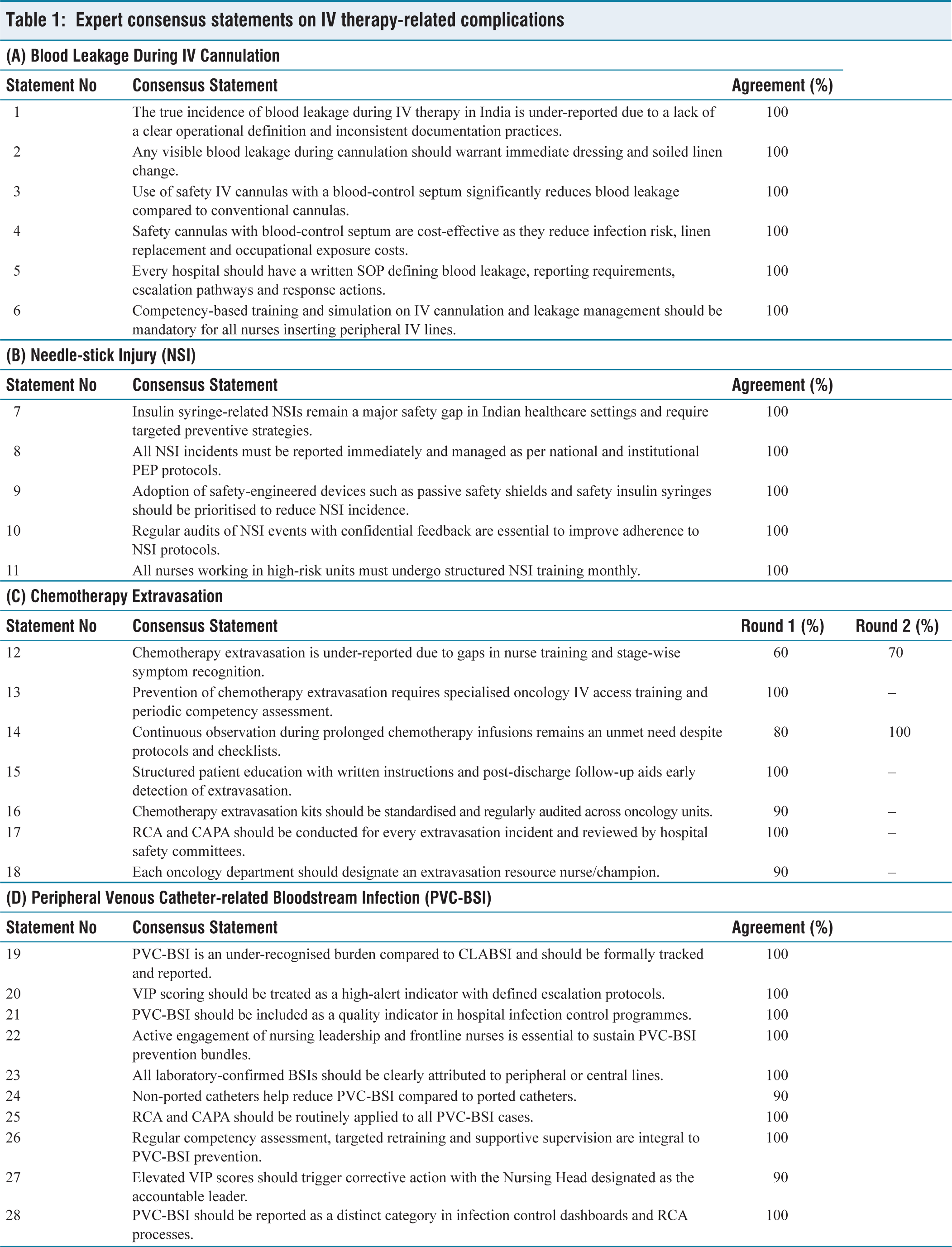
Findings from two expert consensus meetings held on 26 September 2025 and 28 October 2025 were synthesised to develop standardised recommendations for the prevention and management of IV therapy-related complications in Indian corporate hospitals. A total of 28 draft consensus statements, spanning four domains: blood leakage, NSI, chemotherapy extravasation and PVC-BSI, were evaluated using a modified Delphi approach. Consensus was predefined as =90% agreement (ratings of 4 or 5 on a five-point Likert scale).
In Round 1, 26 of 28 statements (92.9%) met the consensus threshold and were accepted without modification. All statements related to blood leakage and NSI achieved 100% agreement, reflecting unanimous endorsement of standardised definitions, mandatory reporting, safety-engineered devices and competency-based training. Most statements addressing chemotherapy extravasation and PVC-BSI also achieved strong agreement (90%–100%), supporting structured surveillance, leadership accountability and routine RCA-CAPA processes.
Two chemotherapy extravasation statements failed to meet the threshold in Round 1 (agreement 60% and 80%) and were revised based on panel feedback. In Round 2, one revised statement addressing challenges in continuous monitoring during prolonged chemotherapy infusions achieved 100% agreement and was accepted. The second revised statement, relating to under-reporting of chemotherapy extravasation due to variability in nurse training, achieved 70% agreement and was excluded.
Overall, 27 of 28 statements (96.4%) achieved formal consensus and constitute the final recommendations presented in Table 1A-1D.
Expert consensus statements on IV therapy-related complications
Discussion
The expert consensus meetings identified complications related to IV therapy as a substantial yet under-recognised concern within Indian corporate hospitals. Despite the availability of established infection prevention guidelines, gaps remain in standardisation, consistent frontline implementation, reinforcement of training and documentation practices. These observations align with the broader patient safety literature, which underscores that the success of technical interventions depends not solely on device availability but on well-functioning organisational systems, clearly defined accountability structures and sustained workforce competency.[14–16]
A recurring theme across all domains was the divergence between institutional policies and actual bedside practice. Although most participating hospitals reported the presence of formal standard operating procedures (SOPs), inconsistent adherence- driven by factors such as high nursing turnover, workload pressures and limited opportunities for refresher training- significantly diminishes their effectiveness.[1] Furthermore, evidence indicates that patient safety initiatives are most effective when supported by simulation-based training, periodic reassessment and visible leadership engagement, rather than relying solely on one-time induction programmes.[17,18] In this context, the panel emphasised the integration of IV therapy competencies into ongoing nursing education frameworks.
Blood Leakage During Cannulation
The consensus panel noted that blood leakage is likely under-reported due to the absence of uniform definitions and routine surveillance mechanisms, a concern consistent with findings from international IV therapy audits that identify blood leakage and dressing contamination as common yet inconsistently documented events.[2,3] Within the Indian healthcare context, no published data specifically quantify blood leakage during IV cannulation, as existing studies largely focus on broader infection control outcomes rather than procedural contamination events.
Importantly, the panel agreed that any visible blood leakage, irrespective of volume, should prompt immediate dressing and linen replacement. Blood leakage during IV cannulation has important implications for healthcare workers, patients and healthcare systems. For healthcare workers, it increases the risk of exposure to blood-borne infections such as HIV, hepatitis B and hepatitis C, along with a higher likelihood of needle-stick injuries. It also contributes to psychological stress, requires post-exposure prophylaxis and follow-up and can disrupt workflow.
For patients, blood leakage may indicate compromised aseptic technique, increasing the risk of infection and IV-related complications. It can lead to repeated cannulation attempts, procedural delays, discomfort and reduced patient satisfaction and trust in care.
From a financial and institutional perspective, blood leakage results in increased costs due to additional consumables, cleaning and waste management, as well as expenses related to occupational exposure management. It also affects staff efficiency, hospital productivity and quality indicators, with potential medico-legal implications.[19]
This recommendation reflects its implications for infection prevention, patient reassurance and perceived quality of care. Infection prevention guidelines consistently advocate for the prompt replacement of visibly contaminated dressings and linen to minimise cross-transmission risk and maintain patient confidence.[14,18]
The recommendation for written SOPs defining blood leakage, reporting mechanisms and escalation protocols is consistent with established safety management principles that identify standardisation as a foundational requirement for reliable healthcare delivery.[15] In addition, mandatory competency-based training and simulation for IV cannulation are supported by evidence demonstrating reduced catheter failure rates and lower complication incidence in institutions implementing structured training programmes.[1,20]
The panel’s endorsement of safety IV cannulas incorporating a blood-control septum is supported by device-specific clinical evidence. A prospective observational study evaluating an IV catheter designed to prevent blood leakage reported a significant reduction in blood leakage during catheter insertion and subsequent handling when compared with conventional safety IV catheters, resulting in lower contamination risk and reduced cleaning-related workload.[21]
From a practice perspective, hospitals should operationalise blood leakage prevention by embedding clear SOPs, mandatory linen-change triggers and cannulation competency assessment into routine nursing audits and onboarding processes.
Needle-stick Injury
The consensus statements demonstrated strong alignment with international occupational safety priorities. The panel unanimously identified insulin syringe-related NSIs as a major contributor to preventable occupational injury, a conclusion supported by systematic reviews that highlight insulin administration and disposal as leading sources of NSIs due to their high frequency of use and limited inherent safety features.[7,22] Mandatory reporting of all NSIs and strict adherence to PEP protocols were strongly endorsed, consistent with World Health Organisation guidance linking timely reporting to improved clinical outcomes and reduced psychological distress among affected healthcare workers.[14]
Within the Indian healthcare context, several hospital-based studies have documented substantial under-reporting of NSIs, with estimates ranging from approximately 40% to over 70%. This under-reporting has been attributed to factors including fear of blame, limited awareness of reporting pathways, perceived low risk of exposure and competing clinical demands.[23,24] These findings suggest that the true burden of NSIs among Indian healthcare workers is likely underestimated, underscoring the need for structured reporting systems supported by a non-punitive, leadership-driven culture of safety.
Practically, NSI prevention programmes in Indian hospitals should combine routine use of safety-engineered devices with confidential reporting systems and structured, high-frequency training—particularly in ICUs, emergency units and operating theatres. In addition, there should be a dedicated NSI champion(nurse) in every department who will focus on the execution of SOP & review training.
Role of Safety-engineered Devices
In addition to organisational and training interventions, safety-engineered devices play a critical role in reducing NSIs. Both observational and systematic reviews have demonstrated that passive safety devices are more effective in reducing percutaneous injuries than active devices, as they minimise reliance on user activation and thereby reduce opportunities for procedural error.[25,26]
At the institutional level, procurement policies should prioritise passive safety devices with proven effectiveness in reducing occupational exposure, supported by staff training to ensure correct and consistent use.
Chemotherapy Extravasation
Although chemotherapy extravasation occurs relatively infrequently, the panel underscored its disproportionate clinical, psychological and medico-legal consequences. All endorsed statements emphasised the importance of specialised oncology IV access training, formal competency validation and periodic refresher programmes, consistent with international oncology nursing standards that recommend credentialed administration of vesicant and high-risk agents.[9,27] The panel also acknowledged practical challenges in maintaining continuous infusion-site monitoring during prolonged chemotherapy administrations, reflecting staffing and workflow constraints commonly described in oncology safety literature.[28]
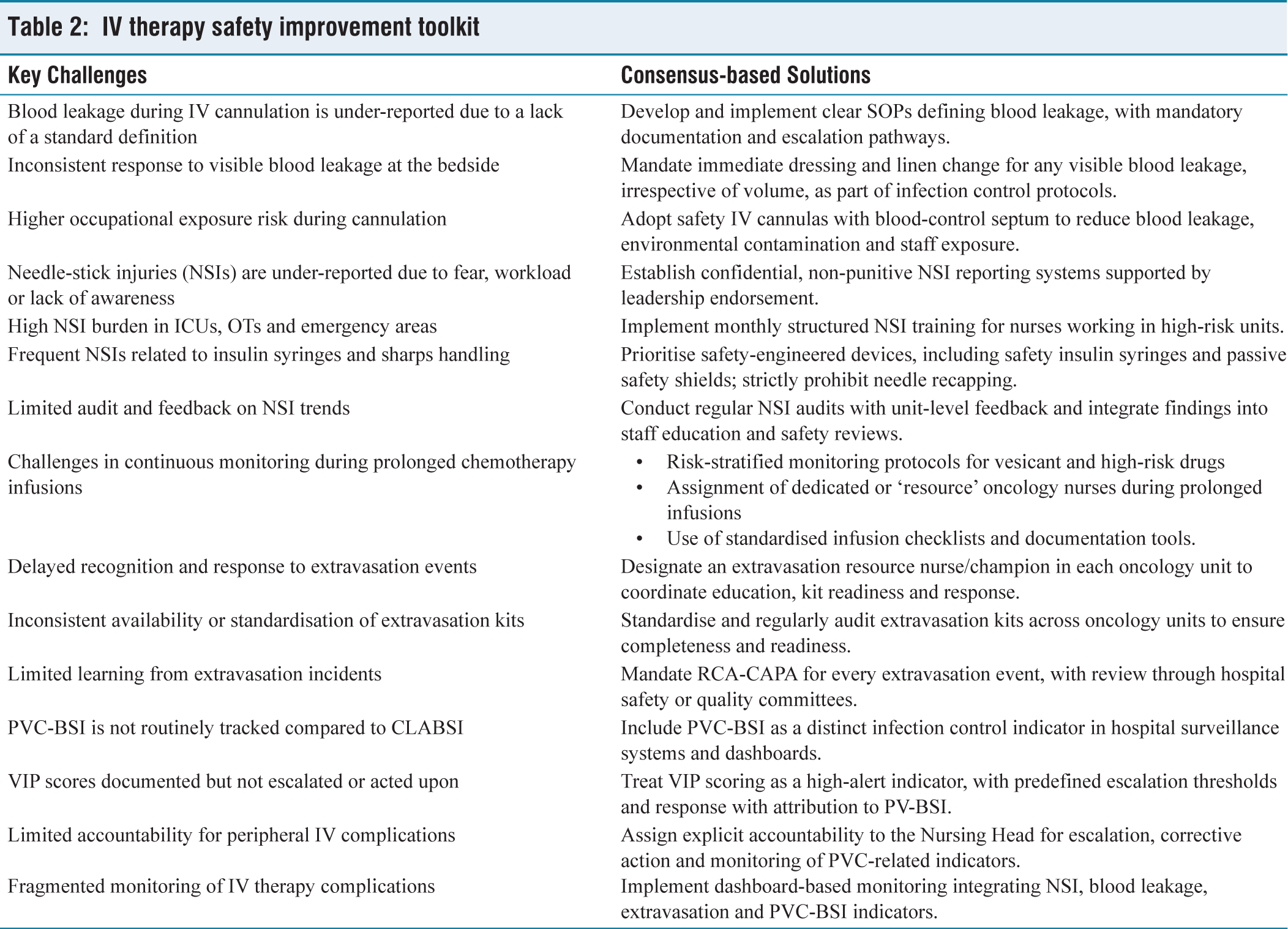
To address these challenges, the panel recommended a combination of system-based strategies, including risk-stratified monitoring protocols for vesicant and other high-risk agents, assignment of designated or ‘resource’ oncology nurses during prolonged infusions, scheduled site assessments at predefined intervals and use of standardised infusion checklists and documentation tools [Table 2].
IV therapy safety improvement toolkit
The panel strongly endorsed mandatory RCA-CAPA for all chemotherapy extravasation events, reinforcing the importance of systematic learning from adverse incidents, a practice widely advocated in medication safety and oncology risk management frameworks.[29]
Oncology units should designate trained extravasation resource nurses and implement risk-stratified monitoring protocols to ensure early detection and rapid response during prolonged chemotherapy infusions.
Peripheral Venous Catheter-related Bloodstream Infection
Consensus recommendations for PVC-BSIs emphasised the establishment of formal surveillance and reporting systems distinct from central line-associated bloodstream infections, use of VIP scores as high-alert indicators with defined escalation protocols, explicit leadership accountability, particularly at the level of nursing leadership, routine root cause analysis and corrective and preventive action (RCA-CAPA), preferential use of non-ported catheters and dashboard-based monitoring supported by ongoing staff competency assessment.
PVC-BSI was identified as a critically under-prioritised area. The panel unanimously agreed that PVC-BSIs should be systematically tracked and reported separately from central line infections, consistent with evidence demonstrating that peripheral IV catheters account for a substantial proportion of bloodstream infections due to their widespread use.[3,6] In the Indian context, a prospective study conducted in a tertiary care intensive care unit reported a 19.5% incidence of PVC-BSI among patients with peripheral venous catheters, with Staphylococcus aureus and Klebsiella species identified as the most common pathogens.[30] 1
Consensus statements also reinforced the use of VIP scoring as a high-alert indicator, supported by evidence linking elevated VIP scores with increased risk of catheter failure and infection.[19] Indian nursing audits have documented inconsistent documentation and escalation of VIP scores despite their routine inclusion in nursing records, indicating an implementation gap rather than a lack of available tools.[31] Explicit accountability of nursing leadership for escalation and corrective action reflects governance models in which leadership engagement is associated with improved compliance and sustained reductions in infection rates.[16]
In Indian hospitals characterised by high patient volumes and variable staffing patterns, leadership-driven monitoring and dashboard-based surveillance were viewed as essential enablers of sustainable PVC-BSI prevention. Nurses serve as the primary custodians of IV therapy safety, with nursing leadership playing a pivotal role in oversight, audit, escalation and the development of a culture of safety. Embedding safety principles into routine nursing practice—supported by simulation-based training, regular audits, transparent reporting and RCA-CAPA processes—is strongly supported by quality and patient safety literature as a foundation for sustained improvement.[14,15]
Finally, the consensus determined that strengthening IV therapy safety is closely aligned with broader goals of hospital accreditation, nursing excellence and patient-centred care. By empowering nursing staff, clarifying leadership accountability and institutionalising evidence-based practices, Indian corporate hospitals can progress towards internationally benchmarked standards of IV therapy safety and clinical governance.
Strengths
This consensus draws strength from its multidisciplinary expert panel representing nursing leadership, infection control, clinical education and hospital administration across Indian corporate hospitals. The use of a structured modified Delphi methodology enabled systematic integration of clinical experience with available evidence in areas where India-specific epidemiological data remain limited. The domain-wise approach and high consensus threshold ensured that recommendations are both contextually relevant and implementation-ready for real-world hospital settings.
Limitations
This consensus has several limitations. As an expert opinion-based process, the findings are inherently influenced by the clinical experience, institutional practices and perspectives of the participating experts. The relatively small panel size (n = 10), although consistent with Delphi methodology, may limit the breadth of viewpoints and reduce representativeness across diverse healthcare settings. Additionally, the panel primarily comprised experts from tertiary corporate hospital settings, which may not fully reflect the realities of public-sector institutions or resource-constrained environments, where infrastructure, staffing and infection control practices may differ significantly.
Conclusion
The expert consensus demonstrated that complications related to IV therapy are largely preventable through structured, system-level interventions, particularly within the high-volume and resource-variable context of Indian corporate hospitals. Key recommendations included clear SOPs and competency-based training for blood leakage prevention, regular structured NSI training with safety-engineered devices and mandatory reporting, specialised oncology IV competency with designated extravasation resource nurses and formal surveillance of PVC-BSI using VIP score-based escalation and dashboard monitoring.
Overall, the findings highlight that standardisation, sustained nursing competency and leadership-driven oversight are essential to improving IV therapy safety in India. Adoption of these consensus-driven practices can strengthen patient safety, reduce occupational risk and help Indian hospitals align with national accreditation standards and internationally accepted best practices in IV therapy quality and governance.
Supplemental material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
B. Braun India organised the project management and the medical writing support was provided by Medofy Healthcare Solutions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable.
Informed consent
Not applicable.
Credit author statement
Study conception or design of the work: all authors.
Data collection: all authors.
Data analysis and interpretation: all authors.
Drafting the article: all authors.
Critical revision of the article: all authors.
Final approval of the version to be published and accountability for all aspects of the work: all authors.
Data availability statement
Data will be made available upon reasonable request from Dr Akhil Agarwal.
Use of artificial intelligence
None.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.