
Abstract
Background and context. Uncontrolled and exponentially increasing population is one of the biggest obstacles in the socioeconomic progress and prosperity of a nation. Aims and objectives. The present study was undertaken to evaluate contraceptive practices among eligible couples living in the rural areas of Punjab and their perception, knowledge, attitude, and behavior toward various family planning methods. Materials and methods. A cross-sectional descriptive study was done by the interview method to evaluate the various individual determinants toward contraceptive practices among 1123 married women and their husbands aged between 15 and 49 years. Eligible couples (5477) from in and around the hospital were registered at the rural health center of our institute. Statistical analysis was carried out using nonparametric tests such as percentand χ2 test. Results. Contraceptive prevalence was found to be 78.1% and the most commonly used method was surgical sterilization (42.3%). Among the spacing methods, condoms, oral contraceptive pills, and intrauterine contraceptive devices (Cu-T) were used by 36.4%, 7.4%, and 5.5% of the couples, respectively while traditional methods were preferred by 8.3% of the women. Weakness, menstrual dis infertility, weight gain, etc were few of the side effects that were perceived by women as the main hurdle in the use of contraceptives. Irrespective of the method of contraception used, 33.3% of the women reported unwanted pregnancy, most commonly among the users of condoms (79.1%). Sixpercent of the women were not satisfied with the gender composition of their family and desired a male child. Conclusions. Increased use of modern contraceptives requires community-wide and multifaceted interventions that aim at countering negative perceptions about modern methods.
Keywords
Introduction
India is harboring approximately 16.0% of the world’s total population, even though occupying only 2.4% of world’s territorial area. India is thus the second most populous country in the world, next only to China. 1 The past decade has seen a rise in India’s population growth by 21.3%, which means an addition of another 180 million people to the population. The cumulative momentum in population growth in India can be attributed mainly to a higher percentage of women (45.0%) in the reproductive age group (15-45 years) and majority of them getting married at an early age. 2 In the past decade, the health policy of the nation has laid stress on achieving the Millennium Development Goals with special emphasis on improving reproductive health by improving maternal care, reducing the infant mortality, and eradication of the extreme poverty among Indian masses.3,4 It is estimated that 90% of abortion-related mortality and morbidity, 20.0% of pregnancy-related complications, and 32.0% of maternal deaths in India could have been prevented by the effective use of contraception. 3
India, along with China, is a way ahead in population dynamics and statistics in spite of being a pioneer in the launching of the first family planning program, which has now been renamed as reproductive and child health. Currently, married women in India are having easy access to various new, safe, effective, and affordable methods of family planning, which enables them to safely plan their pregnancy and childbirth. The contraceptive services are freely available in all the government health centers throughout the country under various health schemes. But in spite of the provisions of numerous family planning methods, there is hardly any significant increase in the number of eligible couples adopting these methods as per the population census. Women in India, although desirous to space childbirth and limit their family size, do not adopt correctly or partially adopt the various family planning practices, which leads to the vicious cycle of unintended pregnancies, septic abortions, and increased maternal mortality or morbidity. This is one of the biggest challenges faced by the Indian government in tackling the problem of population explosion. 3
The lack of awareness, illiteracy, and poverty along with numerous other factors and reasons are responsible for the irregular and improper use of these family planning practices. The majority of the population in India is from an agricultural background and resides in rural areas. All the above-mentioned factors along with certain myths, faith, superstitions, and sociocultural factors shared by this large Indian community are responsible for the ever-rising population growth of the country. The majority of the contraceptive users often attribute reproductive tract infection of any type or even a common health problem to the method used for family planning. The factors that further contribute to this problem include the absence of complete pre-acceptance counseling, including information on potential side-effects and lower complications, as well as lack of postacceptance follow-up results after the discontinuation of a particular method. 5 Until and unless the current level of deficiencies and weaknesses are properly identified and suitable measures are adopted to rectify and strengthen them, no yojna or scheme can stabilize the growing rate of population to a satisfying extent.
Keeping in mind the various considerations and practices related to contraceptive use, we planned to conduct a study and work at this level to evaluate the knowledge, attitude, and behavior of women regarding the adoption of family planning methods. We believe and hope that this information and analysis could be of immense benefit to family planning programs. The format and the methodology adopted in this study may also help in strengthening the contraception and family planning practices in other developing countries in general and India in particular, thereby assisting in redesigning policies to tackle the problem of population explosion.
Materials and Method
The present study was conducted among married women in the age group of 15 to 49 years whose families were registered at the field practice area of the Rural Health Training Center attached to the Department of Community Medicine of our institute, during the period of March 2009 to October 2009. Every registered family was thoroughly covered for the study, and a simple random sampling method was chosen for selecting eligible couples for the purpose of the study out of the total 5477 registered couples. The sample size of 1123 eligible couples was selected with a confidence level of 95% and confidence interval of 2.61. Criteria for eligible couple comprised 2 individuals who are legally married under the laws of the state where they have a permanent home, living together in the same household, and holding themselves as husband and wife to the community in which they live. Most of the couples belonged to Sikh (52%) and Hindu religions (44%), whereas Muslims, Christians, and other religions accounted for the rest. Women who were widows, infertile, divorcees, and postmenopausal were excluded from the study. Similarly, couples wherein the male had a history of azoospermia or were not fully cooperative were excluded from the study.
A pretested questionnaire was designed in such a manner so as to get quantitative information keeping the prime objectives of the project in mind. A convenient time for the face-to-face interview was fixed with the participants as per their convenience and a semistructured interview was conducted at the respondents’ houses in their own vernacular. The objectives and the reasons for the study were explained, and written consent was obtained after assuring them of their privacy and a promise to keep the information confidential. As the decision for adoption of contraception by the couples is a mutual one, the initial approach was to make them sit together and gather as much information as possible. Later on the husbands were requested to leave the room on the pretext that some problems regarding menstrual cycle were to be discussed. This was done deliberately as in a male-dominated society females do not completely feel the freedom of expression and are quite uncomfortable and reluctant to express their thoughts and opinions especially in the presence of their husbands. This approach worked very well in all the cases as the husband also got good attention in the beginning and readily obliged for the wife’s interview later on.
The rationale behind the adoption of the interview method was mainly to eliminate any subjective error owing to the prevalence of low literacy rate, clearing any doubts then and there, to elicit a complete response, and to bring uniformity in the pattern of the survey. During the interview, respondents were asked about their age, occupation, menstrual history, obstetrical history, number and gender of kids, any history of abortion and its cause, methods of spacing the pregnancies, reasons for not using any contraceptives, awareness about various methods to avoid pregnancies, and the reasons for preferring a particular contraceptive method. These respondents were also asked about any variation in their menstrual cycle before or after the use of these contraceptive methods. Particular attention was paid to condom users in asking about the daily and regular routine use of condoms as a contraceptive practice. The data thus collected from the participants included the age, type of family, family income, number of years of marital life, number of children including “unwanted” pregnancy if any during their married life, menstrual disturbances, perception about the various family planning methods, source of knowledge about the contraception services, the method(s) adopted, and the reason(s) for adopting a particular method and rejecting others. A detailed menstrual history was elicited from the contraceptive users to know the prevalence of menstrual morbidity. The following clinical presentations were reported:
Menorrhagia: Prolonged duration of more than 5 days with excessive but regular bleeding Dysmenorrhoea: Painful menstruation, both congestive and spasmodic types included Polymenorrhoea: Frequent menstrual periods with less than 21 days duration, either excessive or not Metrorrhagia: Irregular bleeding that may or may not be prolonged in duration but normal in amount
The data thus collected were analyzed by using nonparametric tests such as percentages and χ2 test.
Results
The total number of ever-married women in the age group of 15 to 49 years was 1123 (20.5% of the total population), and the proportion of married women was highest (20.6%) in the age group of 30 to 34 years.
Demographic Profile of the Contraceptive Practices Adopted by the Female Participants
Table 1 shows that out of the 1123 women interviewed, 78.1% were “ever users” of any contraceptive method at the time of the study. The most commonly used method was the terminal method or surgical sterilization (42.2%). Condoms, oral contraceptive pills (OCPs), and intrauterine contraceptive devices (IUCDs) were used by 36.4%, 7.4%, and 5.5% of the couples, respectively, among the available spacing methods. Traditional methods (eg, abstinence, coitus interruptus, breast feeding, and rhythm method) were adopted by 8.3%. Contraception was practiced maximum by the women in the 35 to 39 years age group (22.8%). The difference in relation to the preference of use of spacing and permanent methods of contraception among women of younger age groups (15-34 years) when compared with older age groups (35-49 years) was found to be highly significant statistically (P < .001).
Age Distribution of Ever-Married Women (15-49 Years) According to Contraceptive Practices
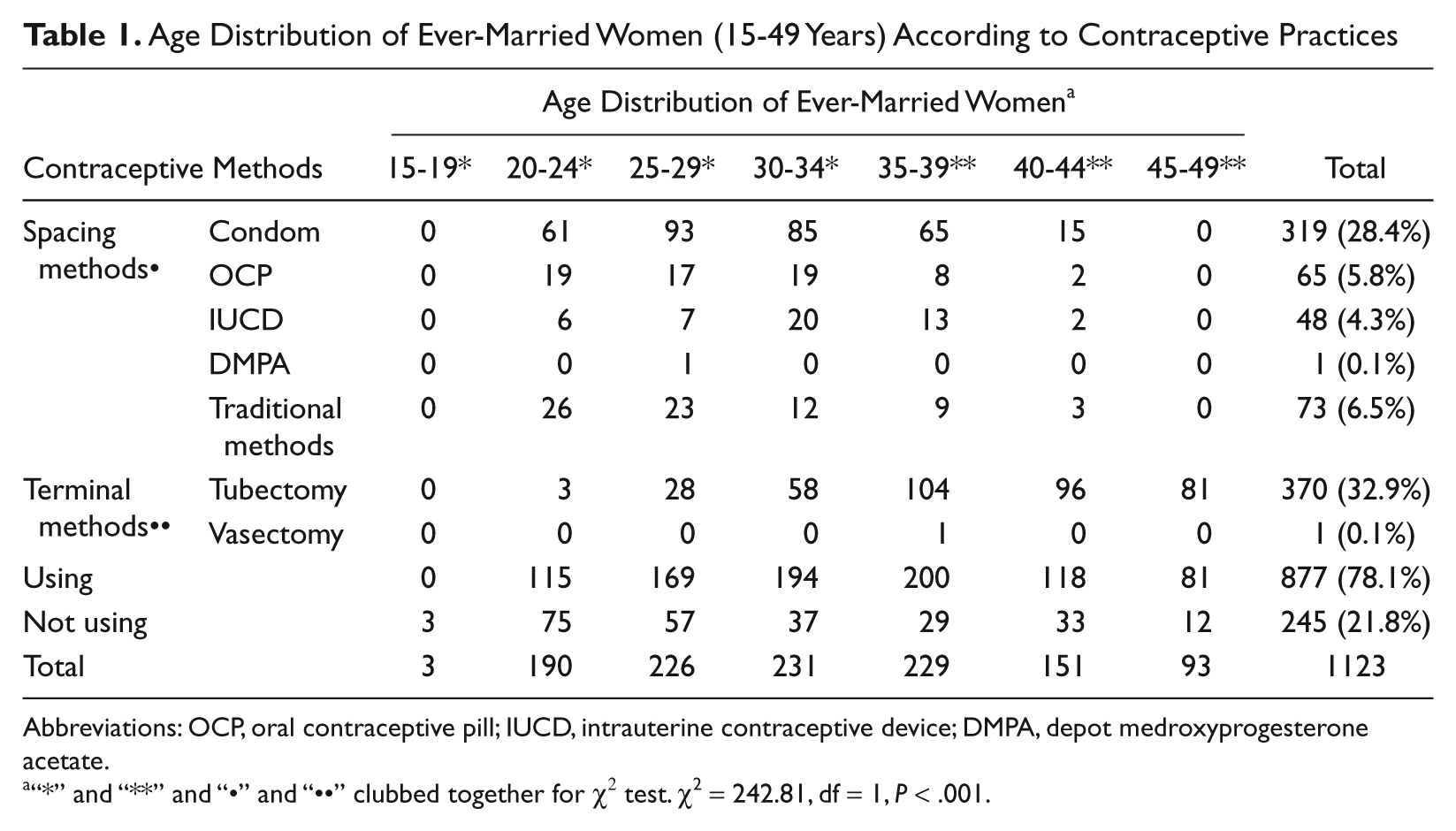
Abbreviations: OCP, oral contraceptive pill; IUCD, intrauterine contraceptive device; DMPA, depot medroxyprogesterone acetate.
“*” and “**” and “•” and “••” clubbed together for χ2 test. χ2 = 242.81, df = 1, P < .001.
Myths and Beliefs Inhibiting the Use of Contraceptives
Table 2 shows that the awareness in eligible couples about the availability and use of different contraceptives was more than 90.0%, except in cases of DMPA (depot medroxyprogesterone acetate; 11.1%). All of them had knowledge about the various family planning methods, although the absolute correct use and merits of these methods was not known to all of them in entirety.
The onset of physical weakness with the use of these contraceptive methods was commonly perceived by almost all contraceptive users as the prevalence of 72.4% in the case of OCPs, 59.3% in IUCDs, 59.7% in tubectomy, and 13.9% in the case of condom use highlighted this perception. Exacerbation of menstrual problems was an another common belief and perception in relation to the use of various contraceptives, as 74.3%, 67.7%, 30.6%, and 26.0% of the study population using DMPA, IUCDs, OCPS, and tubectomy, respectively, reported this menace. Contraceptive use leading to infertility was perceived by 30.1% of women who used OCPs, 28.3% who used DMPA, and 26.8% of women using IUCDs.
Perception of Women Toward Various Contraceptive Methods Inhibiting Their Use (Multiple Responses)
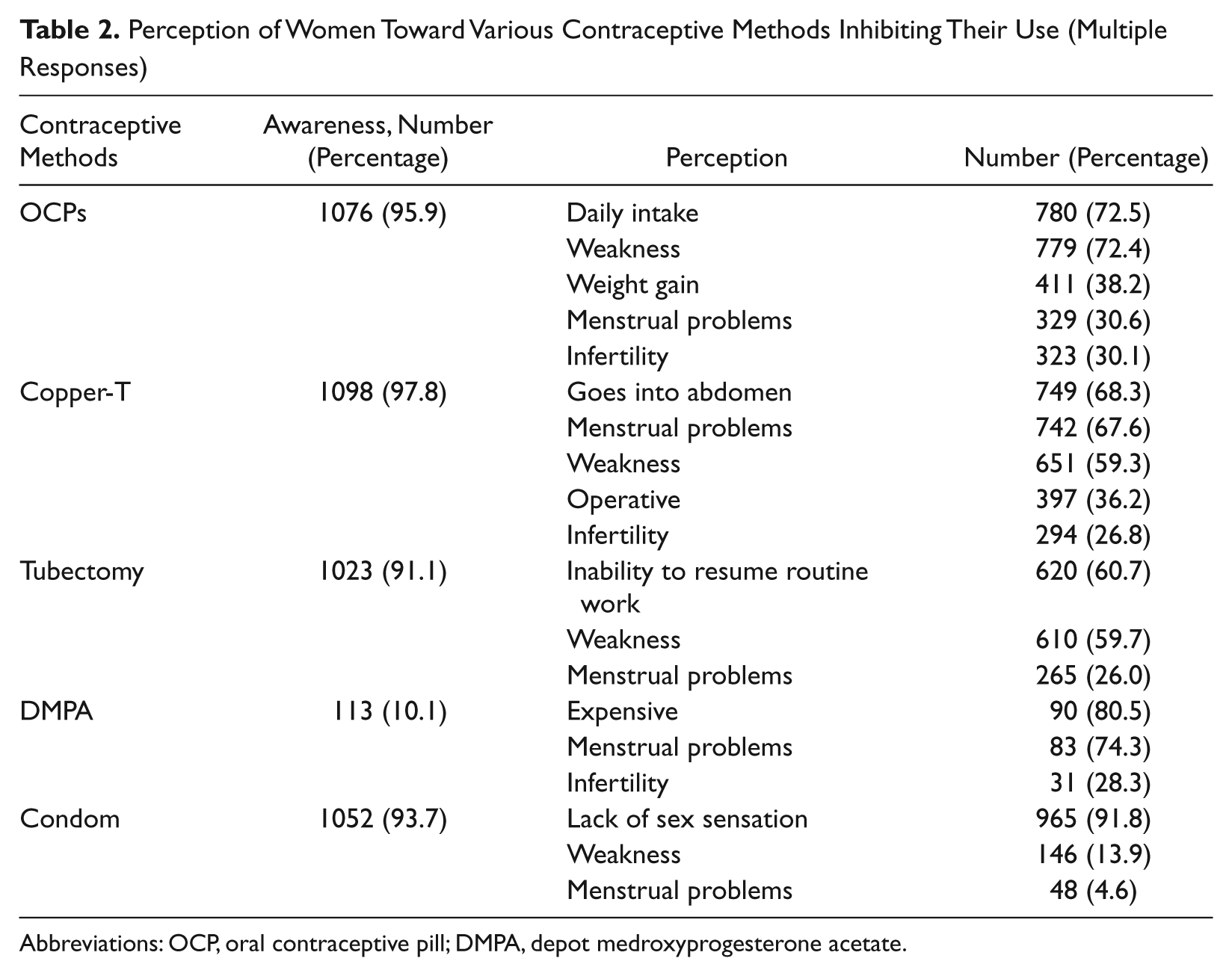
Abbreviations: OCP, oral contraceptive pill; DMPA, depot medroxyprogesterone acetate.
The problem of weight gain and reluctance to daily intake of 1 pill was reported by 38.2% and 72.5% of contraceptive users, respectively, in reference to OCPs.
“Cu-T going into abdomen” was believed and commented by 68.3% of the women, who were aware of this method although none of the subjects in our study group had complication of perforated uterus due to Cu-T. The various operative problems related to the use of IUCDs were other perceptions among 36.2% of the women using them.
Among the women who were aware of DMPA as a contraceptive method, 80.5% had reported that it was quite expensive to use.
Among ever-married women whose husbands were using condoms as a contraceptive method, 91.8% reported and complained of lack of adequate and proper sexual sensation with the use of condoms. This lack of sexual sensation was the chief complaint of the husbands to their respective wives.
Among the menstrual disturbances reported by women, irregular bleeding was indicated by 3.1% of the OCPs users. Dysmenorrhoea (27.1%), menorrhagia (22.9%), and polymenorrhoea (12.5%) were the other common discomforts reported by the IUCDs users. Among women who had undergone tubectomy, 6.8% complained of dysmenorrhoea, 6.0% menorrhagia, and 4.3% polymenorrhoea.
Unwanted Pregnancy With the Use of Contraceptive Methods
Table 3 shows that a total of 33.3% of the women using any of the available methods of contraception reported “unwanted pregnancy” during their married life. The unwanted pregnancy was reported most commonly among the users of condoms (79.1%) and with traditional methods of contraception (48.0%). The incidence with the use of other methods was reported to a lesser extent (3.1% with OCPs and 0.5% with tubectomy). The difference in the incidence of unwanted pregnancies related to the use of various methods of contraception was found to be highly significant statistically (P < .001).
Distribution of Ever-Married Women With Unwanted Pregnancy According to Their Use of Contraceptive Methods a
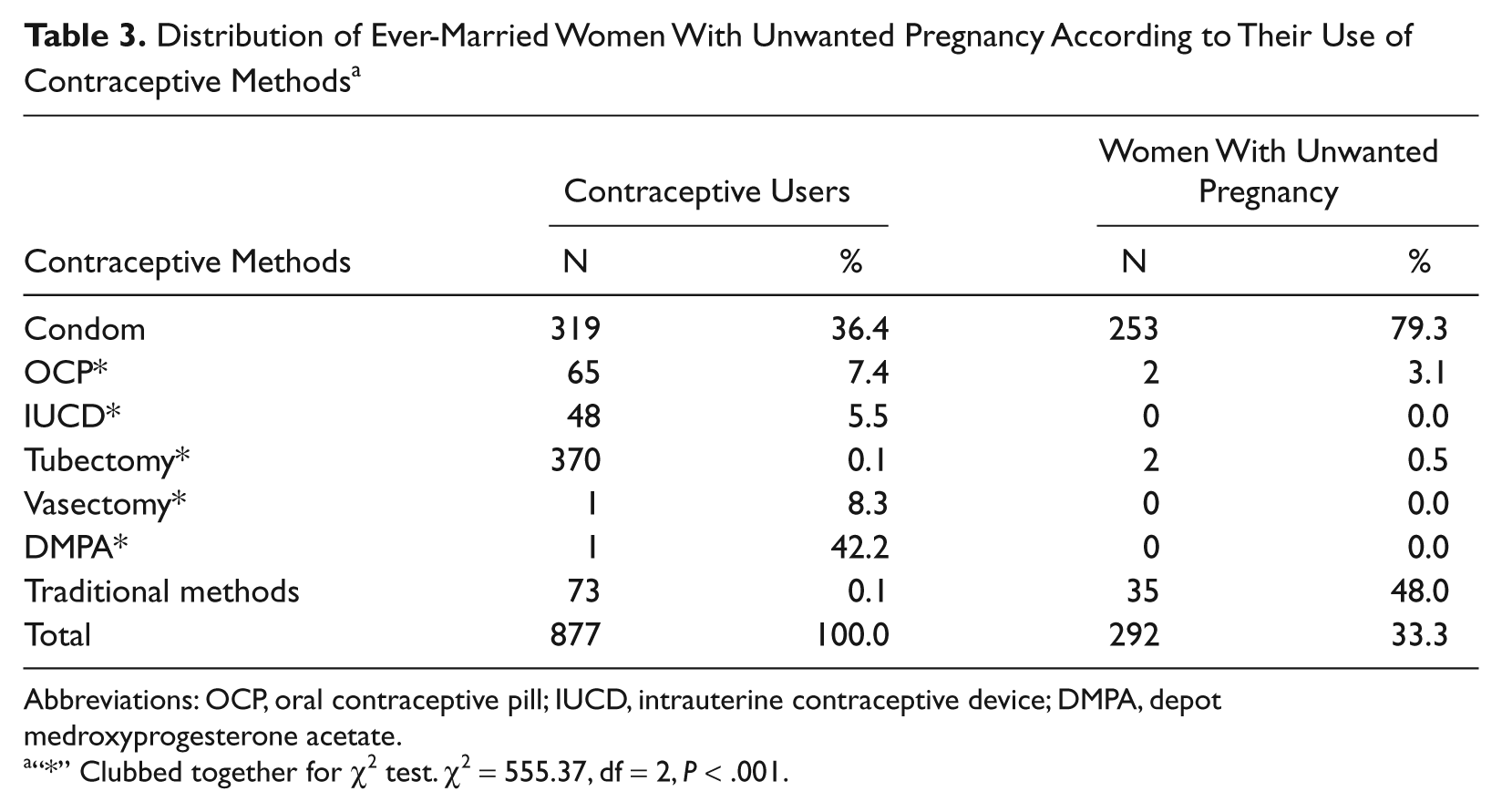
Abbreviations: OCP, oral contraceptive pill; IUCD, intrauterine contraceptive device; DMPA, depot medroxyprogesterone acetate.
“*” Clubbed together for χ2 test. χ2 = 555.37, df = 2, P < .001.
Reasons for Reluctance to Use Family Planning Methods
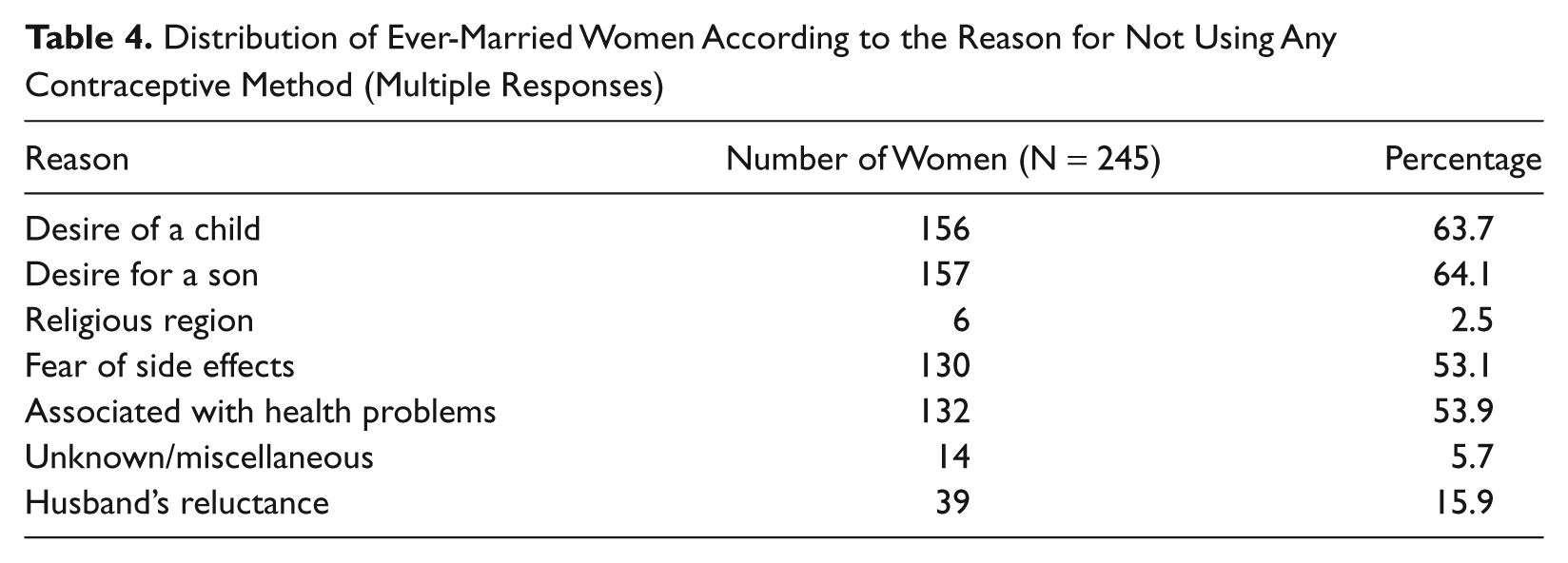
Table 4 shows that among the women who were not using any contraception, maximum number of them (63.7%) desired for a child and majority of them desired a son (64.1%). The common health problems associated with the use of these contraceptive was cited a reason by 53.9% of the women, whereas 53.1% of the women reported the fear of side effects as a reason for not using these contraceptive methods. The refusal by the husbands to use a condom as a contraceptive was reported by 15.9% of the women.
Distribution of Ever-Married Women According to the Reason for Not Using Any Contraceptive Method (Multiple Responses)
Discussion
Although there is regional, religion, and caste diversity in the population of the entire rural India, the sociocultural, behavioral, economic, and educational parameters of these communities do reflect quite a similar pattern and in fact a unity in diversity. It was difficult to encompass the entire nation for conducting the present study, but we can consider the concerned population as somewhat a true representative of the entire country though minor variations and limitations may still exist. The recruitment of 1123 eligible couples represented 20.5% of the registered couples from a total of approximately 0.125 to 0.15 million population. The incidence of the contraceptive prevalence rate in the present study was found to be 78.1%, and surgical sterilization is the most commonly used method by the population (33.0%) in the present study, which is quite similar to the survey reports of NFHS-3 (National Family Health Survey) in India (38.3%) as well as DLHS-3 (District Level Health Survey) in Punjab (33.2%).6,7 The similarities in our study and those of the state and national levels again reaffirm the fact that our study sample is almost a true representative of the entire nation. More important, be it African or Asian countries, contraception and family planning statistics in developing nations depicts a similar scenario.8-10
The majority of the female population in our study in fact was very much aware of the concept of spacing as well as the permanent methods of contraception, which does project a picture of similarity with the findings of other researchers. 11 The credit of success for the present scenario in our country regarding the level of awareness about the contraceptive practices among the general public goes to the continuous and dedicated efforts of our government and its health policies, mass media, and our hard-working health and social workers who are the main contributors followed by some efforts from public relations and magazines.
The maximum users of spacing methods were the women in the 20 to 34 years age group, in whom condoms (27.3%) were the most frequently practiced spacing method, followed by the traditional methods (7.0%), when compared with the women in other age groups. The older women preferred to adopt the terminal method for contraception and the reasons for this finding were quite obvious. As the women get older, most of them would have completed their families and hence were in favor of using terminal method compared to the spacing methods. The most successful contraceptive methods with least failure rates, that is, OCPs, Cu-T, and DMPA, were not popular among our study population (7.4%, 5.5%, and 0.1%, respectively). Similar demographic findings and its related contraceptive practices were observed by the other researchers as well.12,13
In addition to various factors such as religion, type of family, household income, number of living children, and mother’s level of education, there was another important factor that restricted the use of modern contraceptives. It was the perception of people about the numerous side effects associated with the use of such services. In many countries, concern about the side effects associated with the use of contraceptives, which originates from the experiences of friends and the various rumors told and retold through the communities, has contributed to a lower contraceptive acceptance. This affects the pattern of contraceptive use especially in a semiliterate country such as India. 14
Generalized weakness (72.4%), menstrual problems (30.6%), and other side effects along with a reluctance in daily intake of the pill (72.5%) were the main reasons cited for not using OCPs. Fear of perforation of womb (68.3%), menstrual problems (67.6%), and myth of possible operative procedure (36.2%) made Cu-T unfavorable among women in our study group. Awareness about DMPA was very low (10.1%), but even people who were quite familiar with its use were also reluctant to adopt it due to its cost factor (80.5%) and the associated menstrual problems (74.3%). Although tubectomy was preferred by the women in our study group as a method of contraception, many of the women who refused to adopt it as a family planning method cited the perception that it causes weakness (59.7%) and inability to resume daily routine chores (60.7%). The perception about similar contraceptive practices and their related side effects were reported in the findings of other such similar conducted in Delhi. 15 Misconceptions, rumors, and myths about the contraceptive practices are the main hurdles to discourage the use of modern contraceptive methods as has also been reported by various other studies. 16
A particularly important challenge for the health service providers and the delivery system itself is the side-effects associated with the use of various contraceptives. Health care providers often dismiss the women’s concerns about the various side effects with a disparaging remark such as “Its all psychological or imagined.” Women treated in this manner are less likely to get encouraged to be compliant, satisfied, or become effective users of contraception irrespective of their educational and income levels, which leads to an increased risk of unwanted pregnancy. The health care providers need to have thorough knowledge about the consequences of the various side effects from contraceptive use for women and must be trained and encouraged to treat women’s concerns with respect, dignity, and honesty.
Each and every woman is always aware of and concerned for her periods especially during the marital life as she desires a regular and adequate bleeding pattern. In addition to weakness, menstrual problem was the other main perceived side effect associated with the adoption of the contraceptive services. Therefore, we interviewed all the women who were using the various methods of contraception in the background of these aspects and misconceptions. Among OCP users, no menstrual problem was observed except in 2 women in whom the missed pill was the main reason for irregular bleeding. In fact, OCPs are the prescribed treatment of choice worldwide for various menstrual problems. 17 Menorrhagia, dysmenorrhoea, and polymenorrhoea were observed in some tubectomized women (4.3%, 6.8%, and 6.0%, respectively) as well as in women who were using Cu-T (22.9%, 27.1%, and 12.5%, respectively), which was similar with findings of other such studies. 18 On elicitation of the respective history, most of the women stated that they bled slightly more than the previous menses and that dysmenorrhoea was spasmodic, which can be ascribed as physiological, whereas in other women it was associated with polymenorrhoea. IUCDs sometimes do cause menstrual troubles and that too in the initial period after insertion, which may be due to biological changes in the uterine cavity. 19 Cu-T insertion by ill-trained or partially trained staff has often caused problems, which could have been avoided had the health professionals been adequately trained and by the application of some stringent measures and legislations. In tubectomized patients, menstrual disturbances can be explained on the basis of possible postligation syndrome in which blood vessels adjacent to mesosalpinx can get damaged during the procedure. 19 Even this complication demands strong need for adequate surgical training.
Among nonusers of contraceptives, in addition to the spouse opposition (15.9%), fear of side effects (53.1%) and health problems (53.9%) were the other main reasons for avoiding contraception. Furthermore, a few of the nonusers of contraceptives strongly cited the desire for another child (63.7%), and among them majority had a desire of a son (64.1%). Similar sociocultural and psychological constructs were reported by other observers among the nonusers of contraceptive services. 15 In our study group, a large proportion of nonusers comprised women (63.7%) who were married for just 1 or 2 years and were planning to conceive at that stage, whereas the rest (64.1%) were not satisfied with the gender composition of their offspring, which led them to continue their reproductive activities. The gender preference in the Indian sociocultural setup as well as the desire to have another child are important factors that act as barrier to the use of contraceptives.20,21
To our surprise, in spite of the high prevalence of the use of contraceptive practices (78.1%), unwanted pregnancy was still quite high (33.3%) in our study group though a greater proportion of the participants adopted condoms (79.3%) or traditional methods (48.0%) as means of contraception. Other researches have also arrived at almost similar conclusions, which relates to the failure of condoms and traditional methods in preventing unwanted pregnancies.22,23
On descriptive analysis of such failures and a little higher incidence of unwanted pregnancy, we found the false perceptions of people about use of contraceptives, such as “there is no need to use condom daily, it is needed during the days of menstrual flow during which pregnancy occurs” and “until I will breast feed there is no chance of pregnancy.” Keeping the beliefs and myths about these practices in their mind, they continue to breast-feed their baby for 3 to 4 years and sometimes even more. This entire exercise has revealed that the women received very little information from health providers regarding the efficacy or appropriate use of contraceptives. The findings of the present study have highlighted facts that call for the urgent need to include both the genders in reproductive health interventions, particularly in relation to the use of condoms. Therefore, we have observed that one of the major reasons for unwanted pregnancies is the lower level of awareness about the shortcomings of contraceptives and family planning delivery systems.
Millions of women from developing nations who want to limit or space childbirth do not use modern contraceptives because of the unknown fears of the technology. They are restrained by the partners, family, or the community, or they lack proper information as observed in this study. Therefore, it is the social and moral duty of the government and health care personnel to provide comprehensive information on the use of various contraceptive methods. This does not mean simply conveying the list of the various contraceptive methods available but also includes providing information on possible side effects, contraindications, and modes of use. When the women are fully informed about the options available, only then will they be able to take their own decisions about choosing a method of contraception that they feel most safe and comfortable with and thus can use it effectively.
Conclusions
Our study has concluded and reaffirmed the fact that in modern India women want to space childbirth but most of them rely on the traditional methods and condoms rather than the adoption of other modern contraceptives due to their preformed misconceptions about them. The increased use of modern contraceptive practices requires community-wide and multifaceted interventions, which should be directed to diminish, if not eliminate, the negative perceptions associated with the use of these modern methods. Family planning and health programs should ensure provision of empathetic counseling for contraceptive choices and offer comprehensive services to meet the multiple reproductive health needs of Indian women.
Similar studies can be carried out in other developing countries where an uneven growth of the population is a hindrance to the overall socioeconomic development. Even in India, similar methodologies can be adopted while simultaneously analyzing the other population-related problems in the society. The rural health infrastructure should be strengthened in a manner similar to that in our institute, wherein we covered more than 75 to 80 villages as well as 0.28 to 0.3 million people in the urban population, as specialists from the entire medical arena are employed and deployed in such rural health centers. It is only in this manner can we provide these misinformed people the best of contraceptive services as well as contribute to the improvement of overall health and demographic statistics and thus lead to the development of the nation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.