
Abstract
This study investigated the relationship between intention of undergoing cancer screening and information, motivation, and behavioral skills using an information–motivation–behavioral skills model. The authors performed a telephone survey of a random sample of 2030 residents aged 30 to 69 years from 6 counties of Gangwon province, South Korea from July 15 to July 25, 2009. Questions about information, motivation, and behavioral skills were examined using a confirmatory factor analysis and relationships among factors were analyzed using a structure equation model. The intention of undergoing cancer screening showed a positive relationship between intention to undergo cancer screening and information(r = .134, P < .001), social norms(r = .059, P = .009), and behavioral skills(r = .129, P < .001). Therefore, comprehensive intervention considering motivation and behavioral skills as well as information is necessary to improve cancer screening rates.
Introduction
Cancer is the leading cause of death in Korea with incidence rates per 100,000 of 229.8 persons (in 2002), 245.6 (in 2004), 263.2 (in 2006), and 286.8(in 2008), an increase of 3.3% per year. According to the 2010 International Agency for Research on Cancer report, the incidence rates of cancer in Korea have shown the highest among Asia Pacific region. 1 According to a previous study that followed 39 625 cancer patients for cancer reoccurrence from March 1995 to December 2004, the 5-year average survival rates were as follows: 85.8% for cases involving first stage detection; 67.5% in cases of second stage detection; 38.1% in cases of third stage detection; and 10.1% in cases of fourth stage detection. Based on these, the 5-year survival rate in cases of first stage detection was 8 times greater than rates for cases of fourth stage detection. 2
The World Health Organization suggested that national cancer screening programs have been the most effective and efficient method for improving the quality of life. 3 Although the Korean government established the “Cancer Control 10 Years Plan” in 1996, and implemented the National Cancer Screening Program in 1999, cancer screening rates in Korea have remained lower than in other advanced countries.
When developing strategies to increase screening rates, it is important to consider the psychological factors affecting those undergoing cancer screening as well as the development of institutional and political support.
The information–motivation–behavioral skills (IMB) model developed by Fisher and Fisher4-7 has been very useful in explaining the factors associated with the intention to undergo cancer screening. The IMB model suggests that health-related information, motivation, and behavioral skills are important factors in the performance of health behaviors. 4 Furthermore, it indicates that when individuals have information, motivation, and skills for behaviors, the result is a strong intention to change behaviors and maintain these altered habit. This model assumes not only that information and motivation directly affect behaviors but also that behavioral skills influence behaviors.
It has been suggested that information directly relevant to a particular health domain is an initial prerequisite of enacting a health behavior, and that motivation is divided into personal and social types. 8 Personal and social motivation includes attitude and social support, respectively. In the meantime, behavioral skills consist of personal objective skills for performing the behavior and a perceived sense of self-efficacy. 9
The IMB model was invented as a trial for applying sociopsychological concepts, methodology, and measurement skills to describe a current problem. Its usefulness has been proven continuously in cross-sectional studies and experimental intervention studies performed with population groups. This model has been used as a basic concept in many studies conducted with various population groups to predict HIV risk and preventive behaviors, 10 to predict other preventive behaviors for mentally ill patients, 11 in motorcycle safety, 12 and to investigate effective interventions for behavioral change. 13
The purpose of this study was to identify the applicability of the IMB model with respect to the intention of undergoing cancer screening and to suggest influential messages of information, motivation, and behavioral skills related to cancer screening.
The IMB model framework used in this study to predict intention to undergo cancer screening has been described in Figure 1.
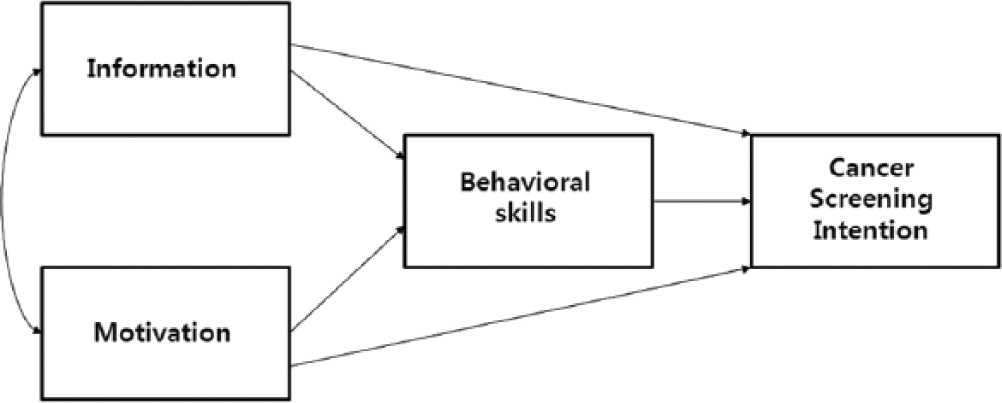
Information–motivation–behavioral skills model for the intention to undergo cancer screening.
Methods
Subjects
The research survey was completed from July 15 to 25, 2009. Participants were selected from 6 major counties in Gangwon province, 1 of 9 South Korean provinces, which consist of 18 cities and counties with 1.5 million people. This study was conducted as part of a study to develop educational messages for improving screening rates at the Gangwon Regional Cancer Center. Participants included 2030 residents (959 male, 1071 female) ranging in age from 30 to 69 years and living in the previously mentioned 6 major counties, selected according to area, gender, and age. A telephone survey was conducted by trained investigators using the structured questions. A random digit dialing method was used to randomly select participants. The phone surveys were continued until the target number was met. After identifying whether the respondents were local residents, those with cancer were excluded from the study.
This study was approved by the Institutional Review Board of the Kangwon National University Hospital.
Questionnaire Survey
Development of questions
The questionnaire was developed through a literature review and a focus group interview with residents from Gangwon province. During the literature review, we referred to research by Cha, 14 which predicted AIDS preventive behaviors using the IMB model.
Six focus groups, divided into level of intention, were conducted among 54 residents aged 40 to 60 years from the same province. Based on the results of focus group interview, information, motivation, and behavioral skills items were developed.
Measurement of items
Questions consisted of sociodemographic characteristics, intention of undergoing screening, and IMB constructs. The questions related to sociodemographic characteristics investigated gender, age, educational background, income level, and marital status. Age was classified into the 30s, 40s, 50s and 60s, and educational background was divided into graduation from elementary school or lower, graduation from middle school, graduation from high school, and graduation from college or higher. Monthly income level was examined by categorizing it into <$800, $800 to $1600, $1600 to $2400, $2400 to $3200, and >$3200, and marital status was categorized as unmarried, married, bereaved, divorced, or separated. In addition, family history of cancer was established.
The information related to cancer screening consisted of the following 5 items, with each item being rated on a 4-point scale from 1 (strongly unaware) to 4 (strongly aware):
Do you know the benefits of cancer screening?
Do you know the side effects of cancer screening?
Do you know the kinds and intervals of cancer screening?
Do you know about the national cancer screening program?
Do you know about the national financial support system for patients diagnosed with cancer?
The motivation related to cancer screening consisted of 8 items. The motivation to perform cancer screening–related behaviors was divided into a cancer screening attitude scale of 5 items on internal motivation and a cancer screening social norms scale of 3 items on social motivation as follows:
I am ashamed of a specific position during the examination.
I am burdened by the loss of time during cancer screening.
I am worried that cancer screening will be painful.
I am anxious about the side effects of cancer screening.
I am anxious about the results of cancer screening.
My family recommended cancer screening.
A friend or a neighbor recommended cancer screening.
A doctor recommended cancer screening.
The 5 items related to internal motivation were rated on a 4-point scale from 1 (strongly agree) to 4 (strongly disagree), and the 3 items related to social motivation were rated on a 4-point scale from 1 (strongly disagree) to 4 (strongly agree).
The behavioral skills related to cancer screening (gastric, colon, breast, liver, and cervical cancer by endoscopy, occult blood test and colonoscopy, mammography, blood analysis and sonogram, and Pap smear test) consisted of 8 items and were divided into a cancer screening perceived self-efficacy scale of 4 items and a cancer screening objective ability scale of 4 items as follows:
Can you endure discomfort during the examination?
Can you endure psychological troublesome during the examination?
Can you endure the fear related to the results of the cancer screening?
Can you undergo cancer screening when you feel physical annoyance?
It is easy to bear the cost of cancer screening.
It is easy to register for cancer screening and to check its results.
It is easy to arrange time for cancer screening.
It is easy to understand the results of cancer screening.
Each item was rated on a 4-point scale from 1 (very difficult) to 4 (very easy).
The intention to undergo cancer screening was measured using the question, “Are you willing to receive cancer screening in the future?” (yes or no)
Data Analysis
Data analysis was performed with PASW 17.0 and AMOS 18.0. To examine sociodemographic characteristics of the respondents, descriptive analysis was conducted and then a confirmatory factor analysis was done to classify questions related to information, motivation, and behavioral skills for the intention to undergo cancer screening.
To identify factors associated with the intention to undergo cancer screening within the IMB model, an analysis using the structure equation model (SEM) was conducted with information, motivation (attitude, social norms), and behavioral skills (perceived self-efficacy, personal objective ability) as pertaining to cancer screening as independent variables and the intention to undergo cancer screening as a dependent variable. Model Fit was evaluated to interpret the results of the analysis of the SEM.
We evaluated the model fit with primarily used indexes such as χ2, root mean square error of approximation (RMSEA), and comparative fit index (CFI). The index of χ2 verified the null hypothesis that the model completely fit the data based on a theory that data follow a normal distribution. The RMSEA could range from 0 to ∞, with smaller values indicating a closer fit; specifically, values of 0.05 or lower indicated a close fit, values of 0.08 or lower indicating a reasonable fit, and those ≥0.10 indicating a poor fit. 15
In an effort to develop powerful educational messages, a logistic regression analysis was performed with intention to under cancer screening as the dependent variable and information, motivation, and behavioral skills as independent variables.
Results
Sociodemographic Characteristics of Respondents
The sociodemographic characteristics of respondents are provided in Table 1. The respondents included 959 males (47.2%) and 1071 females (52.8%), with those in their 40s accounting for the largest proportion (31.2%). The educational levels of 783 (38.6%), 648 (31.9%), and 350 (17.2%) were graduation from high school, college or higher, and elementary school or lower, respectively.
Sociodemographic Characteristics of Respondents (N = 2030).
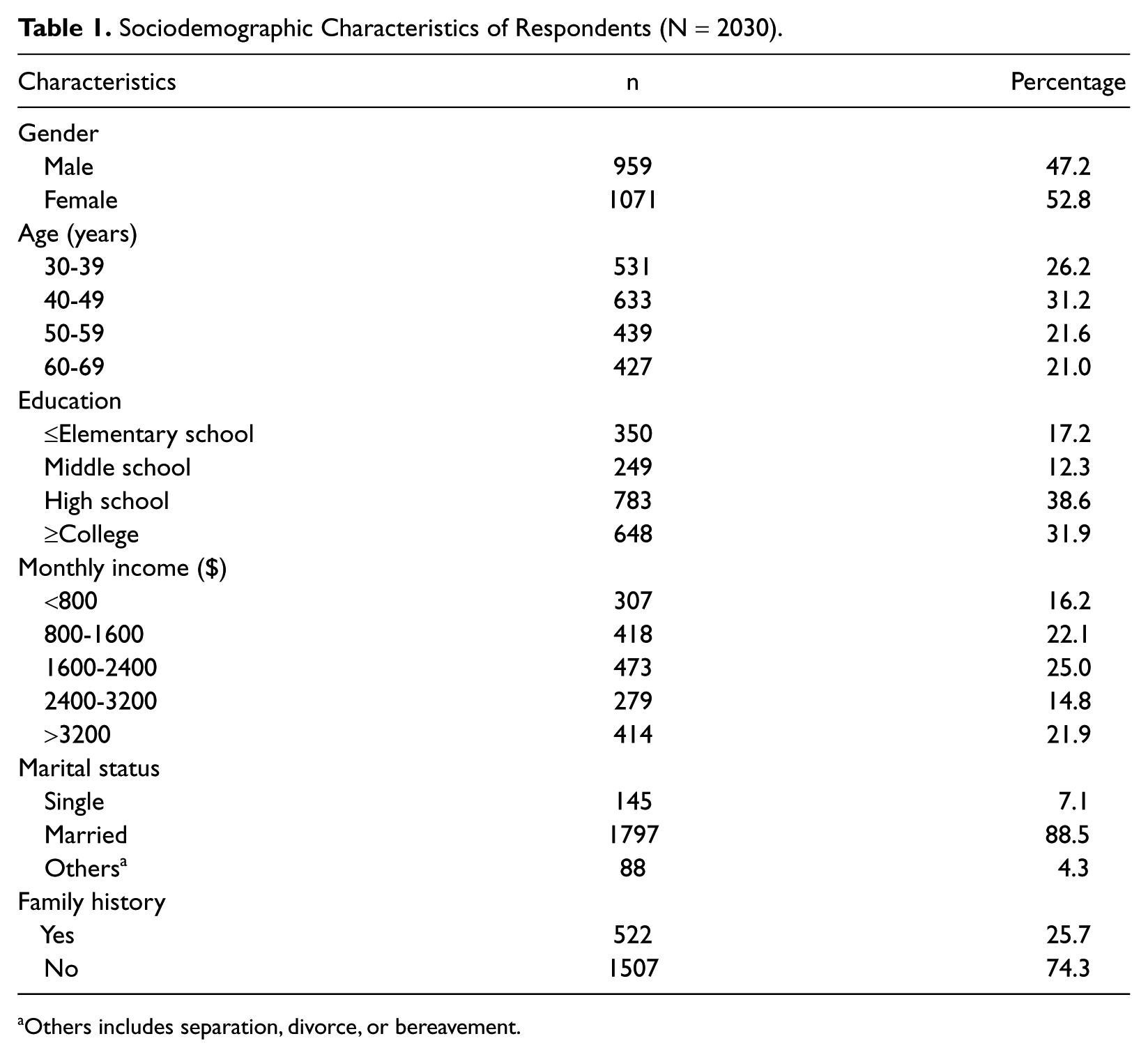
Others includes separation, divorce, or bereavement.
Relationship Between IMB Factors
A confirmatory factor analysis was conducted after the initial development of questions and the final questions were confirmed by excluding questions on behavioral skills with a standardized factor loading of 0.371. Means and their standard deviations, factor loadings, and reliability concepts from a confirmatory factor analysis have been presented in Table 2.
Summary of Statistics and Factor Loadings From a Confirmatory Factor Analysis.
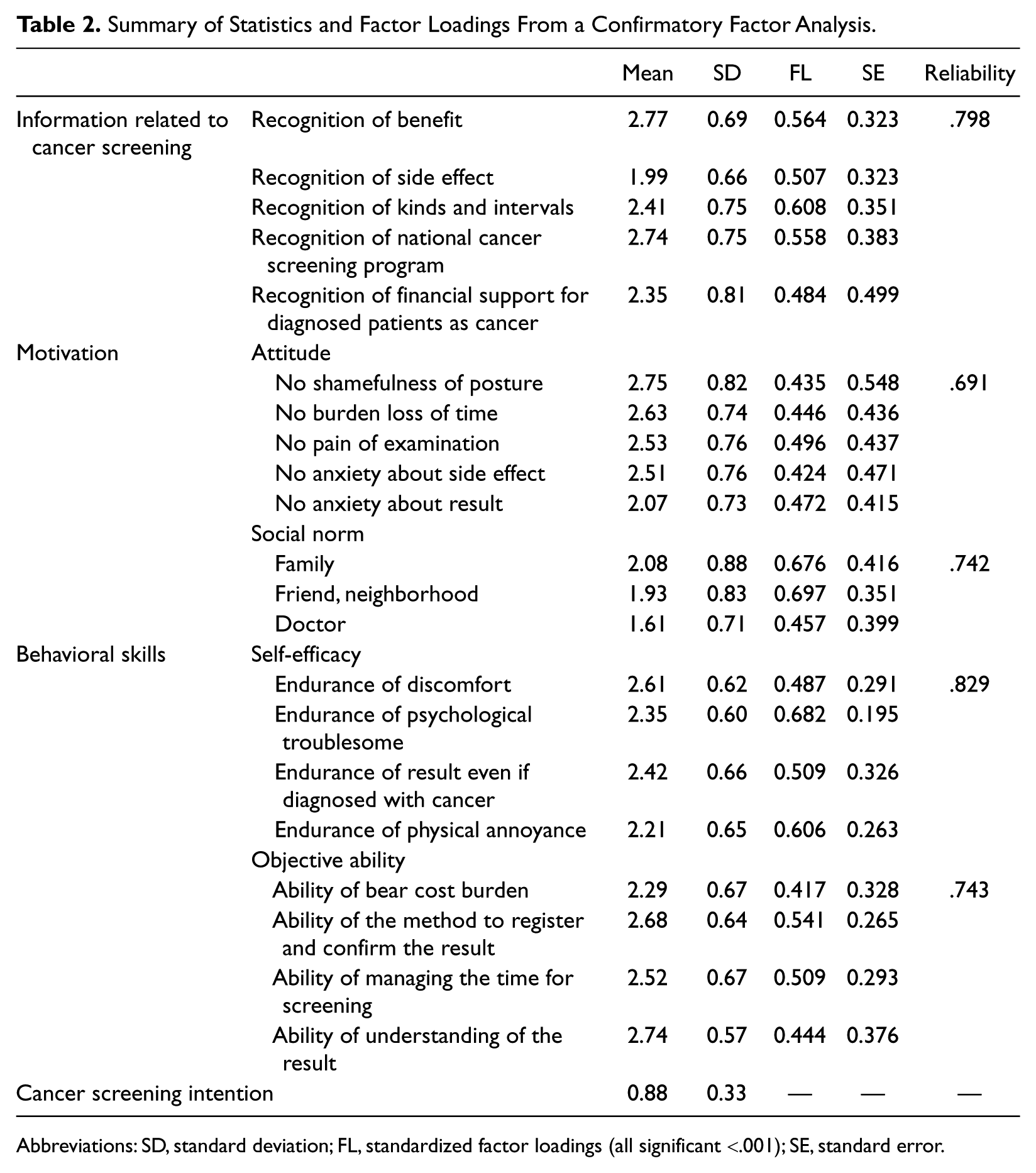
Abbreviations: SD, standard deviation; FL, standardized factor loadings (all significant <.001); SE, standard error.
All variables related to information about cancer screening showed statistical significance (P < .001). Reliability concepts related to the 5 information items recorded .798 demonstrating that they had internal consistency.
With respect to variables related to motivation, including measurements of attitude and social norms, variables related to attitudes about cancer screening were statistically significant (P < .001). The reliability of the 5 items about attitude was .691. All variables related to social norms about cancer screening were also significant P < .001), and reliability of the 3 items was .742 meaning that they had internal consistency.
Among behavioral skills about cancer screening, all variables related to perceived self-efficacy about cancer screening were statistically significant (P < .001) and reliability concepts of its 4 items recorded .829, which was interpreted as having internal consistency. All variables related to personal objective ability about cancer screening were also statistically significant (P < .001), and the reliability of its 4 items was .743 indicating that they had internal consistency.
Analysis of IMB Structure Equation Model
The IMB SEM of respondents is presented in Figure 2. According to analysis of the SEM, this measurement model demonstrated good data fit, χ2 = 1.377, df = 1, P = .241, CFI = 0.999, RMSEA = 0.014.
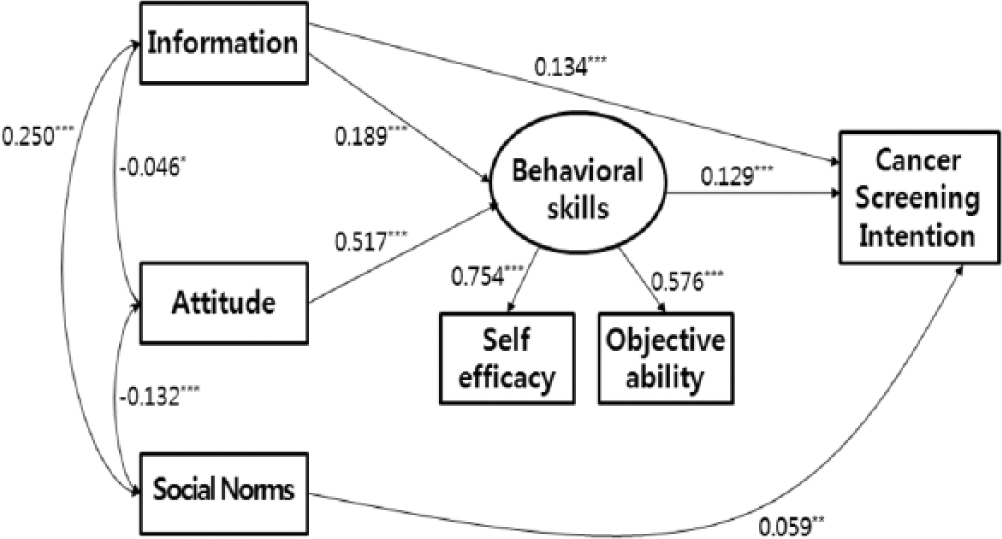
Structure equation model depicting significant regression paths in the information–motivation–behavioral skills model for respondents.
The information and attitude related to cancer screening had a positive relationship with behavioral skill (r = .189, P < .001 and r = .517, P < .001, respectively).
The results of an analysis of factors associated with the intention to undergo cancer screening showed a positive relationship between intention to undergo cancer screening and information (r = .134, P < .001), social norms (r = .059, P = .009), and behavioral skills(r = .129, P < .001).
IMB Factors Affecting Cancer Screening
The results of a logistic regression analysis of the intention to undergo cancer screening are provided in Table 3. For information about cancer screening, the better informed subjects were about the benefits of cancer screening (odds ratio [OR] = 2.05, 95% confidence interval [CI] = 1.68-2.51), and the national financial support for diagnosed cases (OR = 1.26, 95% CI = 1.05-1.51) meant that they were more likely to have the intention of undergoing cancer screening.
Odds Ratios (ORs) and 95% Confidence Intervals (CIs) for the Effect of Information, Motivation, and Behavioral Skills on the Intention to Undergo Cancer Screening.
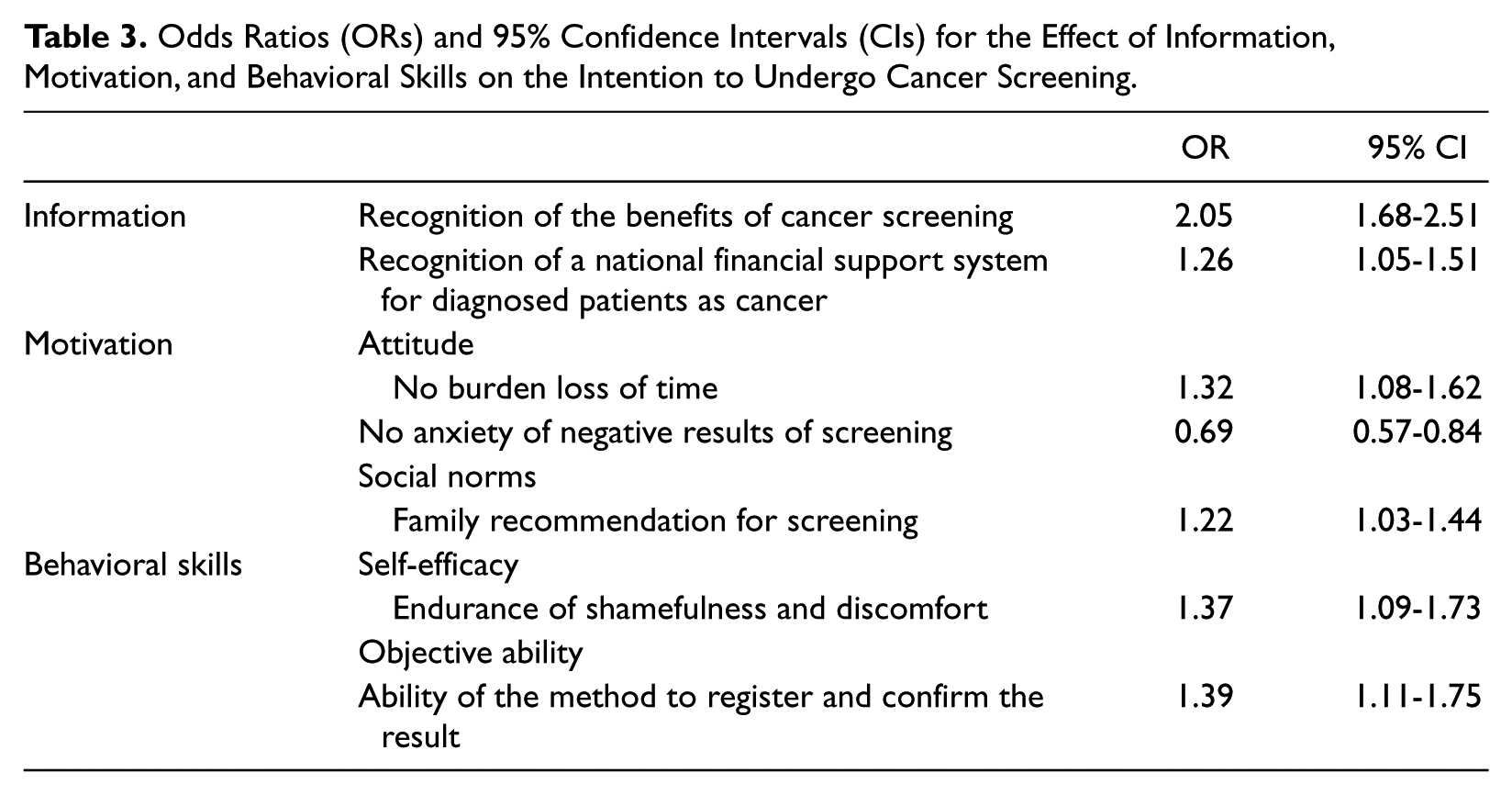
With respect to motivational factors, cases that had less burden of time loss for cancer screening showed a stronger intention of undergoing cancer screening (OR = 1.32, 95% CI = 1.08-1.62) and cases that had more anxiety about the results of cancer screening showed a weaker intention to undergo cancer screening (OR = 0.69, 95% CI = 0.50.84). Furthermore, family recommendations for cancer screening were demonstrated to exert a significant impact on the intention to undergo cancer screening (OR = 1.22, 95% CI = 1.03-1.44).
Finally, behavioral skills such as endurance of discomfort during cancer screening (OR = 1.37, 95% CI = 1.09-1.73) and the ability to register and confirm the results (OR = 1.39, 95% CI = 1.11-1.75) were significantly related to the intention to undergo cancer screening.
Discussion
To raise cancer screening rates, a multidimensional approach is required given that complex reasons are involved as to why people choose not to undergo cancer screening.
To date, several studies predicting influential factors on cancer screening have focused on health behavior theories such as the “health belief model (HBM),” 16 the “theory of planned behavior (TPB),” 17 and the “social learning theory.” 18 The HBM demonstrated that perceived susceptibility, perceived benefits, and general health motivation affected the intention to get pap smears, 19 and the TPB suggested that social norms and perceived behavioral control were significantly related with college female students’ intentions to get Pap smears. 20 In addition, the social learning theory used self-efficacy to predict cancer screening. Additional studies have reported that higher self-efficacy was associated with higher intention to undergoing breast cancer screening. 18 In summary, factors associated with undergoing cancer screening in various models were information on cancer, expected benefits from cancer screening, social norms, perceived behavioral control, and self-efficacy to behavioral performance. Therefore, it is necessary to develop a more comprehensive and systematic model integrating the various related factors.
This study used the IMB theory to determine factors influencing the intention to undergo cancer screening. In a previous study by Misovich et al, 21 the IMB model was applied as a tool to understand the intention of breast self-examination (BSE). They suggested that the usefulness of the model lay in its ability to predict the behavior and to develop strategies for educational message. Although they addressed the behavioral skills that influenced adherence to the BSE, they did not emphasize behavioral skills with respect to undergoing cancer screening such as mammography, endoscopy, and colonoscopy because these screening tests are conducted by medical equipment unlike BSE.
However, our study suggested that there are skills that are needed for the behaviors related to cancer screening, and that these skills can have an impact on the intention to get screening. The skills are the abilities to endure discomfort and fear during the screening test, to know how to apply the test and check the results, to make screening appointments, and to understand the screening test results. Therefore, although people had prior knowledge of its importance and positive attitudes toward cancer screening, they tended to fail in fulfilling the behavior if they had no appropriate ability for performance screening.
The present Korean government has promoted the screening program for 5 cancers: gastric, colon, breast, liver, and cervical. These screening tests have included endoscopy, occult blood test and colonoscopy, mammography, blood enzyme analysis, liver sonogram, and Pap smear tests.
The results of our study have shown the fact that some skill is needed to undergo cancer screening and these skills must be provided to communities as a whole.
In the results of our analysis, motivation and information combined with behavioral skill was related to the intention to undergo cancer screening.
When factors affecting behavioral skills related to cancer screening were examined, the skills were improved when the subjects had more information related to and better attitudes about the screening. In correlation with behavioral skills, attitude was observed to be related more closely than information. The findings of this study were the same as that of Misovich et al, 21 which investigated BSE based on the IMB theory. According to it, information on and motivation of BSE were significantly related with behavioral skills (β = 0.13, P < .05 and β = 0.59, P < .01, respectively). Comparing regression coefficients, the effect of motivation on behavioral skills was higher than that of information and therefore the efforts to increase positive attitudes toward cancer screening is more effective rather than just providing information and knowledge for people.
With respect to motivational factors, higher social norms led to a significantly higher intention to undergo screening in our results. A similar finding was observed in a previous study by Misovich et al, 21 which reported that higher social norms of BSE were associated with higher examination rates. Also, a study by Bae et al, 22 which examined influential factors affecting participation in cancer screening of Koreans based on the social ecological model, showed that higher social norms related to stomach cancer screening was related with higher stomach cancer screening. Social norms related to cancer screening were considered to be an important index of future participation in cancer screening. These finding suggest that collectivism, which is a typical characteristic of Korean society, needs to be taken into account in developing health programs in the community. In particular, the family’s recommendation on cancer screening was significantly related with the intention to participate in cancer screening. Given that Korea is a family-centered society, previous studies also showed a high influence of family. Therefore, a family unit cancer screening program or other cancer screening programs, which can be recommended through family, will be effective strategies in enhancing participation rates.
Finally, better behavioral skills related to cancer screening were significantly associated with higher intention of participating in cancer screening. A previous study by Son et al 23 applying TPB to predict cancer screening behavior in Koreans showed that higher perceived self-efficacy influenced significantly behaviors for early detection of breast cancer. Another study by Jirojwong et al 24 using the health belief model showed that self-efficacy was positively associated with Pap smears. 24
According to the results of the logistic regression analysis, there was significantly influential information about the benefits of cancer screening and the national financial support systems for diagnosed person. A previous study by Tong et al, 25 who studied the factors affecting screening test by fecal occult blood testing, found that individuals more interested in information related to colon cancer had plans to be screened at 6.7 times that of individuals less interested. Such information can reduce anxiety about the results of cancer screening.
A previous study by Kwak et al, 26 which examined influential factors related to undergoing cancer screening in Koreans, reported that the anxiety delayed cancer screening in many cases. Our result showed the similar finding that special skills such as methods to endure the discomfort during cancer screening are necessary.
Meanwhile, consideration for increasing the compliance of follow-up in addition to increasing the screening rate is also needed. The representative study of explaining the necessity of follow-up of screening was performed by Pisani et al. 27 They conducted a randomized controlled trial of effect of clinical examination of the breast on breast cancer mortality in Manila, Philippines. In their result, they pointed out that females with positive result had low follow-up and low compliance rates on clinical examination of the breast.
Therefore strategies, including motivation and behavioral skills as well as information, are necessary not only to increase the screening rate but also to raise the compliance of follow-up. In this sense, our result has supported the importance of provision of information, motivation, and skills to the community people.
There were some limitations to our study. We performed a cross-sectional survey and thus, we cannot make any causal relationship according to time. Also, we chose intention as the dependent variable and thus, we were unable to find long-term effects of information, motivation, and behavioral skills related with cancer screening. With respect to survey methodology, we conducted telephone interviews and so, the questionnaire surveys used were unable to examine many issues in detail. Furthermore, random digit dialing neither had information about the number of calls made nor number of attempts, and hence it is difficult to have the representativeness of final sample.
Despite the limitations, this study was not limited to one hospital or specific subjects. This study could be useful because it studied all targeted individuals for screening programs throughout the whole area with respect to information, motivation, skill, and the intention to undergo screening for cancer.
This study should be regarded as a useful case showing that the IMB model is applicable in predicting cancer screening, and it demonstrates which specific messages influence the intention to undergo screening.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.