
Abstract
Introduction. Women suffer disproportionately from depression, which has a high prevalence in developing countries. Sociodemographic factors are associated with depression, some of which may be modifiable and lead to better outcomes for depression among women. Objectives. To determine sociodemographic factors associated with depression among women of reproductive age in Karachi. Methods. A case control study was conducted on 376 women in 2 hospitals in Karachi. Patients were diagnosed by psychiatrists and family physicians by Diagnostic and Statistical Manual of Mental Disorders (4th ed.) criteria and SRQ20. Results. The odds for women with depression being married for >5 years, being abused by in-laws, spending ≤3 hours per day with their spouses, and being just satisfied or not satisfied with their married life was more than that for controls. Conclusion. The authors’ findings highlight the important modifiable risk factors for depression, which if addressed will help decrease the burden of depression among women.
Introduction
Depression is a common condition in all parts of the world and is the second most common disorder seen by primary care physicians.1,2 It has been projected that in the next 10 years, depression will be the second most common cause of disability. 3 In developing countries, the prevalence is even higher, and some studies have reported that the prevalence of depression is more than 50%. 4
Depression is twice as common in women as in men. Higher prevalence of depression among women may be attributed to certain biological as well as environmental factors, which have been studied in various parts of the world. Some of the known risk factors for depression among women are a family history of mood disorders, personal past history of mood disorders in the early reproductive years, loss of a parent before the age of 10 years, childhood history of physical or sexual abuse, and use of an oral contraceptive.5,6 Other studies have found risk factors such as marital status, lack of social support, marital dissatisfaction, ethnicity and educational levels, ceasing to cohabit with a partner, widowhood, or being divorced.7-9 In a Nigerian study, factors associated with depression included being single, divorced, separated, living in a polygamous relationship, and a previous history of still birth, 10
A systematic review of studies reveal that the prevalence of depression in Pakistan is 28.8% to 66% for women (overall mean 45.5%) and from 10% to 33% for men (overall mean 21.7%). 1 Studies done in rural Pakistan showed that almost 50% of the women visiting primary care physicians were depressed. High levels of social adversity and low levels of education are also associated with depression in women living in rural areas of Pakistan.11-13 In urban settings, the prevalence of depressive disorders was found to be 44%—26% in men and 58% in women. 5
A systematic review of studies done in Pakistan has shown the association of a number of social factors with depression such as female sex, and middle age and low level of education among women. Loss of husband (being widowed, separated, or divorced), increasing duration of marriage, problems with in-laws, and being a housewife were also positively associated with depression. Women living in joint households with more than 12 members also showed a positive association; in contrast, 1 study reported a positive association for women living in unitary households. 1 Chronic difficulties with housing, finances, and health; absence of a confiding relationship; lack of autonomy; and arguments with husbands and in-laws has also been shown to be associated with depression.1,14
In Karachi, a survey done in a lower-middle-class semiurban community of Karachi, found that the prevalence of depression among housewives was 30%, and most women perceived that financial, interpersonal, and family problems were contributory factors to their ill health. Increasing age, lack of education, and verbal abuse were the associated factors that were found to have an independent relationship with depression. 15 In married women, marital conflicts, bereavement, domestic violence, work stress, daughter’s marriage, and traumatic experiences were found to be associated with depression. 16
Another important factor that undermines women’s physical, reproductive, and mental health and has been shown to be associated with depression is domestic violence. 17 Depression and posttraumatic stress disorder, which have substantial comorbidity, are the most prevalent mental-health sequelae of intimate partner violence.19,20 Women who are abused by their partners suffer more depression, anxiety, and phobias than nonabused women according to studies in Australia, Nicaragua, Pakistan, and the United States. 21 A comprehensive meta-analysis of mainly US studies showed that the risk for depression and posttraumatic stress disorder associated with intimate partner violence was even higher than that resulting from childhood sexual assault. 22
Violence against women is also common in Pakistan as in other parts of the world. A study by Women’s Division on “Battered Housewives in Pakistan” reveals that domestic violence takes place in approximately 80% of households. 23 The Human Rights Commission report states that 400 cases of domestic violence are reported each year, and half of the victims die. 24 A United Nations research study found that 50% of the women in Pakistan are physically battered, and 90% are mentally and verbally abused by their men. 25 Cross-sectional studies have found a higher prevalence of depression among physically, mentally, and verbally abused women.1,14,15 A study in India found that the majority of the women prefer to remain silent despite being victimized because of fear of social isolation. 26
In summary, depression is a common mental disorder, especially among women in developing countries. Studies have indicated that social adversity, lack of education, and the fact that women are underprivileged and are mistreated by their partners and in-laws, leading to marital dissatisfaction, are important determinants of depression in women. A significant proportion of women’s mental health is attributable to sharing of responsibility and common principles in marriage and meeting of emotional and sexual needs. 27 In developing countries, women’s disclosure of psychological and emotional distress is difficult and often stigmatized, which leads to delayed diagnosis and hence increased morbidity by depression.
Rationale
Studies have shown a high prevalence of depression among women in Pakistan, with a few studies indicating more than 50% prevalence in some areas. 13 The high prevalence of noncommunicable diseases such as mental disorders and particularly depressive disorders, which can have devastating economic consequences, is challenging in a developing country like Pakistan because the burden of infectious diseases is still very high. There is a need to develop an evidence base to aid policy development on tackling anxiety and depressive disorders, which are twice as common in women.
Local research highlights important social stressors and sociodemographic risk factors associated with depression in women, but the study designs are variable and there are methodological flaws in the studies. Most of the studies done in Pakistan are descriptive in design, which does not allow one to control for possible confounders and to establish any association. 1 There has been only 1 case control study in Karachi that has shown certain factors to be associated with depression, but the results cannot be generalized as it is confined to the fishing community. 28
Exploring factors and their association with depression is very important in the Pakistani context because of the specific culture where a woman’s disclosure of her social and physical needs is difficult, and often stigmatized. This study intends to identify factors associated with the high burden of depression among women and to indicate measures that may have policy implications for decreasing the burden of disease.
Objectives
We designed an analytical study to determine the association of sociodemographic factors with depression among women of reproductive age at 2 teaching hospitals in Karachi. Our findings highlight the important modifiable risk factors of depression, which if addressed would help decrease the high burden of morbidity from depression among women.
Methods
A case control study was conducted at the psychiatry and family medicine clinics of Aga Khan University Hospital (AKUH) and psychiatry clinics at Liaquat National Hospital from June 2007 till February 2008.
Assuming that the percentage of married women among the reproductive age group is 67% 29 (exposure among controls), with 5% type 1 error, a power of 80%, and an odds ratio (OR) worth detecting of 2.0, the sample size was calculated (at 95% confidence interval [CI]) to be at least 376 with 188 patients and 188 controls. To account for 10% nonresponse in patients and 10% nonresponse in controls, 209 patients and 209 controls were approached (ratio 1:1). 30
Patients comprised all consecutive women, 15 to 49 years of age, attending the clinics mentioned above, not on any antidepressants for the last 2 weeks, diagnosed as suffering from depression by a psychiatrist or family physician according to the Diagnostic and Statistical Manual of Mental disorders (DSM-IV criteria), 6 and currently having a score of 8 or more on the Self-Reporting Questionnaire for Anxiety and Depression (SRQ20). 31 Women who had a history of any other psychiatric illness except depression were excluded.
Controls were selected from among attendants accompanying the patients or any patient visiting the consulting clinics. These were women of reproductive age, who did not have any psychiatric history or current depression according to SRQ20 (score of 7 or less). Controls who on screening had a score of 8 or more were also excluded and referred to a family physician at AKUH for confirming the diagnosis and appropriate management.
The other exclusion criteria for both patients and controls were a history of any chronic illness (diabetes mellitus, hypertension, ischemic heart disease, chronic renal failure, chronic liver disease, rheumatoid arthritis, thyroid disorders, malignancy, chronic obstructive pulmonary disease, and asthma). Those who were on any medication except micronutrients, pregnant/postpartum (up to 4 weeks of delivery), or postmenopausal were also excluded.
Patients diagnosed by the psychiatrist or family physician as having depression according to DSM-IV criteria were reassessed; and the controls were screened for depression by administration of the 20-item SRQ. The sensitivity of the SRQ ranges from 63% to 90% and the specificity from 44% to 95% (tested against in-depth psychiatric interview). 32 The validity of the SRQ has been established in Urdu in the Pakistani population as well. 33 Pretesting was done on 10% of the total sample—that is, 30 participants.
Informed consent was taken from the patients and controls. A verbal consent was taken by the consulting physician from the patients, and if they consented to participate, a written consent was taken by the data collectors. The study was approved by the AKUH Ethical Committee.
Data were collected through self-administered questionnaires in English or Urdu, and if the participants were unable to read or write Urdu or English, the questionnaire was verbally administered by the data collector, and confidentiality was ensured. The completed questionnaires were dropped in closed boxes to maintain their confidentiality.
Data entry was done on EPIDATA 6 and analyzed on Statistical Package for the Social Sciences (SPSS) version 14. Descriptive statistics were computed for categorical variables for patients and controls by computing the frequencies for the 2 groups. Cross-tabulation was run for each categorical variable with outcome variable to look for any zero cell count or sparse data, and based on this, categories of education, ethnicity, occupation, reason for working, and abuse by spouse and in-laws were merged.
For quantitative variables, quartile analysis was done to check linearity of the variable. As none of the variables was significant as quantitative, categories were created by checking the significance of each variable as a quartile or dichotomous variable, and subsequently cell counts were checked for sparse data, and if they were found, variables like working hours, number of family members, number of years married, number of children, and number of hours spent with husband were further merged.
Crude ORs and their 95% CIs were computed through a logistic regression model developed for each independent variable. Risk factors with a P value of <.25 in univariate analysis of factors associated with depression among currently married women were considered for inclusion in the multivariate model to keep the number of participants equal in all variables considered in the multivariable analysis. Confounding status was also checked before removing any variable from the model. The cutoff point for being a confounder was a 15% change in β coefficients. Multicollinearity of independent variables was assessed in the main effect model. Variables with the most significant P values were included in the final model, and other variables were added or removed depending on their significance in the model. The final model was tested for goodness of fit by the Hosmer Lenshow statistic. After checking the goodness of fit, adjusted ORs and 95% CIs were used to interpret the model.
Results
We enrolled 188 women, 15 to 48 years old as patients, including 42 (27.6%) from psychiatry clinics and 60 (39.5%) from family medicine clinics of AKUH and 50 (32.9%) from CHC clinics of AKUH. Equal number of controls were recruited from each clinic. The mean age (SD) of controls was 31.0 (7.1) and of patients was 31.3 (7.5). The descriptive and univariate analysis results are described in Table 1.
Univariate Analysis Showing the Distribution and Association of Sociodemographic Factors With Depression Among Women of Reproductive Age by Their Odds Ratio (OR) and 95% Confidence Interval (95% CI)

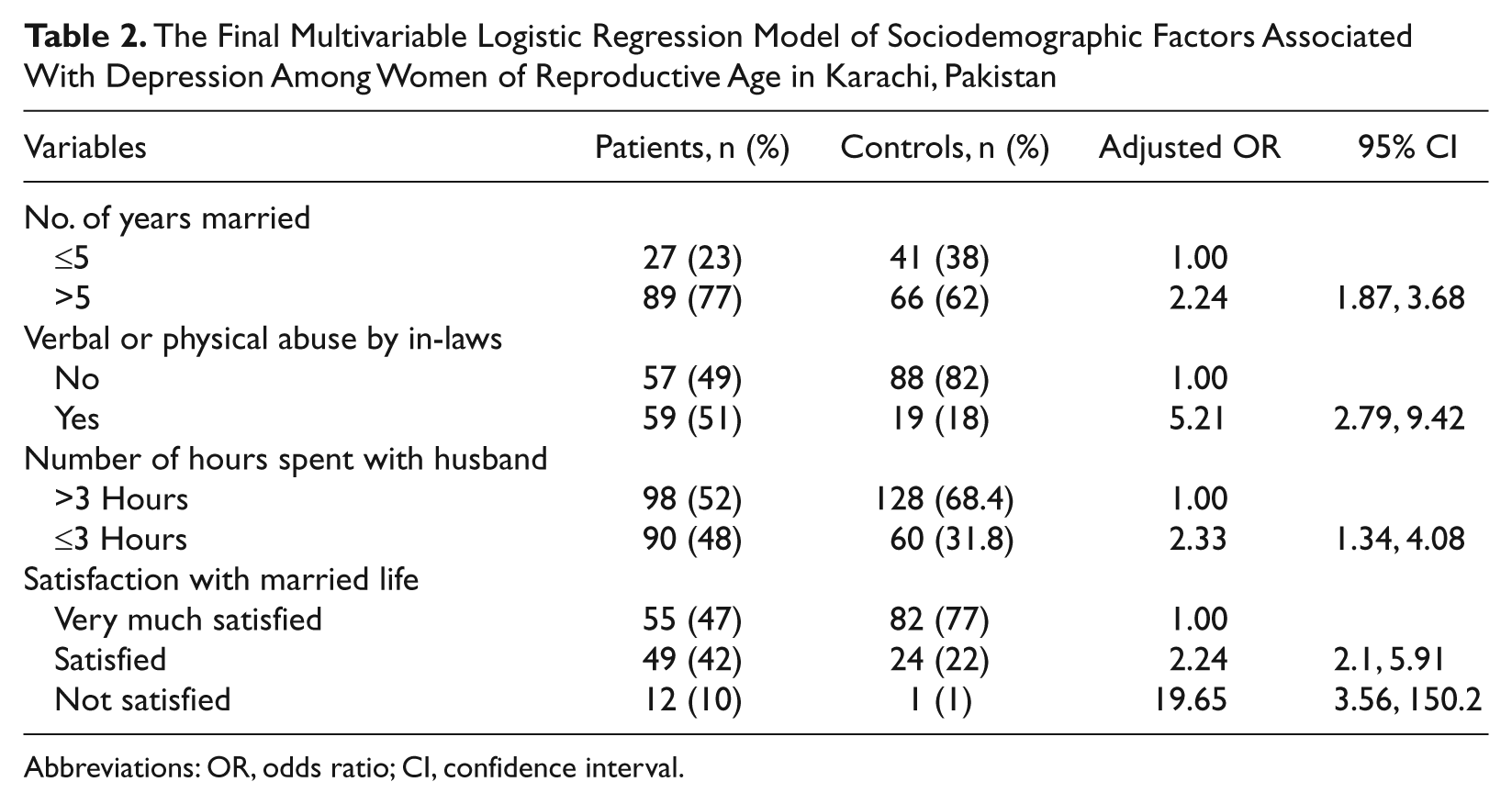
The final logistic regression model included number of years married, physical or verbal abuse by in-laws, number of hours spent with husband, and satisfaction with marital life in currently married women (Table 2). After adjusting for other variables, the odds of patients being married for more than 5 years were more than the odds for controls (OR = 2.24; CI = 1.87, 3.68). Similarly, the odds of patients being physically or verbally abused by in-laws were more than the odds for controls (OR = 5.21; CI = 2.79, 9.42). The odds of patients spending less than or equal to 3 hours per day with their spouses were more than those for controls (OR = 2.33; CI = 1.34, 4.08). Considering very much satisfied as the reference category, the odds of patients who were satisfied (OR = 2.24; CI = 2.1, 5.91) or not satisfied with their married life (OR = 19.65; CI = 3.56, 150.2) were more than the odds for controls.
The Final Multivariable Logistic Regression Model of Sociodemographic Factors Associated With Depression Among Women of Reproductive Age in Karachi, Pakistan
Abbreviations: OR, odds ratio; CI, confidence interval.
There was no interaction found in the model. The Hosmer Lenshow test for the final model was (χ2 = 7.72; P = .45).
Discussion
Our study found that number of years married, abuse by in-laws, less than or equal to 3 hours per day spent with husband, and not being very much satisfied with marital life were associated with depression among currently married women of reproductive age. All these findings show that if a woman does not share a good relationship with her spouse and in-laws, it could reflect on her mental health.
Some of these positive associations were consistent with those found in other studies, such as increased duration of marriage 1 and poor relations with in-laws15,34; other associations have never been studied in the past in Pakistan.
Dissatisfaction with married life was found to be associated with depression and it showed trends. Longer years of marriage was also found to have a positive association with depression in our study. Some studies in the past have shown that being single, divorced, separated, and living in a polygamous relationship is associated with depression, but in our study, in the univariate analysis, being married was significantly associated with depression (taking a P value of .25 as significant). This is consistent with a study in Malaysian women, which has also shown correlation of depressive symptoms with marital dissatisfaction scores. 9 This could be because of the feeling of helplessness that arises from living with an imposed partner for a lifetime, which is a usual feature in our part of the world because of cultural and social inhibitions that do not allow women to marry by choice. A study done in South Africa, which is a developing country like ours, showed that 95% of married women had relationship problems, 34 which again explains the higher number of married women with depression. Another reason, as another study reveals, is that married women faced lesser distress than single women, but this distress increased in divorced women compared with women who lived in continuous marriage. Also, it has been reported that marital dissolution affects men more than women.35,36 Therefore, a long-lasting marital relationship that is unsatisfactory is a risk for depression among women.
Another factor that was found to have a positive association with depression among currently married women in this study was less number of hours spent with the husband. This finding is also important and may be related to younger age at marriage because other studies have shown that women who are married at a younger age tend to have spouses who are much older than them, which may intensify the communication gap and power imbalance between spouses. 37 Another reason could be that because of economic hardships and a joint family system, which prevails in our part of the world, male partners may be unable to give quality time to their wives, hence the lower level of moral support, which results in a poor marital relationship and, subsequently, depression.
No previous studies were found on association of number of hours spent with spouses and depression, but a study has shown that the prevalence of domestic violence among women in association with depression15,38 was less among couples who communicated and made joint decisions. 39 This means that a good relationship between couples leads to a lesser incidence of domestic violence, which may lead to a lower incidence of depression among women.
Taken together, hours spent with husband and marital satisfaction and number of years married, it can be inferred that a good relationship between husband and wife is associated with lower levels of depression among women, whereas a poor marital relationship that persists aggravates the distress and depression in women. Because the prevalence of depression among Pakistani women is high, efforts should be made at the community level to enhance communication between partners.
Another factor found to be associated with depression among currently married women was abuse by in-laws, which includes abuse by the mother-in-law, father-in-law, and sister-in-law. This has already been studied in the past.15,40 The joint family system is common in Pakistan, and therefore, women here are more prone to physical, verbal, and emotional abuse by in-laws than in other countries where nuclear families are more common and accepted culturally. Violence, abuse, and relationship problems are a significant cause of depression among women, and hence, this finding is consistent with that from other studies. Increased number of family members living in a household was not found to be associated with depression in the multivariable analysis, which reflects the fact that living in a joint family itself may not be a risk factor for depression; in fact, for a married woman, living with supportive in-laws may decrease the burden of responsibilities and thus mental stress. This may have an opposite effect with an abusive family.
Other factors such as ethnicity, less education, number of family members in the household, monthly income, abuse by spouse, and number of children were also associated with depression in the univariate analysis, but they were not considered in the multivariable analysis because of the discrepancy in the number of participants between different variables. Some of these associations are consistent with those found in other studies, such as less education,1,15,41 socioeconomic adversity, verbal abuse, and relationship problems.1,4 Among married women, marital conflicts, domestic violence,19,38,40-43 increasing duration of marriage, and multiparity 1 have been shown to be associated with depression. It is a possibility that as patients and controls were selected from the same clinics, it may have resulted in the dilution of certain sociodemographic factors. Responses may have been similar for spousal abuse and marital satisfaction; moreover abuse by in-laws may also be associated with spousal abuse, and therefore, association of spousal abuse was not found in the multivariable analysis, although initially no multicollinearity was found between independent variables.
Finally, 19% of the potential controls were screened to be positive for depression by the DSM-IV criteria, which is a high number. This reflects the fact that women in our population do not even know that they are suffering from a mental illness, and therefore, they delay seeking medical care, which leads to an increase in morbidity associated with this disease. This means that there is an urgent need to develop programs for screening of women for depression in the community and to train and create awareness among physicians to routinely screen for depression in the primary care setting.
In conclusion, we found that increased number of years, physical or verbal abuse by in-laws, less number of hours spent with the husband, and dissatisfaction with marital life are associated with depression among currently married women of reproductive age in Pakistan. These associations may be a result of the fact that women are suppressed and abused in our society, and as a result of the nonconfiding relationship with the husband, nonrecognition of a wife’s needs by husbands, and pressure from in-laws, married women suffer disproportionately from depression.
Strengths and Limitations
This is the first analytical study of its kind in the patriarchal Pakistani society where women’s autonomy is limited. This study has identified associations between some sociodemographic factors and marital abuse among women in the Pakistani setting, where the cultural context of women’s marital rights is different from that in most of the world. This has never been studied in Pakistan.
There are certain limitations that are inherent in a case control design. It is difficult to establish a temporal relationship, which means that we cannot be sure whether depression was actually preceded by the associated factors. Even if the patients were diagnosed with depression for the first time in the clinics, we can never be sure when depression had actually started because the severity and persistence of symptoms may have made them seek care at that point in time. For such a chronic disease like depression, a cohort study may not have been a better option because a large sample size would be required and loss to follow-up would be a problem. Second, it would not have been ethically appropriate to follow such women for development of depression without trying to help and counsel them. A case control study is also a better choice for a disease like depression with multiple etiologies and risk factors. A matched case control study controls for confounders as well, but the objective of this study was to determine the sociodemographic factors associated with depression; therefore, it was not possible to match the patients and controls on their age or sociodemographic factors. This could be a limitation, but we checked for the confounders in the analysis by logistic regression.
There is always a possibility of imperfect recall in such studies, but it is not very likely because all the questions asked reflected the current social and reproductive status of the participants. The possibility of interviewer bias was eliminated by pretraining of the research officers and keeping the questionnaire self-administered except in participants who requested assistance from the research officer. Still there are chances that participants may not have revealed the true details—for example, the frequency of abuse may actually be more than what was reported.
In all, 100% of the participants answered all the questions, which was well above our expectations because we thought that women may not want to disclose their marital issues in our cultural setting. The participation rate was also good (97%). Among women who refused to participate, 10 excused themselves because of nonavailability of time, and 3 said that they would not like to disclose personal information.
In this study, depression in patients was diagnosed by DSM-IV criteria by the physicians or through the psychiatrist interview, which is the gold standard for diagnosis of depression; through this we tried to avoid misclassification of patients. As the physicians were asked before the study if they use the DSM-IV criteria to diagnose depression and 100% of them gave a positive answer, we were unlikely to misclassify a patient as a control, although there is a very small probability of classifying a control as a patient.
The patients and controls were selected from hospitals, which might have induced a selection bias. The controls were selected from the same clinics, and 20% of the controls were actually attendants accompanying a patient, which might have lead to matching of some sociodemographic factors among the patients and controls, consequently leading to dilution of some associations, especially about ethnic origin and monthly income—hence the inability to find significant associations.
Our study participants may not be representative of the general population because these were women who attended a tertiary care hospital, and therefore, there is the possibility that they had different characteristics from the general population.
The tools used to measure verbal and physical abuse consisted of 3 items each to measure frequency of abuse, which were not validated, although the questions asked for measuring abuse have been used in the WHO multicountry study. 44 The reason for not using validated tools was that no tools for measuring abuse have been validated in Pakistan, and validating tools was not in the scope of this study. This could have led to imprecise measurement of some outcome variables and gives scope for further, more comprehensive studies.
Conclusion and Recommendations
Our study indicates that among married women of reproductive age there are certain risk factors for depression, including increasing years of marriage, domestic violence by in-laws, less time spent with the spouse, and not being satisfied with married life. Primary care physicians should be trained to identify depression and provide appropriate guidance and counseling to women at risk and their families about the predisposing factors for depression. Early recognition of marital dissatisfaction, poor relation with in-laws, and domestic violence is also important to promote better mental health outcome through marital counseling of couples if required.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.