
Abstract
The aim of this 5-year longitudinal cohort study was to assess the prevalence, severity, and trends in caries increment and impact of the School Dental Incremental Care Programme (SDICP). Data were gathered from school dental records as part of the SDICP. A sample of 1830 children were included and checked for caries experience annually using World Health Organization criteria. In total, 95.4% of the children were caries free in 2004, and caries experience declined to 70.5% in 2009 with an average of 4.9% annually. At baseline, the mean DMFT (confidence interval [CI]) was 0.06 (0.05-0.08) and increased to 0.58 (0.53-0.63) in 2009. Children with active caries were 4.4% in 2004, and figures rose to 9.6% in 2009. The FT component increased most rapidly during these 5 years from 0.2% to 25.1%. Overall caries prevalence and increment was low in this study. Proportions of FT component were higher as compared with DT component with low rate of extractions during the latter years of the study.
Introduction
Dental caries remains one of the most common preventable public health problems throughout the world. It is the primary cause of oral pain and tooth loss, which lead to chewing difficulties, speech problems, general health disorders, psychological problems, and ultimately lowers quality of life. 1 The treatment of dental caries is expensive, sometimes leading to complex procedures of treatment and rehabilitation. Consequently, it imposes a massive financial burden for the individual and society. 2
Globally, caries prevalence and pattern have changed considerably over the past 3 decades. In most industrialized countries, the prevalence of dental caries and the mean dental caries experience in children have declined tremendously. Malaysia is one of the few developing countries that has declining caries prevalence though not as dramatic as in the industrialized countries.3-5 The National Oral Health Survey for Schoolchildren (NOHSS) has been conducted by the Ministry of Health, Malaysia about every 10 years since the 1970s.6-8 These successive surveys confirm the declining trends of dental caries in Malaysia. These changes are often ascribed to the national water fluoridation policy since 1976, availability of affordable fluoridated toothpaste in the Malaysian market, changing living conditions and lifestyle, effective use of oral health services, adaptation of self-care practice, and implementation of school-based oral health care programs.7-9
According to NOHSS, the dental caries prevalence for the 12-year-olds in peninsular Malaysia declined from 78.4% (1970-1971) to 71.3% (1988), to 57.1% (1997), and to 39.0% (2007). Caries experience for the same age group also declined from a mean DMFT (decayed, missing, filled teeth) of 3.7 (1970-1971) to 2.37 (1988), to 1.6 (1997), and to 1.5 (2007) in peninsular Malaysia.6,10 In this study, data were collected from the 2 districts of peninsular Malaysia, Shah Alam and Seberang Prai. These regions have contrasting socioeconomic features. Seberang Prai is a suburban district with a mix of urban and rural areas whereas Shah Alam is a sprawling modern city located in well-developed Klang Valley. Both, Shah Alam and Seberang Prai have access to public water supply with fluoride level of 0.5 to 0.8 ppm since 1976. 11 Apart from water fluoridation, fluoride tooth paste is widely available in the markets of both areas.12,13
Although, water fluoridation and fluoridated toothpaste are the 2 main strategies to prevent dental caries, there is still a need for school-based oral health education and preventive programs to promote good habits such as regular tooth brushing, flossing, and diet control. 2 To promote good preventive oral health behavior, the Oral Health Division, Ministry of Health launched the School Dental Care Programme in all the states of Malaysia in 1984. It is a comprehensive and systematic incremental dental care programme to render school children orally fit before they leave school. In this programme, dental therapists visit primary schools annually and perform oral health education instructions to children and also provide curative care free of charge. Every year, more than 90% of primary school children benefit from this programme. By year 2000, more than 800 schools in Malaysia had a dedicated school dental clinic to cover almost 92% of primary and 60% of secondary school children. 14
There are adequate cross-sectional data available to measure dental caries prevalence in school children in Malaysia. However, there is a need for longitudinal cohort studies starting from the earliest possible age to provide information on caries increment and impact of the school dental health programs in Malaysia as well as identifying school children who are at risk of developing childhood caries to be targeted for specific and cost-effective preventive measures. Therefore, this study was conducted to assess (a) the prevalence, severity, and trends in caries increment; (b) the association of dental caries increment with gender and ethnicity; and (c) the impact of the incremental School Dental Care Programme on the prevalence, severity, and trends in caries increment in a 5-year longitudinal cohort.
Method
The research protocol for this study was approved by the Research Ethics Committee of Universiti Teknologi MARA. This 5-year longitudinal cohort study included primary school children initially aged 6 years attending government-aided schools in the city of Shah Alam and mixed urban–rural districts of Seberang Prai, Malaysia.
A multistage cluster random sampling was used in the study. During the first stage, schools were randomly selected from both the districts as clusters. At the second stage, the children’s dental records were selected from each selected school by using simple random sampling. An error of 5% and power of 80% was accepted for the purpose of sample size calculation. Using the proportion-based sample calculation formula, 15 a minimum sample size of 737 children was needed for the study. To allow exclusion of incomplete records, the initial size was more than doubled.
Data were gathered from school dental records, collected as a part of the School Dental Incremental Care Programme run by the Ministry of Health, Malaysia. Passive informed parental consent was obtained at the beginning of this programme. All clinical examinations and records were done by trained dental therapists. All the participants were examined in the first year of primary school at 6 years of age. The clinical data represented records of the dental status and treatment given to each child was kept by the school administration. These record cards included the information about demographic data (age, gender, ethnicity), oral health condition (caries experience, gingivitis), and treatment need for each children from 2004 to 2009. All included children were examined every year from 2004 to 2009. Caries experience of each child was recorded annually using World Health Organization diagnostic criteria for caries namely, decayed (D), missing (M), filled (F) and teeth (T). 16 However, the examiners were not calibrated.
The schools were contacted for permission to retrieve the dental records. For maintaining confidentiality, the subject’s names were not disclosed. One of the authors (NY) examined all the dental records without knowing to which group the records belonged to. All record cards with complete information from 2004 to 2009 were included for data entry and analysis until the minimum sample size was met. All data were entered by 2 dental nurses independently. The 2 data sets were compared and any mistakes were rectified. Analysis was done using SPSS software (version 16.0). Analyses included associations between demographic background and the children’s continuous dental caries development from age 6 years. Descriptive statistics analysis was used to describe the pattern of dental caries. Because of the positively skewed distribution of caries experience, nonparametric tests (Kruskal–Wallis and Mann–Whitney U tests) were used to compare DMFT values between categories. Model estimates reported mean DMFT with 95% confidence interval (CI). The P value of <.05 was chosen as the level of significance for all statistical calculations.
Results
The final sample size consisted of 1830 record cards. The gender distribution was almost balanced (52% boys and 48% girls). The ethnic mix of the sample consisted of 44.2% Malays, 31.1% Chinese, and 21.5% Indians. About 40.3% of the children were enrolled in Shah Alam schools and 59.7% in Seberang Prai. The majority of the children were from urban schools (65.6%) and the rest from rural schools (34.4%).
Table 1 shows the distribution of DMFT and caries-free children. The majority of children (95.4%) were caries free (ie, DMFT = 0) in the year 2004. This percentage of caries-free children declined steadily throughout the 5 years of study to 70.5% in 2009. The average decline in proportion of caries-free children over the 5-year period was 4.9% annually. At baseline in 2004, the mean DMFT (CI) was 0.06 (0.05-0.08), ranged from 0 to 4; and only 1 child out of 1830 was classified as high caries experience (defined as DMFT >4). At the end of 5 years in 2009, the mean DMFT (CI) increased to 0.58 (0.53-0.63) with a range from 0 to 8, whereas the percentage of children with high caries experience also increased to 7.6% (48/1830). The prevalence of children with high caries experience was 3 (0.2%) in 2005, 11 (0.6%) in 2006, 22 (1.2%) in 2007, and 37 (2.4%) in 2008.
Distribution of DMFT and Caries-Free Children (DMFT = 0) by Cohort Year.

Abbreviations: DMFT, decayed, missing, filled teeth; CI, confidence interval.
Table 2 describes the trends of DT, FT, and MT components among the children during the study period. Of the 1830 children, 81 children presented with active dental caries, with a prevalence of 4.4% in 2004. These figures rose to 175 children with active caries giving a prevalence of 9.6% in 2009. The FT component increased most rapidly during the 5-year period from 0.2% to 25.1%. MT component contributed the least to DMFT with no missing teeth in any child in 2004 and 2005. At the end of the study in 2009, only 20 children had 1 permanent tooth extracted and only 3 out of 1830 had 2 permanent teeth extracted.
Distribution of DT, FT, and MT Components and Caries Level by Cohort Year.
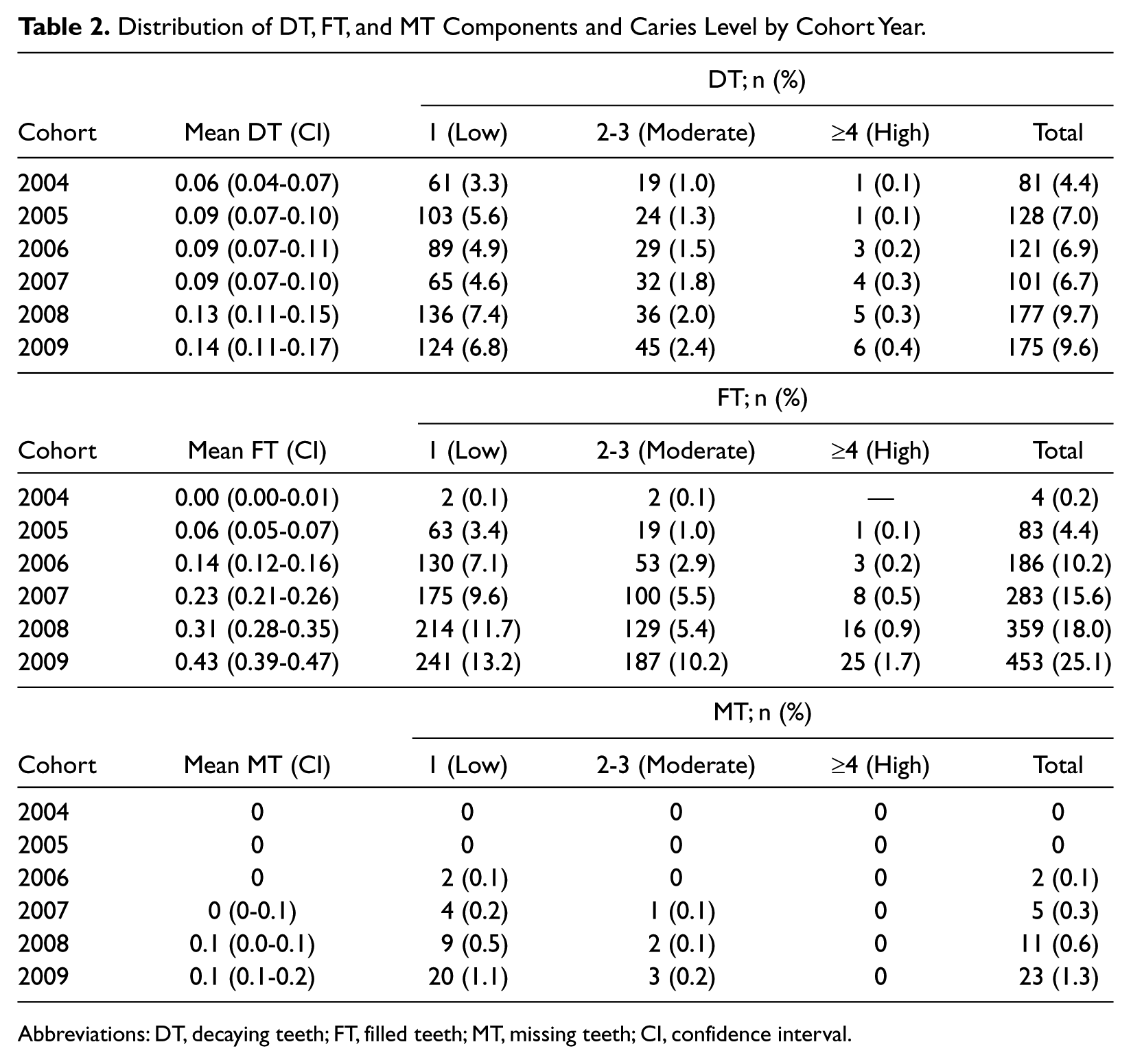
Abbreviations: DT, decaying teeth; FT, filled teeth; MT, missing teeth; CI, confidence interval.
Table 3 shows the differences in mean DMFT between genders, where girls showed higher DMFT during all the years of study. However, the differences were not statistically significant at any year (P > .05). Similarly, no statistically significant differences were found among the three ethnic groups although Indians maintained the lowest mean DMFT throughout the study period.
DMFT Trends by Gender and Ethnicity.
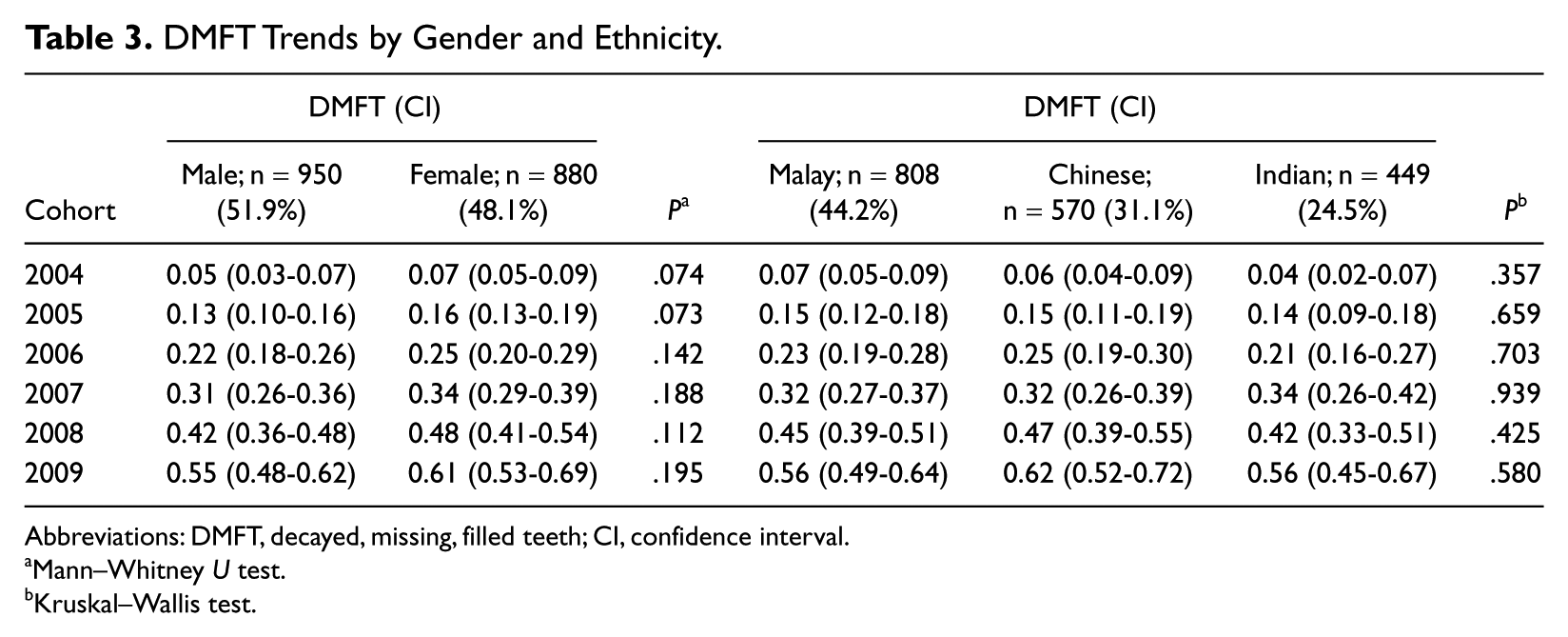
Abbreviations: DMFT, decayed, missing, filled teeth; CI, confidence interval.
Mann–Whitney U test.
Kruskal–Wallis test.
Discussion
The present study provides evidence of relatively low caries prevalence and increment in the cohort of 6-year-olds during the 5-year study period. These results show slightly lower (DMFT 0.58) caries prevalence among children at the end of the study as compared with previous national data and other studies (DMFT 1 to 1.1) in Malaysia.6,8,10 This may be attributed to the successful implementation of the water fluoridation programme in both areas, availability of fluoridated toothpastes, and implementation of Incremental School Dental Care Programme in Malaysia. The DMFT and rate of caries increment have been significantly reduced in the present cohort of 6-year-old school children, irrespective of their gender and ethnicity. The mean DMFT also appears lower than that recorded in other states of peninsular Malaysia especially in states where the implementation of water fluoridation has been erratic or discontinued. For example, the Health Information Management System dental caries data for the state of Terengganu and Kelantan showed, in contrast, a DMFT of 2.1 and 2.2 among their 12-year-olds, respectively. This may partially be credited to the less coverage of school children by Incremental School Dental Care Programme in Kelantan (30%) compared with Selangor (59%) and Penang (81%). Although Trengganu has relatively higher coverage of 75% of school children by the dental care programme, caries prevalence still remains high. It may be because of the termination of water fluoridation in this state. 10
The DT component contributed most to the DMFT scores in 2004 and 2005 indicating that untreated caries was a problem for the children at the age of 6 and 7 years. Whereas, the FT component contributed most for the years from 2006 to 2009 onward showing higher prevalence of treated carious lesions, which constantly increases from 2004 to 2009. This pattern may be because of the time-dependent exposure to the School Incremental Dental Care Programme. Overall, the “F” component was higher as compared with the “D” and the “M” components, indicating more treatment needs being met while minimizing early tooth loss from extractions. It also strengthens the argument that these incremental dental care programs are generally oriented toward curative care.
The World Health Organization target for oral health by the year 2010,10,17 which proposes that 90% of 5-year-olds should be caries free (considering caries experience at cavitation level), seems to be achieved with more than 95% of 6-year-old children being caries free. The target for 12-year-olds, that is, at least 60% children caries free and mean DMFT of less than 1.5 was also achieved with more than 70% caries-free children and mean DMFT 0.58. This is partly because of the well-organized implementation of the school oral health programme. Furthermore, the present study shows a gradual increase of high caries risk children (DMFT > 4) from 2004 to 2009. These findings indicate the need for early identification of this high-risk group and clearly demonstrate the requirement for launching professionally applied preventive approaches for this group to reduce or retard the progression of childhood caries.
The increased caries experience with age found in the present study has been described in many countries,2,18,19 but it does not mean that the oldest are the most susceptible for caries. Actually, the measurement of DMFT is cumulative and caries occurrence also depends on exposure time. The main finding in the present study is that, on average there was a 4.9% decrease in the caries-free population per year. This indicates the need for the implementation of more preventive and health promotion approaches in the school dental care programme. Additionally, alternative vehicles for fluoride administration need to be evaluated and implemented according to local characteristics. In a recent study on Malaysian school children, Chen et al 20 suggested that weekly use of fluoridated mouth-rinse in school children can be an excellent additional preventive approach. Based on the available evidences, the incorporation of fluoride mouth-rinsing programme can be recommended in existing incremental school dental care program in fluoride-deficient areas. Additionally, to get maximum benefit of caries prevention and target high-risk group, mouth-rinsing programme could be combined with other preventive activities such as fissure sealants application. 20 Despite the widespread use of fluoride and school oral health care programme, there seems to be a continuous increment of new decayed teeth every year. The possible reason for this is the high sugar consumption in the Malaysian population, which is one of the important etiological factors that needs to be undertaken for caries prevention. The annual per capita consumption of sugar has been fairly stable in Malaysia and has varied between 43 and 46 kg per person per year from 1994 to 2005. 3 These are very high levels compared with the global consumption data. Even though the direct consumption of sugar has decreased in recent years, the consumption of sugar in products such as soft drinks, confectionaries, cookies, buns, and so on, has increased. It is well established that the intake of sugary beverages, especially in children, is an essential risk factor for caries.21,22 This indicates that educational program intended to prevent caries on deciduous teeth should start during the first year of life as soon as the first teeth erupt, before the condition becomes difficult to prevent and expensive to treat.
In this study, no significant differences of caries experience were found between ethnic groups. The Chinese had the highest DMFT score of 0.62 whereas Indians and Malays had a lower score of 0.54. The most recent Malaysian National Oral Health Survey of 12-year-old school children in 2007 showed highest mean DMFT score among Malays (1.03) followed by Chinese (0.78) and lowest among Indians (0.45). 23 Additionally, results of the present study are not in agreement with previous studies on similar population, which showed that Indians usually had the lowest caries experience.6,8,13 This disagreement may be because of the poor understanding of the effects of other socioeconomic conditions on oral health outcome. 24
One of the limitations of the present study was that it relied on uncalibrated dental caries data, which were present in record cards filled by different dental therapists over a period of 5 years, who screened and treated the school children every year. Although the accuracy, according to exacting epidemiological standards, may be questioned, data from records do provide a very useful tool to measure disease trends because they do not incur additional costs or the need to organize nationwide surveys in 5- or 10-year intervals. As such, this type of data mining procedure should be encouraged and the findings interpreted with this caution in mind. Second, some other explanatory variables (eg, family income level, mother’s education status, oral health behavior, and microbiological factors) were not recorded in this school dental care program, and consequently, cannot be included in this study. These variables, especially the roles of parents in preventing dental caries, play an important role in caries development and should be considered in further studies. 25 The inclusion of these variables would probably clarify how they mediate the effect on caries occurrence. In a hierarchical approach, distal determinants (such as age, gender, maternal level of education, and income) and proximal determinants (such as oral health behaviors or microbiological factors) should not be treated as equivalent. 26
Conclusion
In summary, the overall dental caries prevalence and increment was low in the cohort of 6-year-old school children in Malaysia who lived in a fluoridated area. The proportions of treated dental caries were higher as compared with active decay during the latter years of the study when the incremental dental care program made its impact. However, it is crucial to target dietary control and clinical prevention to the small number of identified high caries risk children in order to make the incremental dental care program more effective and beneficial. At this stage, it is crucial to increase awareness among children and their parents of the health and oral health consequences of high sugar consumption.
Footnotes
Acknowledgements
The authors gratefully acknowledge the support of the Oral Health Division, Ministry of Health, Malaysia for providing data. Thanks to the all staff nurses involved in data collection from Seberang Perai and Shah Alam: Norli Hamzah, Nurul Hana Roslan, Siti Zainalisa bt Hashim, Norhayati bt Othman, Maryaton Kitbiah bt Abu Bakar, Noor Azreen bt Ahmad, Siti Zaria Amini bt Mohd Amin, Mazlinda bt Mohalil, Lim Lean Yeng, Aminah bt Baharum, Yeoh Moy Heng, Oh Yoke Swan, Wong Lai Thiang, Suraini Md Sahat, Lau Cheng Choo.
Authors’ Note
All the authors provided input into drafts and approved the final draft of the article. MM contributed to data analysis and article writing; NY contributed to the design of the study and write up. MIAH and NJ contributed to conceptual framework of the project and data interpretation. All authors read and approved the final version of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed the receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for the research from Research Management Institute, Universiti Teknologi MARA, Shah Alam, Malaysia. Grant Number / File Number: 600-RMI/ST/DANA 5/3/Dst(89/2009).