
Abstract
Objectives: This study aimed to determine the prevalence and underlying sociodemographic correlates of smoking among Sri Lankans. Methods: A cross-sectional sample (N = 5000, age >18 years) was selected using a multistage random cluster sampling. Data were collected using an interviewer-administered questionnaire. Results: Response rate was 91% (n = 4532); males 40%; mean age 46.1 years (±15.1). Overall, urban and rural prevalence of current smoking (smoking) was 18.3%, 17.2%, and 18.5%, respectively (P = nonsignificant, urban vs rural). Smoking was much higher in males than in females (38.0% vs 0.1%, P < .0001). Ex-smokers comprised 10.0% (males 20.7%, females 0.1%, P < .0001). Among the smokers 87.0% smoked <10 cigarettes per day. The male age groups < 20 and 20 to 29 years had the lowest (15.6%) and the highest (44.6%) prevalence of smoking, respectively. In males, smoking was highest in the least educated (odds ratio = 1.96, P = .001). Conclusions: Smoking is common among Sri Lankan males and is associated with lower education, income, and middle age.
Introduction
Tobacco smoking is one of the most important risk factors for cardiovascular disease (CVD), obstructive pulmonary disease, malignancies of the respiratory and upper gastrointestinal tract, and causes death among millions of people worldwide. 1 It is becoming an important health problem in the developing countries. 2 Thus smoking has become one of the leading preventable causes of death for the present-day humankind both rich and poor. 3
Because of the addictive properties of tobacco, a majority of the smokers find it difficult to quit, even when they develop smoking-related diseases.4,5 The World Health Organization has proposed a Framework Convention on Tobacco Control (FCTC
Sri Lanka is a middle-income country in South Asia with better health indicators Ecompared with other countries in the region despite a low annual per capita gross national product. 7 The population of Sri Lanka has undergone a demographic transition with a consequent epidemiological transition. 8 CVD has become the leading cause of death among Sri Lankan adults (Ministry of Health, Sri Lanka, 2005). Nevertheless, tobacco industry has continued to promote smoking among the females and the youth in Sri Lanka using innovative marketing strategies. These strategies include using attractive young girls to promote smoking during festivals, in places frequented by youth (shopping malls, discos, and campuses), sponsoring messages of child safety around schools, 9 and rewarding journalists for not promoting antismoking in newspapers. 10
Several groups have reported on the prevalence of smoking among adults in Sri Lanka in the past. In 1994, smoking prevalence among middle-aged men in the Central Province was reported as 57.9%. 11 Another study carried out in Colombo suburbs in 2002 reported male smoking prevalence as 29.8%. 12 A recent study in southern Sri Lanka reported the prevalence of daily smoking among men and women as 21.1% and 0.6%, respectively. 13 The prevalence of current smoking among Sri Lankan immigrants in Norway has been reported as 19% (n = 603) in males and 0% (n = 398) in females. 14 In the neighboring countries in South Asia, smoking prevalence in males and females have been reported as 29.3% and 2.3%, respectively, from India 15 and 28.6% and 3.4%, respectively, from Pakistan. 16 The majority of the above studies on smoking in Sri Lanka have reported smoking prevalence in middle-aged men in a single city or province. The smoking patterns may change because of the efforts of the tobacco industry as well as because of the changing lifestyles. National-level data assessing the current status of smoking among adults in Sri Lanka are essential for surveillance and timely interventions.
The aims of the study were to determine the prevalence of tobacco smoking among adults and to examine the sociodemographic correlates of smoking in Sri Lanka. Effects of known CVD and risk factors on smoking are also assessed.
Methods
This study was approved by the Ethical Review Committee of the Faculty of Medicine University of Colombo as a wider study on diabetes, CVD, and their risk factors. It was carried out between 2005 and 2006. All participants provided informed written consent.
Study Population
The study was conducted in 7 out of the all 9 provinces in Sri Lanka. The methods of sampling and data collection have been previously reported in detail. 17 The total sample frame was approximately 14 million people living in 12 018 “village office units” (the smallest government administrative unit). A multistage random cluster sampling technique was used to select a nationally representative sample of 5000 people equal to or older than 18 years from the noninstitutionalized civilian population in Sri Lanka. The sample size was corrected for the clustering by multiplying by a factor of 2 (for the design effect). The sample size of each province and the rural and urban samples of individual provinces were determined using a probability proportional to size technique. The sample was recruited from 100 clusters of 50 households in each. A cluster size was determined as 50 households to achieve a satisfactory spread of all sociodemographic and ethnic groups in Sri Lanka. Clusters were selected by a computer-generated random number list from the “village office Units.” Voters’ lists were used to randomly select the first household of each cluster and a uniform criterion was used to select the remaining 49 households in all 100 clusters. An eligible adult equal to or older than 18 years was randomly selected from each household by visiting households. Those who were pregnant, acutely ill, or who declined participation were excluded.
Data Collection
A trained group of medical graduates collected data using a pretested interviewer-administered questionnaire. Interviews were conducted in the mother tongue of study participants. Information regarding sociodemographic factors, medical history, and smoking status was recorded.
Terms and Classifications
Participants were asked whether they “smoke now, used to smoke, or never smoked.” Those who were smoking were categorized into 4 subcategories according to the number of cigarettes/tobacco products smoked per day as ≤1per day, 2-10 per day, 11-20 per day, and >20 per day. Participants were considered to be current smokers if they were smoking any form of tobacco (cigarettes, bidi, or cigars) either every day or on some days at the time of the study or within the preceding 6 months. Those who had successfully quit at least 6 months before the data collection were considered ex-smokers and those who have not smoked tobacco were considered never smoked. Income levels were categorized based on monthly family income in Sri Lankan rupees (LKR). Educational level was categorized into 3 categories based on number of years of full-time education (school or higher education). Occupational categories were based on the International Standard Classification of Occupation (ISCO 88; International Labour Organisation, 1991).
Statistical Analysis
All data were double-entered and cross-checked for consistency. Data were analyzed using Stata/SE 10.0 (StataCorp LP, College Station, Texas) and SPSS version 14 (SPSS Inc., Chicago, IL) statistical software packages. Point estimates for the prevalence of smoking were obtained using the Stata survey data analysis adjusting for the stratified cluster sampling model. Samples weights were assigned to account for the differences in household, cluster level, and gender-specific response. Age-specific and gender-specific prevalence of smoking was calculated for the whole population, urban and rural sectors. Data are presented as percentages and 95% confidence intervals (CI) whenever appropriate. χ2 statistics was used to compare the differences between categorical variables. Multiple logistic regression analysis was performed to examine the association of underlying factors for current smoking among males but not in females because of the very low prevalence of smoking in women. P values <.05 were considered significant.
Results
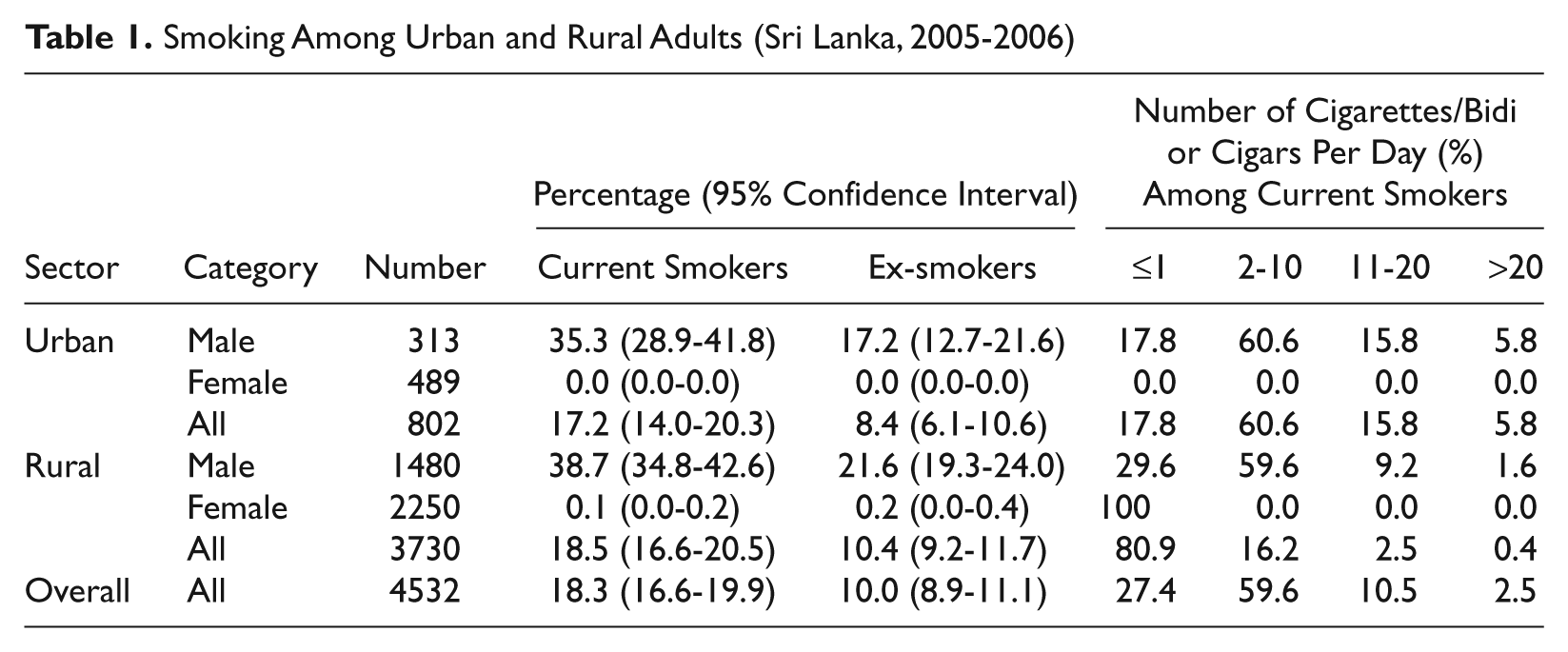
Of the 5000 people selected, 4532 participated (response rate 91%). The mean age of the sample was 46.1 ± 15.1 years; 40% (n = 1793) were males and 18.0% (n = 802) were from urban areas (21% of the Sri Lankan population is urban). Overall, 18.3% were current smokers (Table 1). Smoking was much higher in males (38.0%) than in females (0.1%; P < .0001; Table 2). The prevalences of current smoking in the urban population and rural populations were 17.2% and 18.5%, respectively (P = nonsignificant, urban vs rural). There were no significant differences in gender-specific smoking between the urban and rural sectors (Table 1). Ex-smokers comprised 10.0% of the total sample (males, 20.7%; females, 0.1%; P < .0001; Table 2).
Smoking Among Urban and Rural Adults (Sri Lanka, 2005-2006)
Tobacco Smoking Status Among Adults According to Age and Gender (Sri Lanka, 2005-2006)
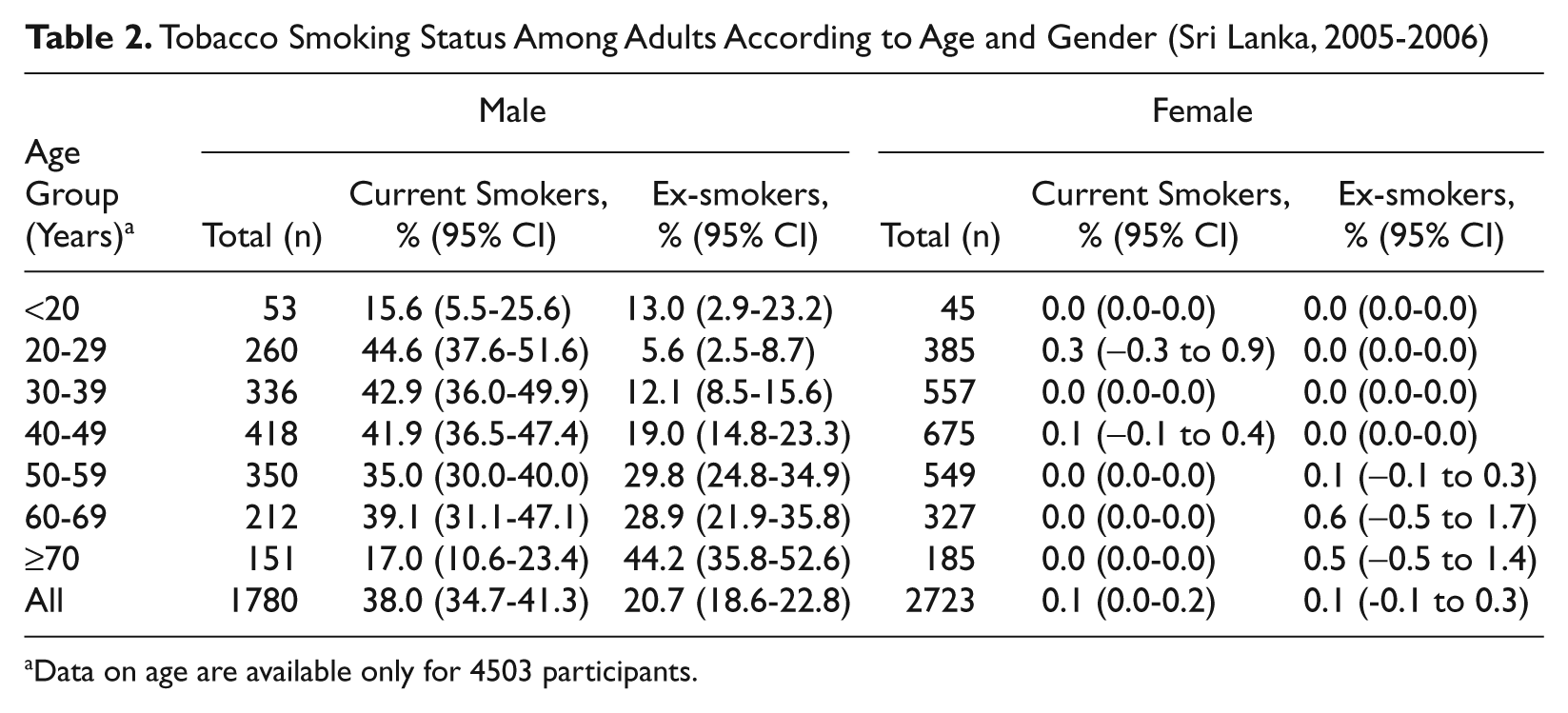
Data on age are available only for 4503 participants.
Age-Specific and Sector-Specific Smoking
The highest prevalence of smoking in males was seen in the 20- to 29-year age group followed by the 30- to 39-year and 40- to 49-year age groups (Table 2). The lowest prevalence was seen in those <20 years followed by ≥70-year age group. Among females, tobacco smoking was <1.0% in all age groups. Higher prevalence of ex-smokers was seen among older adults.
Severity of Smoking
In Sri Lanka, the majority of the male smokers smoked <10 cigarettes per day (Table 1). Male smokers in urban areas smoked higher number of cigarettes per day compared with those from rural areas. All female smokers smoked ≤1 cigarette per day.
Association of Level of Education, Income, and Occupation With Smoking
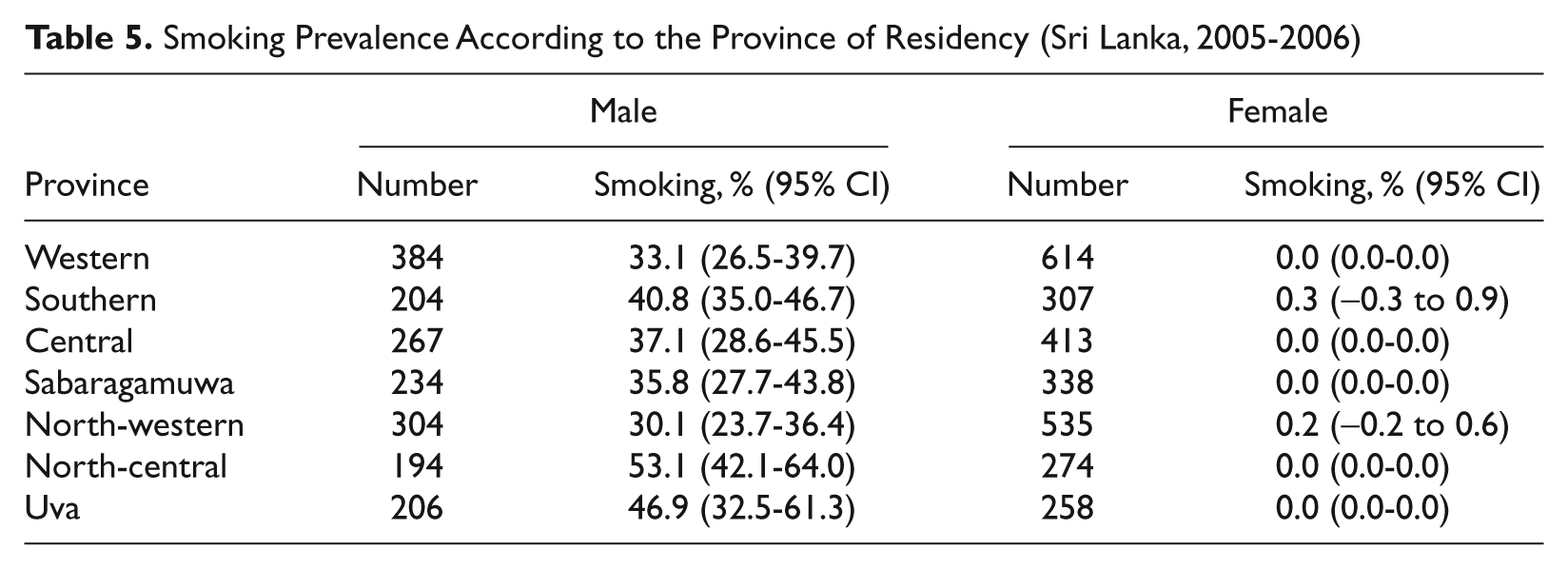
In males, smoking was highest among those with lowest levels of education (odds ratio [OR] = 1.96) and income (OR = 1.33) compared with the highest level of education and income, respectively (Table 3). Among male occupational categories, smoking was lowest among professionals followed by the unemployed (Table 4) and was highest among senior managers and officials. Among females, current smoking was reported only in those engaged in craft/related work and agriculture/fisheries related work. In the income category, the highest male smoking prevalence was seen among those with the lowest income followed by the next level of income (Table 4). In the 7 provinces in Sri Lanka, the smoking prevalence in males was highest in the North-Central and Uva provinces where the majority of the male population is engaged in agriculture (subsistence farming) or labor-related occupations with lower levels of education and income (Table 5). Among females, smoking was <1.0% in all income groups.
Results of Logistic Regression Analysis for Covariates of Current Smoking in Men
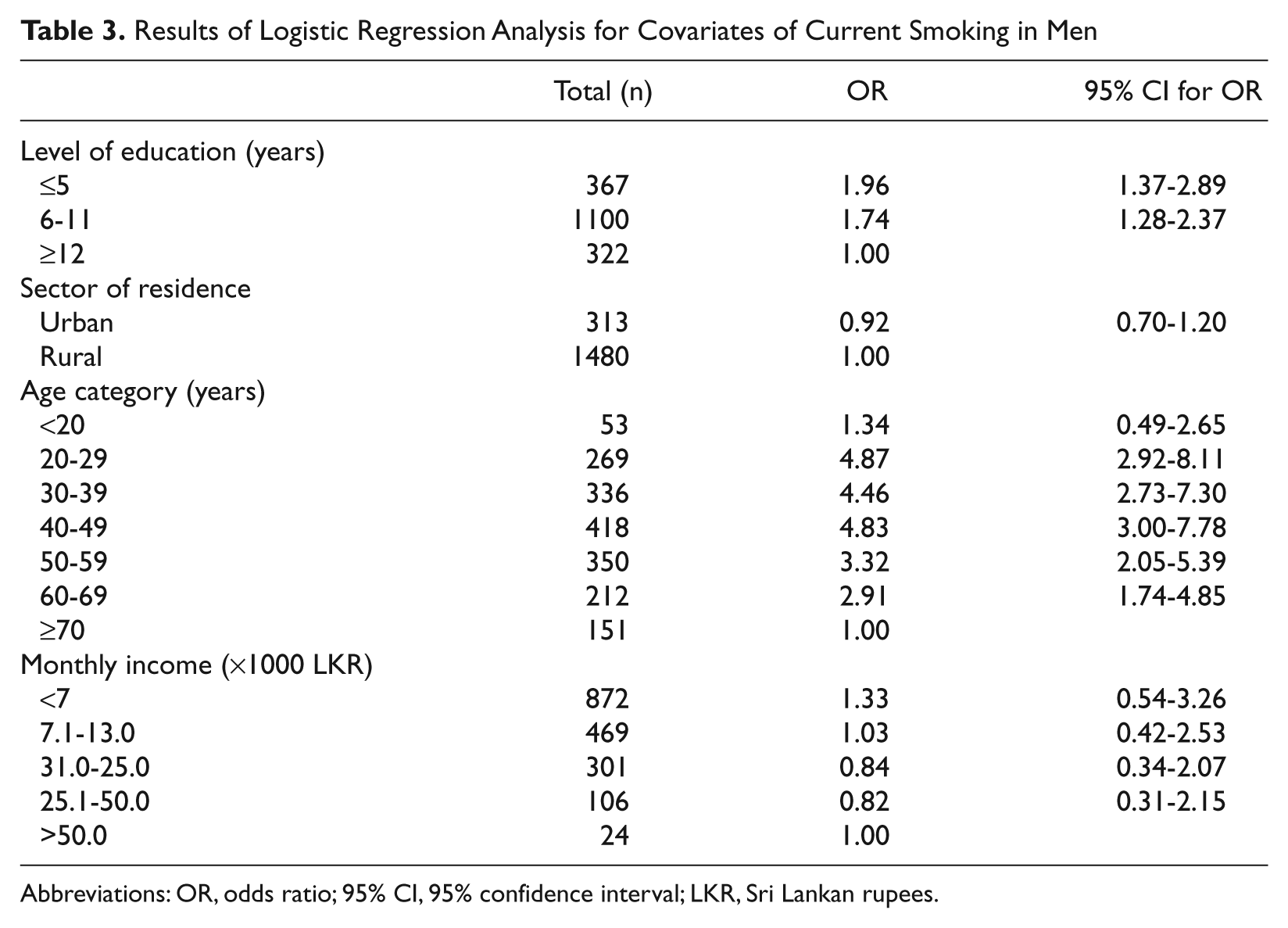
Abbreviations: OR, odds ratio; 95% CI, 95% confidence interval; LKR, Sri Lankan rupees.
Prevalence of Smoking According to the Level of Education, Occupation, and Income Among Adults (Sri Lanka, 2005-2006) a
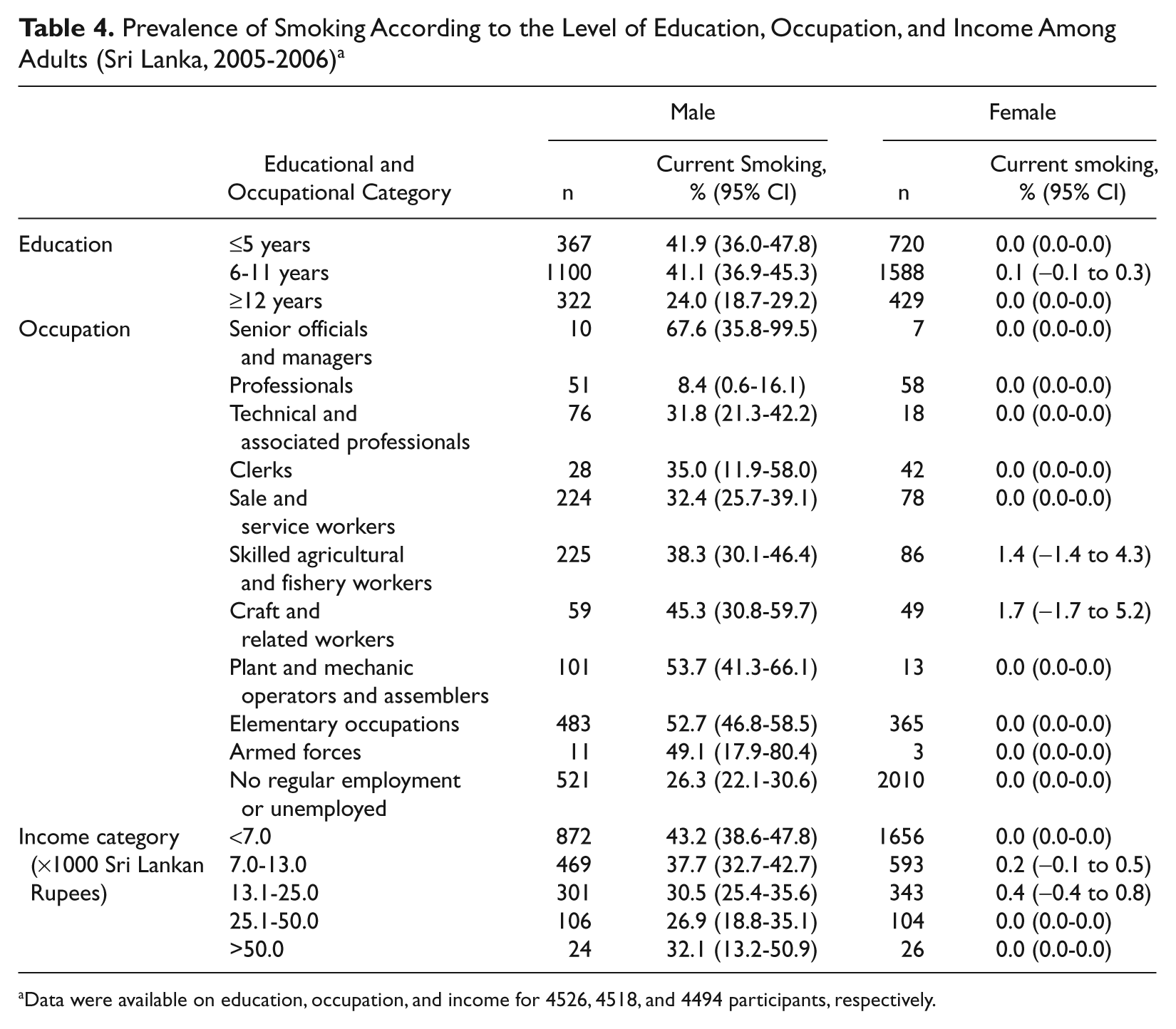
Data were available on education, occupation, and income for 4526, 4518, and 4494 participants, respectively.
Smoking Prevalence According to the Province of Residency (Sri Lanka, 2005-2006)
Association of Ischemic Heart Disease and Cardiovascular Risk Factors With Smoking
About one fifth of males with known ischemic heart disease (IHD) or risk factors continued to smoke compared with those without: IHD (17.6% vs 39.2%, P = .003), diabetes (26.0% vs 39.0%, P = .01), hypertension (15.1% vs 41.4%, P < .0001), and hypelipidemia (12.9% vs 39.6%, P = .0001).
Discussion
This study was conducted in 7 out of all 9 provinces in Sri Lanka and included urban and rural areas and all adult age groups above 18 years. We have also considered the stratified cluster sampling method of recruitment in the data analysis. Therefore, the data can be generalized to the Sri Lankan population. Inclusion of all forms of tobacco smoke (cigarette, bidi, and cigars) together as cigarette smoking, noninclusion of smokeless (oral) tobacco and collecting data through interviews rather than from self-administered questionnaires when smoking is considered a social taboo were limitations. However, in the study among Sri Lankan immigrants living in Norway where smoking is not considered a social taboo, a zero prevalence has been reported among 398 women. 14 The effect of gender imbalance especially in the urban sample, which was because of more men being productively employed compared with women was minimized by adding sample weights in the final analysis. According to the Centers for Disease Control and Prevention in the United States anyone who had smoked more than 100 cigarettes in their lifetime and continues to smoke every day or some days is defined as a current smoker. 18 Because a minimum number of cigarettes smoked during lifetime was not a prerequisite for the definition of current smoker in our study, there is a possibility of overestimation of current smoking.
According to this large nationally representative study, the current smoking prevalence is 38.0% among males and 0.1% among females older than 18 years in Sri Lanka. The present data compare well with a study published in 2005 showing 41.0% yearly, 27.8% monthly, and 21.0% daily smoking among males. 13 In the same study, daily smoking among women has been reported as 0.6%. According to a study conducted in Sri Lanka by the WHO in 2003, current daily smoking among males was lower (23.2%) than and females higher (1.7%) than the current smoking prevalence reported here. 19 Our study, the study by Perera et al, 12 and the WHO study in 2003 all have shown lower smoking prevalence compared to the prevalence of 57.9% of current smoking in middle-aged men in 1994. 11 Male smoking prevalence in Sri Lanka was higher than for India (29.3%) 15 and Pakistan (28.6%). 16 Female smoking in Sri Lanka was much lower than most of the developed countries such as the United States (20.0%) 20 and the United Kingdom (24.5%) 21 and the developing countries in Asia such as India (2.3%), 15 Pakistan (3.4%), 16 and Malaysia. 22 According to the World Health Organization, 2007, female smoking prevalence in Sri Lanka is among the lowest in the whole world.
In Sri Lanka, the 20- to 29-year age group had the highest age-specific prevalence of smoking in males. The studies conducted in India (40- to 49-year age group) and Pakistan (25- to 44-year age group) have shown the highest prevalences of male smoking in older age groups.15,23 Similar to the present study, low prevalence of smoking among younger age groups have been reported from other South Asian countries.15,23
Our study shows that the tobacco smoking is higher among groups with lower levels of income, education, and those engaged in blue-collar work (except in the small number of senior officials and managers). In the International Tobacco Control Four Country Survey (ITC-4) conducted in the United States, Canada, the United Kingdom, and Australia, lower levels of education and income have been shown to be associated with higher nicotine dependence and lower tendency for quitting. 24 In addition to the health problems causing increased morbidity and mortality among the productive males, smoking drains out much of the economic resources in low-income families in developing countries, leading to a vicious social cycle of poverty and poor health by depriving the younger generation of nutrition and education. Supporting these conclusions, studies have shown that lower income was associated with smoking-induced deprivation 25 and that successful quitting is associated with significant lowering of financial stress and enhancement of material well-being. 26
Among smokers in Sri Lanka, only 13.0% smoked ≥10 cigarettes per day compared with 16% of British smokers who were categorized as hardcore smokers 27 and 15.1% in Italy who smoked more than 15 cigarettes per day. 28 In Sri Lanka, medical professionals make strong recommendations for smoking cessation for those who develop IHD or risk factors. This may be the reason for the lower prevalence of smoking seen in those with IHD or risk factors. However, about one fifth of males with IHD or risk factors continued to smoke suggesting only partial effectiveness of the efforts by health care professionals. Lack of a formal quitting program with nicotine replacement may also be a contributing factor as the addictive properties of nicotine make quitting difficult.
Low prevalence of smoking among Sri Lankan women in this study is consistent with the studies conducted among Sri Lankan females living in Western countries. 14 Although there is little research into the normative behavior, the strict culturally defined nonsmoking norm among Sri Lankan women over successive generations might be protecting them from this epidemic despite changes of lifestyle and specific marketing strategies aimed at women. 9
The cancer incidence data for year 2000 from the Government Cancer Institute in Sri Lanka reported 509 cases of lung cancer in males compared with 134 in females (male/female ratio 3.8; National Cancer Control Programme, Sri Lanka, 2000). In the United Kingdom and the United States, the prevalence of smoking in women is almost equal to that in males.20,21 In those born in England and Wales, the male/female ratio for lung cancer is 1.5, 29 whereas that in the white population in the United States was reported to be 1.0 in 1997-2000. 30 Therefore, it is highly likely that in Sri Lanka the higher prevalence of smoking in males is contributing to the higher male:female ratio of lung cancer. Further studies are needed to verify this as well as to examine the other health hazards (CVD and chronic lung disease) of smoking among males in Sri Lanka.
Conclusions
Tobacco smoking among adults in Sri Lanka is predominantly a problem in males and more than one third of them currently smoke tobacco. The higher incidence of lung cancer in Sri Lankan males compared with females demonstrates the health hazards of smoking in men. Sri Lankan females should be commended for low levels of smoking. Further studies on the underlying factors of lower prevalence of female smoking may help apply such knowledge to other populations. Interventions for smoking in Sri Lanka need to be designed to target males with lower levels of education, low income, and those who continue to smoke despite having IHD or high CVD risk.
Footnotes
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
The authors disclosed receipt of the following financial support for the research and/or authorship of this article:
National Science Foundation of the Ministry of Science and Technology of Sri Lanka
Oxford Centre for Diabetes, Endocrinology & Metabolism, Oxford, UK
NIHR Biomedical Research Centre Programme
Commonwealth Postgraduate Scholarship (to Prasad Katulanda)