
Abstract
Health expenditure is vital for individuals and the state, reflecting a common concern for well-being, productivity and societal health. This study examines the factors that influence health expenditure in the context of environmental pollution, economic growth, ageing population, and educational attainment in the Gulf Cooperation Council (GCC) countries. It utilizes data from 2000 to 2022 for a panel of six nations and employs the augmented mean group (AMG) estimation, which is further cross-examined by the correlated common effects mean group (CCEMG) estimation and the Dumitrescu–Hurlin (D-H) Granger non-causality test. The AMG estimation findings reveal that CO2 emissions significantly increase healthcare spending in the GCC nations, while economic growth helps mitigate it; education has no significant impact, and the small elderly population reflects ageing as an insignificant factor. This highlights an ageing pattern that diverges from global trends but mirrors regional realities. The robustness assessments, as determined by the CCEMG estimation and the D-H Granger non-causality test, also validate the AMG estimation outcomes. Our findings have important policy implications for policymakers that the GCC nations should strengthen environmental regulations, invest in green technologies, raise public awareness, integrate pollution data into health planning, enhance regional cooperation, leverage economic growth to improve healthcare efficiency, and reassess educational programmes to better influence health behaviours and spending.
I. Introduction
Healthcare is one of the most essential spending categories for the general public and individuals. People work hard to safeguard their mental and physical well-being, improving their overall productivity and quality of life. The state is responsible for establishing a healthy society and providing its inhabitants with basic healthcare. In many nations, healthcare costs have steadily increased (Getzen, 2017) as a proportion of gross domestic product (GDP) and per capita expenditure. This ongoing tendency has raised concerns that healthcare costs will continue to rise, endangering the financial stability of healthcare systems (Mason & Miller, 2018). Therefore, both the state and people are concerned about this steady rise in health spending. Thus, a common field of inquiry is the relationship between health costs and their determinants. Figure 1 illustrates the healthcare expenditure (HE) (as a percentage of GDP) scenario in the Gulf Cooperation Council (GCC) countries.
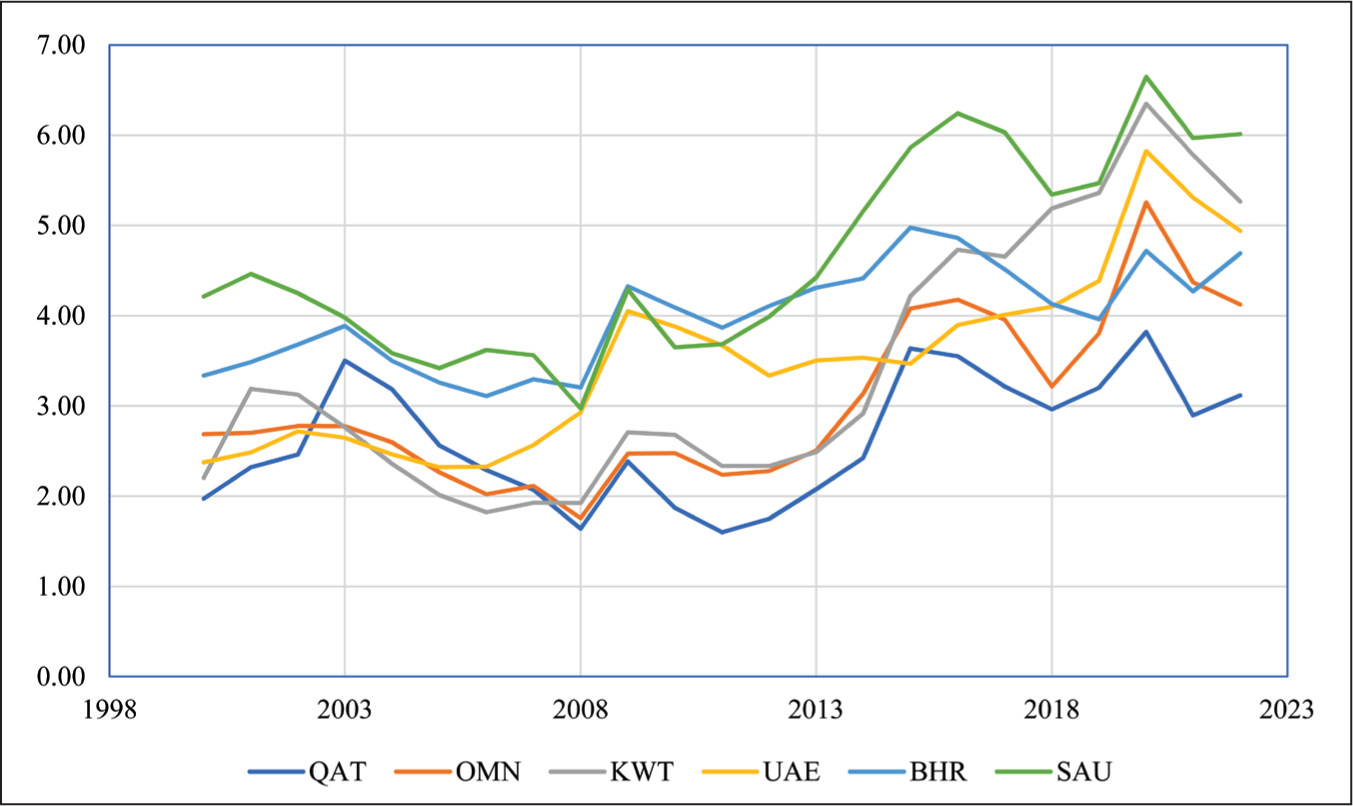
HE have increased across the GCC nations from 2000 to 2022. Saudi Arabia has been the top spender on healthcare, with 4.64% of its GDP, followed by Bahrain in second place with 4% of its GDP and the United Arab Emirates in third place with 3.51% of its GDP, on average, during the period 2000–2022. Kuwait has been placed fourth, with 3.41% of its GDP spent on healthcare, Oman in fifth position with 3.03% of its GDP, and Qatar has been the least spender among the GCC nations, with an average of 2.63% of its GDP spent on healthcare during the study period.
The theoretical literature in this field encompasses the interactions between HE, economic growth and environmental quality. However, the contemporary notion of sustainable development has created an image in which different ideas are intertwined and cannot be considered independently. Literature suggests that most studies have investigated the relationship between HE and their economic determinants while overlooking the impact of environmental, demographic and social factors. This study fills the research gap by examining the relationship between health expenditures, environmental quality, economic growth, the population aged 65 years or older and education.
In particular, environmental quality has become a key factor in determining healthcare needs. Environmental pollution is a significant source of non-communicable diseases like cancer and respiratory disorders. Breathing in polluted air can cause coughing, wheezing, breathing difficulty and irritation of the eyes, nose and throat. As a result, air pollution is a significant factor in determining health and healthcare costs, and it has garnered global attention (Li et al., 2020). Several studies have evidenced that CO2 emissions in the air accelerate the HE in many countries (Xia et al., 2022; Yassin & Aralas, 2019). According to Marmore (2017) and Farahat (2022), the GCC countries have air pollution levels that exceed the global average, with Saudi Arabia and Qatar experiencing dangerously high PM2.5 levels. Therefore, it is a worthy exercise to examine the impact of environmental pollution on the growing HE of the GCC nations. Hence, we intend to explore the effect of CO2 emissions on healthcare expenses of the GCC region for the first time.
In addition to environmental factors, economic growth plays a substantial role in shaping HE. Researchers have widely studied the relationship between health expenditures and economic growth, as documented in the literature. The notion is that health expenditures lead to good health, contributing to economic growth (Islam, 2020a, 2020b; Khrais & Suleiman, 2024). However, our concern is to examine how economic growth contributes to HE. Many references suggest that economic growth finances rising HE, owing to increasing demand for preventive healthcare, long-term care, rehabilitation care and inpatient and outpatient treatments. Furuoka et al. (2011), Kea et al. (2011), Kraipornsak (2017), Phi (2017), Barkat et al. (2019), Yassin and Aralas (2019), Zhou et al. (2020), Piscopo et al. (2024) and Scalamonti (2025) evidenced that economic growth has been a contributory factor in determining the rising HE across the world. The GCC nations witnessed a continuous and sustained increase in HE, and we want to examine the role of economic growth in these expenditures.
Furthermore, demographic changes, especially an ageing population, introduce another important factor. Ageing populations pressure healthcare systems, raising concerns about rising healthcare costs. The world’s ageing population raises concerns about its impact on health expenditures due to the elderly’s increased care demands (Kallestrup-Lamb et al., 2024). An increased percentage of elderly people has caused problems for several high-income developed countries (Lee, 2014). Given the documented positive relationship between age and healthcare spending, this demographic transition is especially worrisome (Fledsberg et al., 2023). Consequently, one of the leading causes of the current and projected future increases in healthcare spending is population ageing. There are numerous instances where an ageing population has contributed to escalating HE (Barkat et al., 2019; Furuoka et al., 2011; Kallestrup-Lamb et al., 2024; Kea et al., 2011; Phi, 2017; Yassin & Aralas, 2019; Zhou et al., 2020). In contrast, there is evidence that an ageing population does not necessarily lead to increased health expenditures (Piscopo et al., 2024). The GCC countries are among the high-income nations, and examining the determinants of health expenses in these countries, the ageing population cannot be overlooked. Therefore, this study considers the ageing population a key factor in HE.
Along with environmental and demographic factors, education emerges as a key social determinant of health expenditures. Education significantly impacts HE by influencing health behaviours, service access and policy priorities. Higher education levels are linked with increased health awareness, leading to pronounced utilization of preventive services and early treatment, which can raise healthcare spending. For example, education is among the most significant drivers of HE in OECD countries (Yetim et al., 2020). Moreover, education enhances individuals’ ability to navigate healthcare systems, follow medical advice and make informed healthcare decisions, contributing to more efficient utilization of healthcare resources (Raghupathi & Raghupathi, 2020). Therefore, education significantly influences individual health outcomes and has a profound impact on national HE. For example, Moayedfard et al. (2020) reported a positive correlation between literacy and HE. Therefore, we intend to examine the role of education in shaping HE in the GCC nations.
The novelty of our research lies in the methodological improvements, comprehensive inclusion of determinants and focused regional relevance, all of which contribute to enhanced empirical precision. (1) This study utilizes an advanced methodology. It is the first to utilize second-generation estimators, such as the AMG estimation, to examine the determinants of health expenditures, addressing cross-sectional dependency and slope heterogeneity that are neglected by earlier first-generation methods. (2) We employ a comprehensive model. Unlike earlier studies, this study combines economic, environmental, and social factors into a single model, providing a comprehensive view of health expenditure drivers. (3) This study has a regional focus. This is the first rigorous analysis of health expenditure determinants in GCC nations, utilizing advanced second-generation methods, unlike previous studies (Ali & Sayed, 2020) that relied on outdated and less reliable techniques. (4) The study examines how ageing, economic growth, environmental pollution and education jointly affect health spending in the little-studied GCC region. This region exhibits distinct economic and demographic characteristics that have received relatively little attention in the literature. The remainder of the research is structured as follows. Literature is reviewed in Section II, data and methods are discussed in Section III, results and findings are disclosed in Section IV, and the conclusion and research implications are presented in Section V.
II. Literature Review
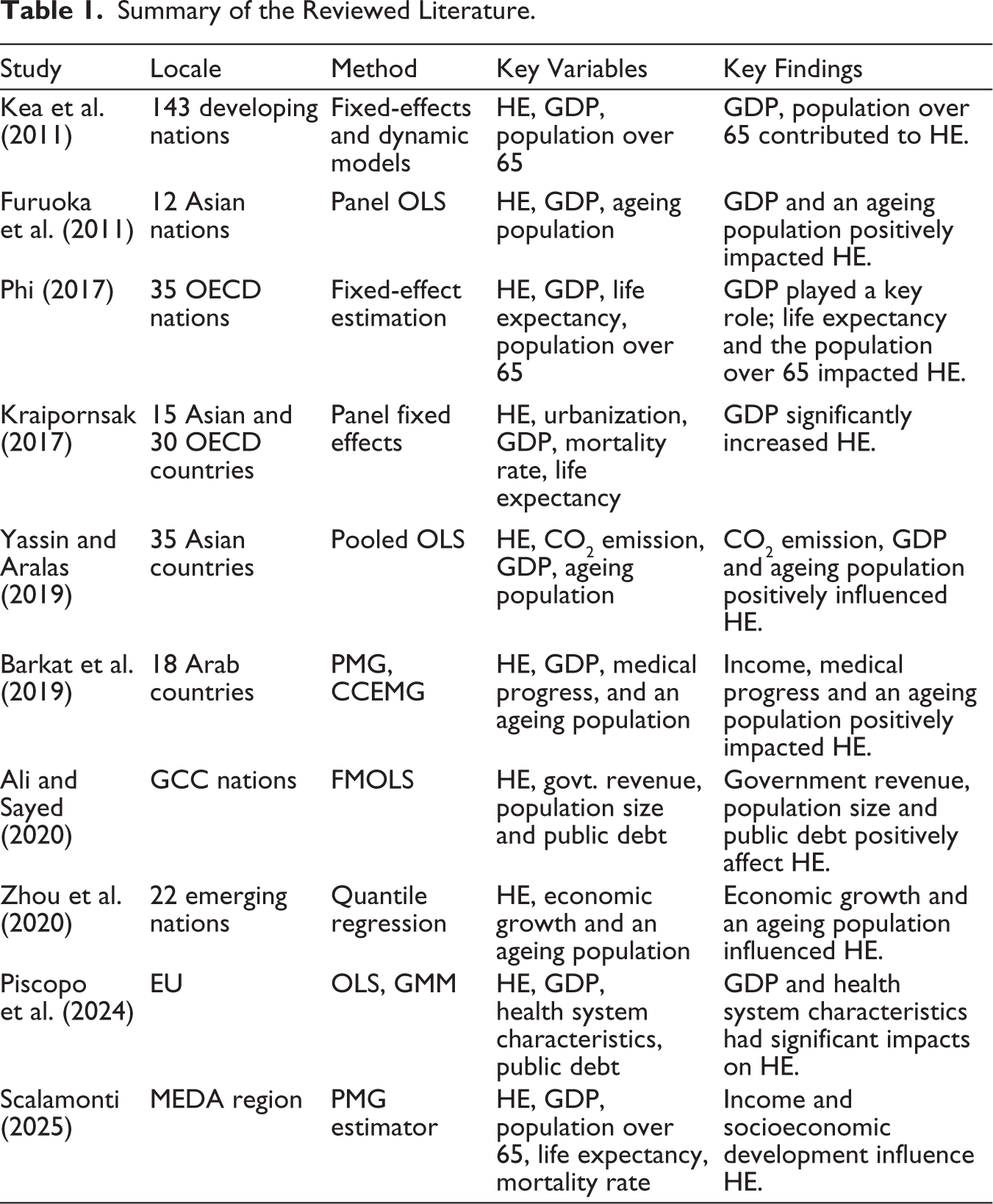
A plethora of literature is available on the determinants of health expenditures worldwide. We review the recent literature on these topics and draw our conclusions. Using panel ordinary least squares (OLS), Furuoka et al. (2011) explored the determinants of HE in 12 Asian countries between 1995 and 2008. They disclosed that GDP and an ageing population significantly positively impacted HE. Kea et al. (2011) considered 143 developing countries, data from 1995 to 2008, and both standard fixed effects and dynamic models to examine health expenditure in developing countries. Apart from income, many factors contributed to health expenditure, ranging from demographic factors to health system characteristics.
Kraipornsak (2017) examined the determinants of health expenditures in 15 Asian and 30 OECD countries, observing GDP as a key positive element, while price had an insignificant impact. Urbanization and out-of-pocket expenditure increased health spending, especially in the OECD. Better health outcomes increased spending in Asia but reduced it in OECD countries. Phi (2017) used fixed-effect modelling to investigate the determinants of health expenditures in 35 OECD countries from 2000 to 2013. She revealed that per capita GDP played a key role, while life expectancy and the population over 65 impacted health expenditure.
Barkat et al. (2019) examined the determinants of HE in 18 Arab countries from 1995 to 2015 using pooled mean group (PMG) and CCEMG techniques. They remarked that income, medical progress and an ageing population played significant roles in determining HE. Yassin and Aralas (2019) investigated data from 35 Asian countries from 1995 to 2010 and found that environmental externalities like CO2 and PM10 emissions positively influenced per capita health expenditure. Additionally, the ageing population and national income levels also impacted health spending.
Ali and Sayed (2020) examined the variables influencing government health spending in the GCC nations between 2005 and 2019. Using the FMOLS technique, they found that the healthcare spending per capita was positively correlated with government revenue, population size and public debt. However, considering the cross-sectional dependency among the GCC nations, the FMOLS estimation outcomes are unreliable, as they cannot account for the cross-sectional dependency. Zhou et al. (2020) looked at the factors that affected healthcare spending in 22 emerging nations between 2000 and 2018. Using the quantile regression technique, they discovered that economic growth and an ageing population influenced healthcare expenses in emerging nations. At the different quantile levels, however, the effects of industry, agriculture and technical development on health costs were notably diverse.
Amiri et al. (2021) conducted a comprehensive literature review to determine the determinants of HE at the national level and report their relevance. They identified a variety of factors that contribute to the emergence of health expenditure and pointed out that while the causes of HE have been extensively studied in high-income nations, very few studies have examined the problem as a whole in developing nations. Using air quality and healthcare data, Xia et al. (2022) analysed the short-term impact of air pollution on medical costs in Beijing. They reported that higher pollution levels and longer pollution episodes significantly enhanced healthcare visits and costs and highlighted that marginal health impacts grow with prolonged exposure, and ignoring this can underrate total health costs.
Kallestrup-Lamb et al. (2024) reviewed empirical literature on healthcare costs, observing that while age determines long-term care expenditure, time-to-death offsets ageing effects for hospital care. The impact of age and time-to-death on drug and ambulatory costs remains debated, with morbidity and medical innovation evolving as key factors in ageing-related expenditure growth. Piscopo et al. (2024) examined EU public health expenditure (2000–2018) using panel OLS and GMM, observing GDP as the main driver, while health system characteristics also had significant impacts. Election years and public debt had modest impacts, whereas ageing, political ideologies and citizens’ expectations were statistically insignificant. Scalamonti (2025) used the PMG estimator to investigate the drivers of per capita health expenditure in the MEDA region during 2000–2021. The study suffers from an improper estimation method as the PMG modelling cannot accommodate second-generation properties of the panel dataset. However, it concluded that, along with income, socioeconomic development also significantly influences health spending. A summary of the reviewed literature is portrayed in Table 1.
Summary of the Reviewed Literature.
The above-cited studies examined the determinants of health expenditures worldwide. They utilized different estimation methods, including panel OLS, fixed effects, PMG, generalized method of moments (GMM), common correlated effects mean group (CCEMG) and quantile regression. Most of them utilize the first-generation estimation process. Our study employs second-generation estimators, the augmented mean group (AMG) estimator and the CCEMG estimation. Most previous studies considered GDP and population over 65 as the common determinants of health expenditure. In a single study, we examine the environmental, social and economic factors that influence HE. Moreover, there is a dearth of studies on determinants of health expenditures in GCC countries. The only available study on the GCC nations, by Ali and Sayed (2020), suffers from several limitations. They used a first-generation fully modified OLS (FMOLS) estimator, which cannot account for cross-sectional dependency and slope heterogeneity, and remains doubtful. In contrast, we employ a second-generation AMG estimator, which accounts for second-generation properties of the data and remains robust and meaningful.
Thus, our study differs from all previous studies in the following ways. (1) For the first time, we employ a second-generation AMG estimator to examine the determinants of health expenditure. (2) We consider all economic, environmental and social determinants of health expenditure in a single model, whereas previous studies have considered them in part in separate studies. (3) This study represents the first attempt to examine the determinants of HE in the GCC countries using a legitimate estimation method. Previous studies employed inappropriate estimation methods, making them doubtful. Hence, this study examines the factors influencing health expenditure in the context of environmental pollution and economic growth, including an ageing population and educational attainment in the GCC countries.
III. Data and Methods
Data
This study is based on secondary data sourced from open sources. The annual consumption of healthcare goods and services is included in health expenditures, which are reported as a proportion of GDP. The World Bank (2024) provides data on health expenditures, CO2 emissions, GDP and population composition, while the UNDP (2024) provides data on education. Their availability determines the data span. Most data are available from 1990 to 2022. However, data on health expenditure have been available since 2000. Therefore, we have utilized data from 2000 to 2022 in this study.
Selection of Variables
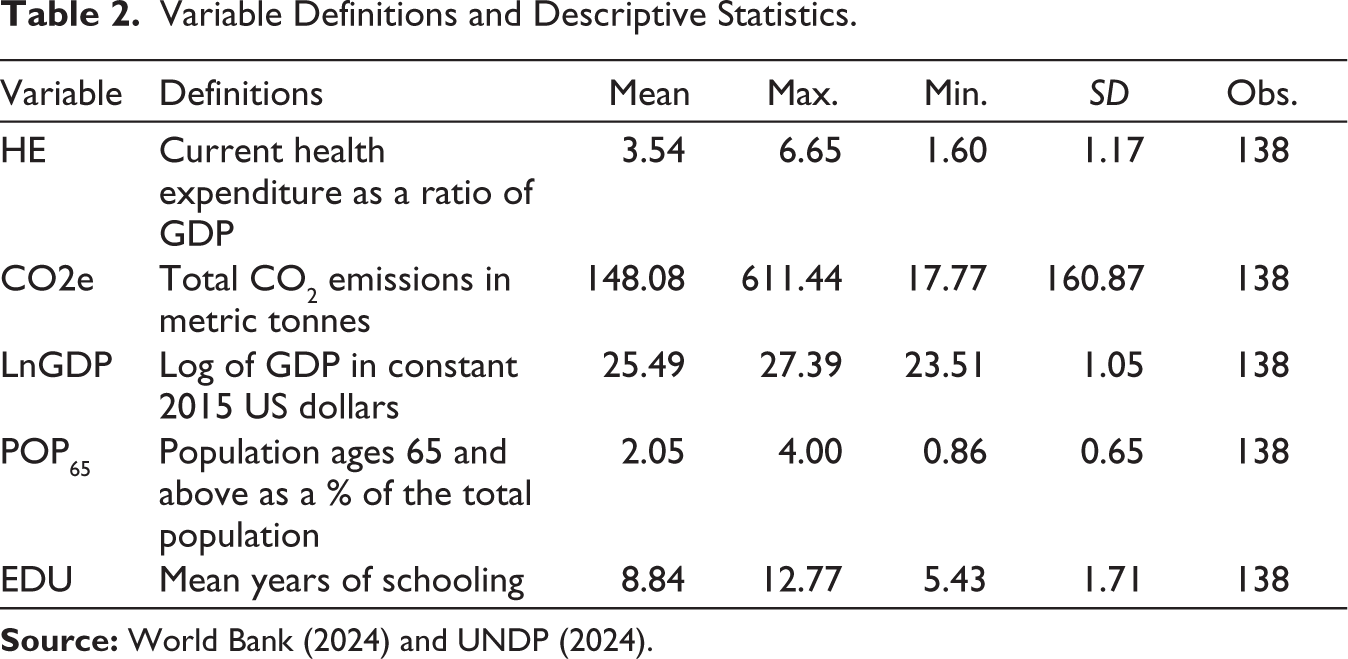
We have selected the variables based on an extensive literature survey. We have chosen the environmental factor (CO2 emissions) as an explanatory variable based on Yassin and Aralas (2019), Li et al. (2020) and Xia et al. (2022). Economic growth and population over 65 are considered based on Furuoka et al. (2011), Kea et al. (2011), Kraipornsak (2017), Phi (2017), Barkat et al. (2019), Yassin and Aralas (2019), Zhou et al. (2020), Piscopo et al. (2024) and Scalamonti (2025), among others. Education is incorporated as an independent variable following Yetim et al (2020), Raghupathi and Raghupathi (2020) and Moayedfard et al. (2020). Table 2 describes the variables, their definitions, data and descriptive statistics.
Variable Definitions and Descriptive Statistics.
Modelling and Estimation Strategy
This study examines the association between current HE and several economic, environmental, demographic and social indicators in six GCC member states in a panel data set-up. Equation (1) presents a model that encompasses the determinants of health expenditures.

Equation (1) provides a functional relationship between health expenditure and its determinants. Out of the five variables, only GDP has been transformed into a log form to make it comparable and facilitate ease of calculations. Equation (1) is further simplified and specified in Equation (2) for estimation purposes.

A panel data estimation strategy is employed to obtain values for the indicated coefficients in Equation (2). Therefore, verifying the pre-estimation requirements is essential for a panel of data.
Pre-estimation Tests
As a mandatory requirement, we assess whether the panel is free from cross-sectional correlations. Pesaran’s (2004) ‘cross-sectional dependency (CD)’ test assesses the dependency among the panel data. If CD is detected, we must employ second-generation tests to evaluate the data properties further. Assuming the existence of CD in the data, we use two different unit root tests: the Cross-section augmented Dickey–Fuller and the Cross-section augmented IPS (CIPS), as proposed by Pesaran (2007) and Pesaran et al. (2009), respectively.
Moreover, when considering panel data, we must check for slope heterogeneity among cross-sections. If slope heterogeneity is detected, typical panel estimation leads to unreliable statistics. Therefore, we employ two slope homogeneity tests: Pesaran and Yamagata (2008) and Blomquist and Westerlund (2013).
Main Estimation Methods
Assuming CD and slope heterogeneity in the data, we employ the AMG estimation developed by Eberhardt and Bond (2009) and Eberhardt and Teal (2010). The AMG estimation adjusts for CD and slope heterogeneity issues in the data.
AMG estimator uses the common dynamic effect parameter to retrieve any unobserved common factors ft in equation (2). Using a first-difference OLS equation, we describe the AMG estimator in equation (3) to capture the unobserved common factors.

where δˆt denotes the coefficient of time dummies, ∆ stands for the first-difference operator, and βi is the country-specific coefficient, and ft represents the unobserved common component. Equation (4) generates the AMG estimator by averaging the group-specific attributes across panels.
where δt is the estimation of δt. The AMG estimation method considers the slope heterogeneity, CD and unobserved factors.
Robustness Examination
Moreover, we cross-examine the AMG estimates by using the CCEMG estimation method (Pesaran, 2006), which follows a second-generation technique and accounts for the slope heterogeneity, CD and unobserved factors. We explain the CCEMG method in equation (5), including the unseen common factors, ft and the mean values of the dependent and independent variables.

where Yit and Xit are dependent and independent variables; βi represents the country-specific slope; ft stands for the unobserved common component with heterogeneous aspects; αi and ϵit are the intercept and error terms, respectively.
In addition, we assess the causal relationships among variables based on Dumitrescu and Hurlin’s (D-H) (2012) evaluation. The D-H evaluation accounts for heterogeneous panels with comparatively small N and large T. Equation (6) describes the D-H causality assessment and considers the cross-sectional variations:

Assuming that δi indicates the slope coefficient, βi denotes the lag parameter, and αi stands for the constant term. The following equation (7) describes the null and alternative hypotheses.

Under the null hypothesis, no causal relation exists among all cross-sections, but the alternative hypothesis assumes at least one causal relationship.
IV. Results and Discussions
CD Test Results
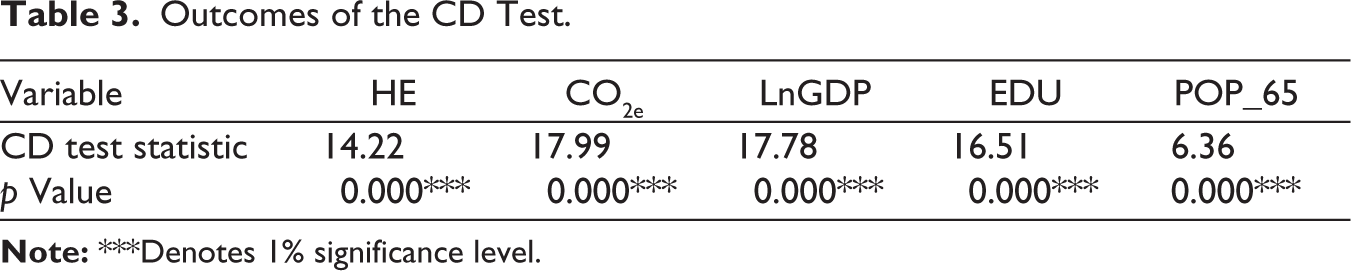
Pesaran’s CD test results are exhibited in Table 3 to examine the underlying null hypothesis, Ho: there is no cross-sectional dependence. The test statistics and their corresponding p values confirm the presence of mutual dependence of the cross-sections. Hence, the first-generation econometric experiments are ruled out.
Outcomes of the CD Test.
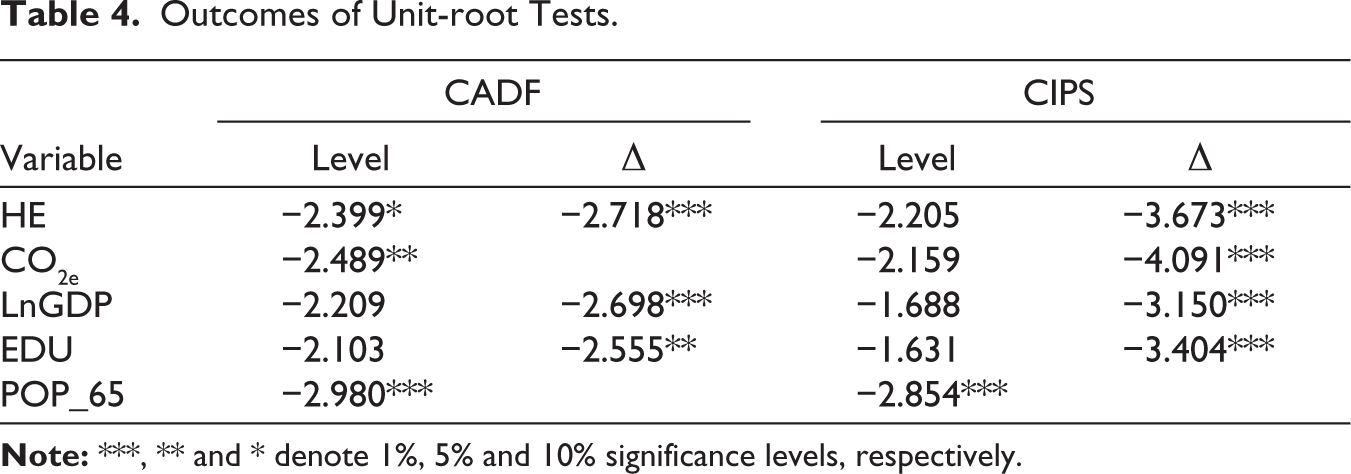
Based on the CD test outcomes, we follow the second-generation unit-root test strategy described in the Methodology section. The CADF and CIPS tests are implemented to examine the underlying null hypothesis, Ho: the variables have a unit root, and their results are presented in Table 4. The results indicate that the variables do not exhibit a unit root and follow mixed order integration, revealing their stationary features at both the level and the first difference.
Outcomes of Unit-root Tests.
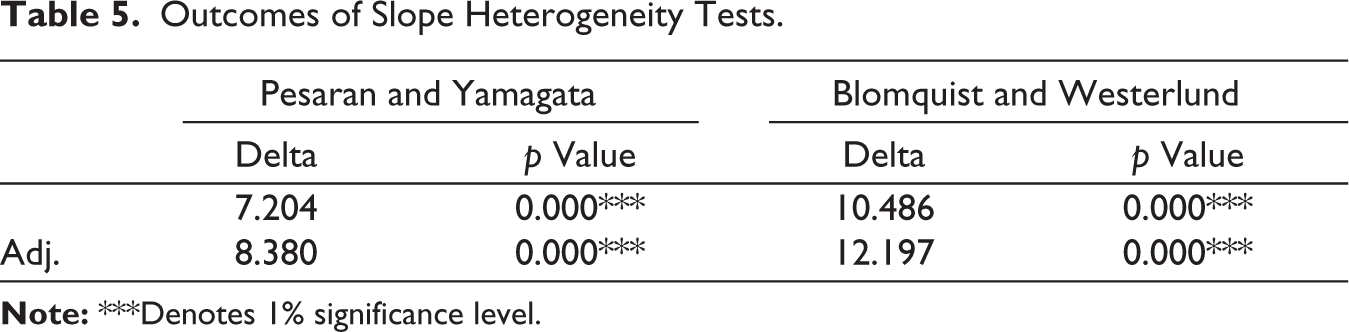
We have further implemented Pesaran and Yamagata, as well as Blomquist and Westerlund slope heterogeneity tests, to examine slope variations across GCC nations. Table 5 demonstrates the outcomes of the two tests. The value of delta and its p value rejects the slope homogeneity assumption and confirms the slope variations among the GCC nations.
Outcomes of Slope Heterogeneity Tests.
AMG Estimation Results
We have applied regression with the AMG estimation using the robust trend specification, generating the following outcomes in Table 6. The common dynamic process (Cdp), trend and constant term coefficients are significant at the 1% level, justifying an appropriate model specification.
Outcomes of the AMG Estimation; Dep Variable: HE.
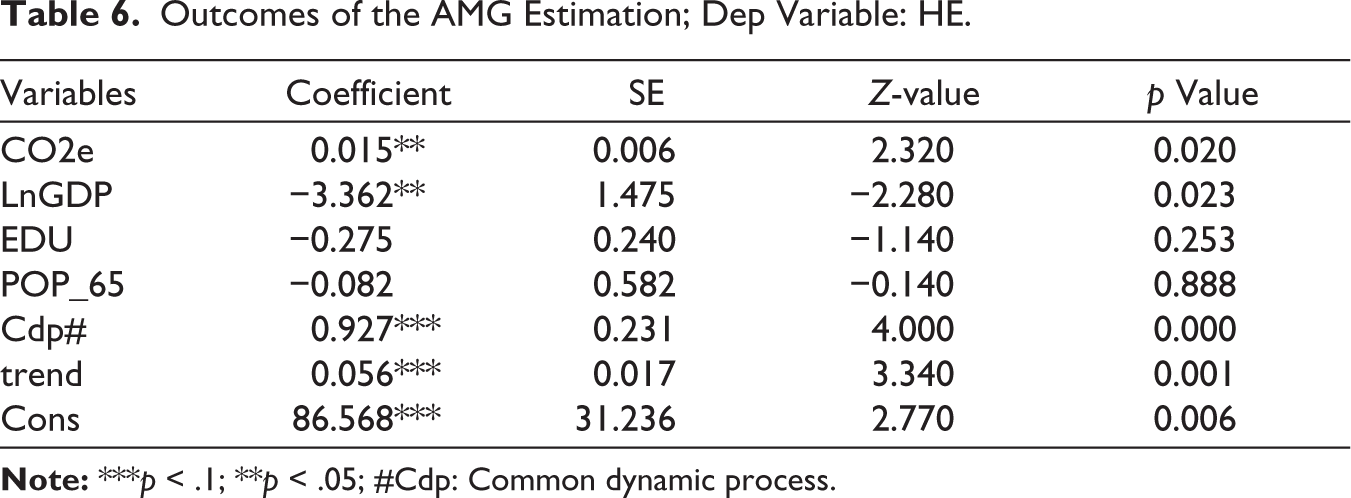
The estimated coefficient of CO2e (0.015) is statistically significant at the 5% level. A one metric tonne rise in CO2 emissions correlates with a 0.015 increase in the health expenditure as a share of GDP. This suggests that higher emissions may result in increased health costs, potentially due to pollution-related illnesses. Empirical data suggest that environmental pollution has been a key factor in rising healthcare expenses in GCC nations. Any upward trend in CO2e data will likely drive HE even higher. Our finding aligns with Yassin and Aralas (2019), Li et al. (2020) and Xia et al. (2022), who also reported the contributory impact of CO2e on HE. Given GCC countries’ higher air pollution levels than the global average (Farahat, 2022; Marmore, 2017), our findings generate several key policy implications that include strengthening environmental regulations, investing in green technologies, increasing public awareness, incorporating pollution data into health planning and strengthening regional cooperation for air quality management throughout the GCC nations.
The coefficient of LnGDP (−3.362) is significantly negative at the 5% level, suggesting a negative impact on HE. A 1% increase in GDP results in a decrease in health expenditure (as a percentage of GDP) by approximately 3.362 × 0.01 = 0.0336 percentage points, assuming CO₂ emissions remain constant. This suggests that as economies expand, the proportion of health spending relative to GDP may decrease, potentially due to efficiency improvements. Unlike many countries, economic growth has been a blessing in helping to offset rising health expenditures. Therefore, future economic growth is likely to offset the rising health expenditures. Our finding is unique and contrasts with findings by most studies in the literature, such as Furuoka et al. (2011), Kea et al. (2011), Kraipornsak (2017), Phi (2017), Barkat et al. (2019), Yassin and Aralas (2019), Zhou et al. (2020), Piscopo et al. (2024) and Scalamonti (2025), who witnessed positive impacts of economic growth on HE. Given the negative association between economic growth and HE, policymakers in the GCC nations should use future economic growth to reduce health spending by encouraging efficiency, investing in preventive care and firming health system management.
The coefficient of EDU is negative but statistically insignificant, suggesting that education has no significant influence on healthcare spending in GGC countries. Typically, education influences healthcare spending by shaping health behaviours, enhancing access to care and improving decision-making. Higher education levels lead to better health awareness, increased use of preventive services and more efficient healthcare utilization, resulting in greater healthcare spending. However, our finding contrasts with those of Yetim et al. (2020), Raghupathi and Raghupathi (2020) and Moayedfard et al. (2020), who found a positive impact of education on healthcare spending. Given the insignificant impact of education on HE in GCC nations, policymakers should review the effectiveness of current educational programmes in shaping health behaviours and consider targeted health education initiatives to better influence healthcare utilization.
The coefficient of POP_65 is negative and highly insignificant, showing that it does not influence health spending. The working-age population (15–64) comprises 75.21% of the total, while the population 65 and over comprises only 2.05% of the total in GCC countries during the study period (World Bank, 2024). Since POP_65 comprises an insignificant share of the total population, it does not influence the region’s healthcare spending. Therefore, the ageing population has not been a concern in the region. Our finding, hence, contrasts with Furuoka et al. (2011), Kea et al. (2011), Phi (2017), Barkat et al. (2019), Yassin and Aralas (2019), Zhou et al. (2020) and Kallestrup-Lamb et al. (2024), who highlighted the positive impact of POP_65 on HE. However, our finding aligns with Piscopo et al. (2024), who revealed that an ageing population did not cause health expenditures.
Robustness Test Results
The robustness of the AMG outcomes is evaluated employing the CCEMG estimation. The robust trend specification is employed in implementing the CCEMG estimation, and its outcomes are displayed in Table 7.
Outcomes of the CCEMG Estimation; Dep Variable: HE.
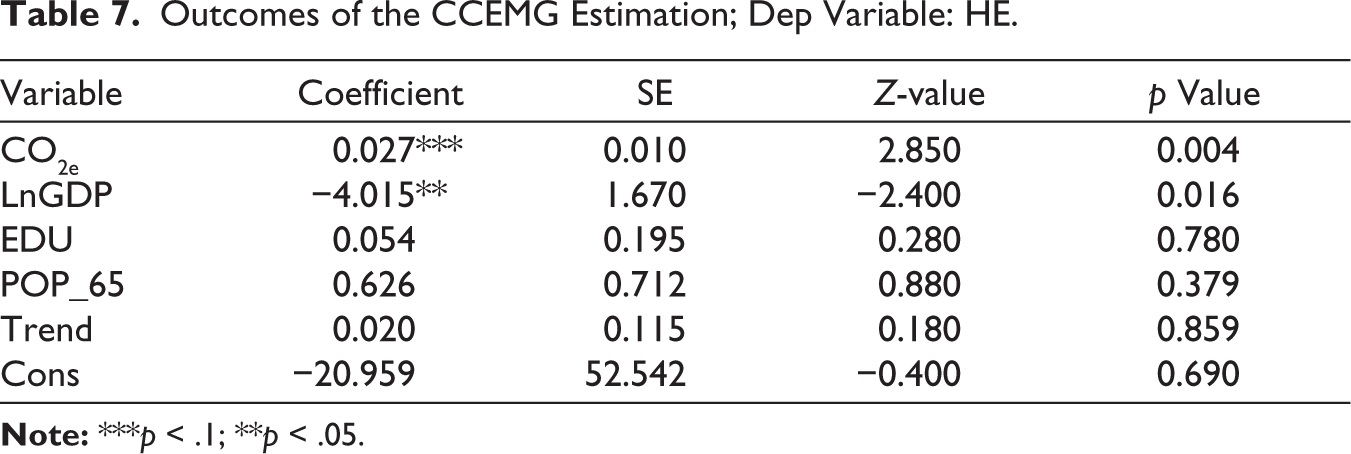
The key outcomes of the CCEMG estimations are similar to those of the AMG estimation findings. A positive and significant correlation coefficient of CO2e reinforces the AMG finding that environmental pollution is a contributing factor to rising healthcare spending. Similarly, a negative and significant coefficient of LnGDP reinforces the notion that economic growth harms healthcare spending, helping to reduce the growth of healthcare costs. Both education and the population 65 and over remain insignificant in determining HE. Thus, the CCEMG estimation validates the robustness of the AMG estimation outcomes.
Moreover, the D-H causality test is employed in addition to AMG and CCEMG estimations to check the causal directions. The outcomes of the D-H causality test are pronounced in Table 8.
Outcomes of the D-H Causality Assessment.
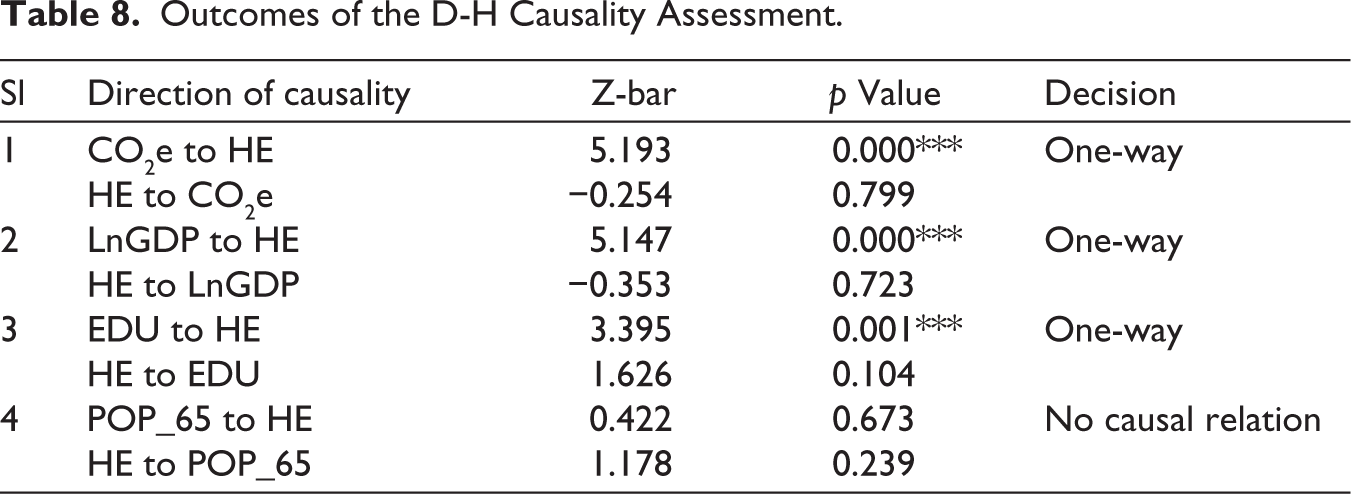
We have reported four causal relationships in Table 8. The first and second causal relationships clearly support the findings of AMG and CCEMG estimations. A one-way causal association appears to exist between CO2e and HE, indicating that environmental pollution affects health expenditures. The opposite causality is ruled out.
The second causal link occurs from LnGDP to HE, indicating that economic growth leads to increased healthcare spending. The opposite is not true. These two one-way causal relationships support the main econometric findings and prove their robustness.
The fourth item shows no causal link between the 65-and-over population and HE, indicating that an ageing population does not cause HE. However, in the third item, unidirectional causality runs from EDU to HE, which differs from the main econometric finding. It is to be noted that a causal relationship is a short-run analysis, while AMG and CCEMG estimation provide long-run relationships. A variation between short-run and long-run coefficients is a usual phenomenon. Hence, one-way causality from education to HE does not oppose the primary econometric outcomes.
V. Conclusions and Policy Implications
This study provides a comprehensive and nuanced understanding of the determinants of healthcare spending in the GCC nations, offering insights that challenge conventional findings and emphasize the importance of region-specific analysis. Among the key findings, environmental pollution—measured through CO₂ emissions—is a significant driver of increasing HE. This finding aligns with global evidence and underlines a critical issue for the GCC, where pollution levels surpass the global average. The policy implications are obvious: GCC nations must strengthen their efforts to mitigate environmental pollution through rigorous regulations, investment in green technologies and coordinated regional policies to monitor and control environmental pollution.
In contrast, economic growth in the GCC nations leads to reduced healthcare spending, a finding that differs from most global studies. This suggests that, in the unique economic perspective of the GCC countries—characterized by high incomes, publicly financed healthcare and efficiency gains—economic development may improve resource allocation and reduce the burden on health systems. Policymakers should capitalize on this dynamic by directing economic gains towards preventive care, strengthening healthcare facilities and promoting cost-effective health system management.
Additionally, the study reveals no statistically significant correlation between education and healthcare spending in the GCC countries, despite the potential influence of education on health spending through improved health practices and system navigation. This finding suggests that existing educational initiatives may not have a significant impact on healthcare utilization, necessitating a reassessment of the role of education in health policy. Targeted health education and awareness initiatives may be necessary to translate educational attainment into meaningful health outcomes and cost implications.
Finally, the ageing population in the GCC countries is currently too small to have a discernible impact on healthcare spending. The demographic structure remains youthful, with only a small portion of the population aged 65 and older, which explains why ageing has a relatively small impact on health spending trends. Although this result aligns with today’s demographic reality, it also highlights the importance of being prepared for the future, as ageing is expected to increase over the next several decades.
Overall, this study emphasizes the importance of contextualized health policy in the GCC nations. Environmental sustainability, effective use of economic growth, enhanced health education initiatives and demographic planning for the future must be the foundations of a strong healthcare system. Implementing policies that align with these results may help GCC nations improve the sustainability of their healthcare systems and address their particular economic, social and environmental concerns.
The study’s policy implications suggest that GCC countries strengthen environmental regulations, invest in green technologies, increase public awareness, incorporate pollution data into health planning, and foster regional collaboration to improve air quality management. Governments can use economic growth to lower HE by enhancing system effectiveness, prioritizing preventive care and strengthening healthcare administration. Current educational programmes may be re-evaluated and redesigned to shape health behaviours better and influence healthcare utilization. Health policy can continue to prioritize the needs of the working-age population while monitoring future demographic shifts, as the ageing population’s impact is relatively minimal.
Although this study offers valuable insights into the factors influencing healthcare spending in the GCC, it is essential to acknowledge its limitations. First, the study is based on aggregate national-level data, which may obscure significant within-country differences and restrict the granularity of insights on population subgroups or regional differences. Second, data limitations prevented the inclusion of several potentially significant characteristics, such as insurance coverage, the quality of the healthcare system, and lifestyle-related risks, such as smoking, which could have limited the model’s comprehensiveness.
Future studies may overcome these constraints by incorporating disaggregated data, such as additional environmental and health factors, to enhance the resilience of the findings. Furthermore, longitudinal research examining how an ageing population may impact healthcare spending in the future will be essential as the region’s demographic composition changes. Researchers may also evaluate the quantifiable health and cost consequences of environmental regulations and investigate the efficacy of targeted health education initiatives. Comparative investigations with other high-income or oil-dependent economies may also offer valuable context for illuminating the unique dynamics observed in the GCC nations.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Data Availability
Data are available at the following open repositories:
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.