
Abstract
Large-scale malaria control activities in China have been conducted with significant success, since the launch of the nationwide malaria control program. This study investigated the malaria distribution in China, particularly in provinces with high risks. Spatial and temporal data were assembled for all endemic or historically endemic areas and combined to identify common patterns and to investigate the actual changes in the burden of malaria in the country. Data were analyzed and the progress in malaria elimination feasibility was discussed. The results indicated that the current distribution of malaria and vectors associated could provide evidence on the assessment of the feasibility of the malaria elimination in China.
Introduction
Malaria is, and has been, the most important parasitic disease of man in terms of mortality, morbidity1-3 and effect on life generally, using “parasitic” in the narrower meaning of the animal parasites: worms and protozoa. 4
Historically, malaria has been a major health problem in China and references to what was almost certainly malaria occur in Chinese document from about 2700
Recent studies have examined malarial distribution patterns around the world, including the global distribution of malaria, 13 population at risk, 13 and the global distribution of falciparum malaria.1,14 Others studies have investigated malaria distribution patterns in China, particularly in provinces with high malaria risks. For instance, studies have examined the geographic distributions, demographic patterns, and temporal trends of falciparum malaria in China, 9 spatial distribution and clustering of malaria in Anhui, 15 and spatiotemporal distribution pattern of malaria in Yunnan 16 and in Hainan.17,18 In this study, we aim to identify common patterns and investigate the actual changes in the burden of malaria in China. We undertake case studies of several provinces to explore the central trends, using available data from similar or related published scientific studies.
Methods
Assuming that the most common channel of communication in the scientific community for sharing information about emerging and endemic diseases is publication in scientific journals, we performed a comprehensive literature review of notified malaria cases using retrospective study. An electronic data search was undertaken through Medline to identify a complete review from World Health Organization, UNICEF, Roll Back Malaria, the World Bank, National Program for Malaria Control, and other scientific reports. Criteria for selection included all reported scientific publications related on malaria morbidity and mortality risks, defined through epidemiological studies. Selected studies regions were classified, as high malaria endemic, with potential malaria transmission or historically or currently malaria free. All articles were reviewed to identify the studies meeting the criteria for selection. We included reports of laboratory that confirmed Plasmodium for both endemic and epidemic events. Full articles were obtained for all original reports. To identify articles for reported malaria events, we used different keywords: malaria burden, malaria control in China, cost-effectiveness, vector control, malaria transmission, malaria epidemic, malaria endemic, insecticide-treated nets (ITNs), indoor residual spraying (IRS), and artemisinin-based combination therapy. We identified regions where malaria is endemic or has been endemic in the past. Then, we compared the temporal and geographical distribution of cases reported. The classification of a region as malaria endemic is not necessarily based on malaria cases and deaths reported in the regions health information system or in general literature. Some provinces where great effort has been made for reducing malaria burden were considered among the malaria endemic. This was done because in remote areas; particularly at the village level, many people are treated at home or in private facilities that do not report to the national health information system. We consider that a region is malaria free when it meet the criteria of a malaria-free area (zero incidence over 3 consecutive years) as defined by the World Health Organization. We also use sibling history data from household surveys and published works reporting population-based studies of insecticide coverage for both national and subnational.
Results
This study shows that great efforts to control malaria in China have been made over the past 50 years, resulting in a significant and continued decline of the prevalence between 1984 and 1993; however, the incidence rate has risen slightly since 2001 with occurrence of local outbreaks in some regions where the disease had previously disappeared. The annual incidence rates of malaria were 3.07, 4.62, 3.57, and 3.38 per 100 000 from 2005 to 2008, respectively. We noticed that the epidemiology of malaria in China is strongly linked to geographical situation and the characteristics of the region (Table 1). The prevalence of malaria gradually increases from the north to the south. Ecological, demographical, and climatic changes influence the distribution of malaria vectors and consequently have an impact on malaria transmission and the predominant species. In the north of China, malaria was of low endemicity and Plasmodium vivax was the only species present; temporary epidemics were occasionally caused by imported falciparum malaria. The southern part of China used to be the hyper- and meso-endemic regions where falciparum malaria was widely present. In some meso- and hypo-endemic areas, (central China), vivax malaria was predominant, though falciparum malaria also existed and focal outbreaks often occurred. The epidemic situation in China is largely affected by that in the nearby Southeast countries (Table 1 and Figure 1). Yunnan and Hainan provinces still face a severe situation of endemic malaria because of the spread of Plamodium falciparum and imported cases of malaria in 25 border counties in Yunnan province (Figure 1A). According to the data from the National Malaria Survey in 2006, the number of fatal malaria cases in Yunnan province was 32, the highest rate in China, and it accounted for 84.2% of total fatal malaria cases; subtertian malaria imported from abroad accounted for 60.4% of these cases. More than 15 000 cases of confirmed and clinically diagnosed malaria were reported in China in 2008-2009. The majority of cases were from the provinces of Anhui, Yunnan, Henan, Hainan, Jiangsu, and Hubei. However, the absolute number of malaria cases and deaths were estimated as being somewhat higher, as it is difficult for the public health system to detect patients in remotes mountainous areas (Tables 2 and 3). Based on the country’s current malaria situation, all counties are classified as high malaria incidence, with potential for malaria transmission, or historically and currently malaria free. This is intended to the development of priorities for national malaria control strategies by the authorities at national and local level (Table 4).
Characteristics of Malaria Transmission Patterns by Geographical Region. a
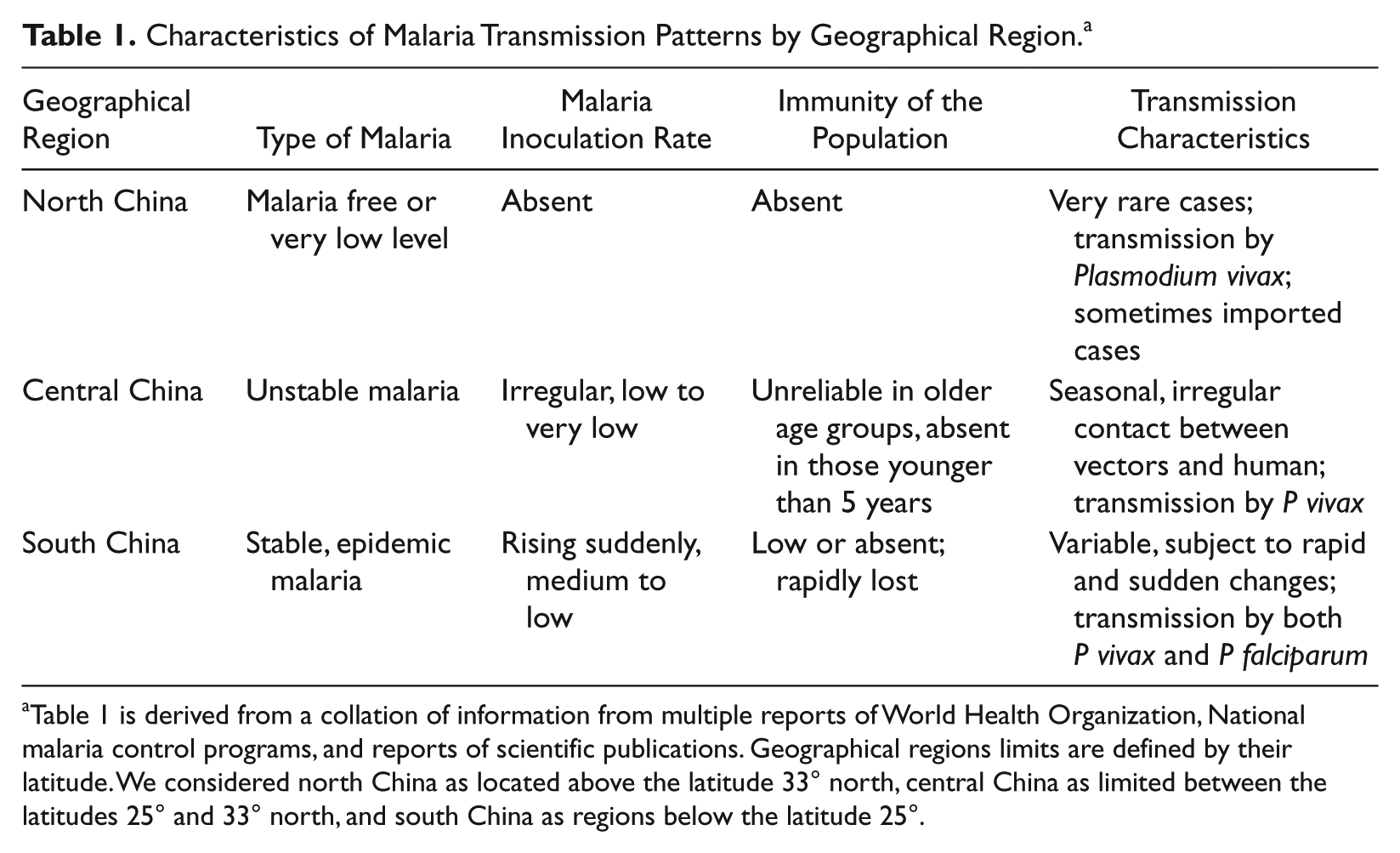
Table 1 is derived from a collation of information from multiple reports of World Health Organization, National malaria control programs, and reports of scientific publications. Geographical regions limits are defined by their latitude. We considered north China as located above the latitude 33° north, central China as limited between the latitudes 25° and 33° north, and south China as regions below the latitude 25°.
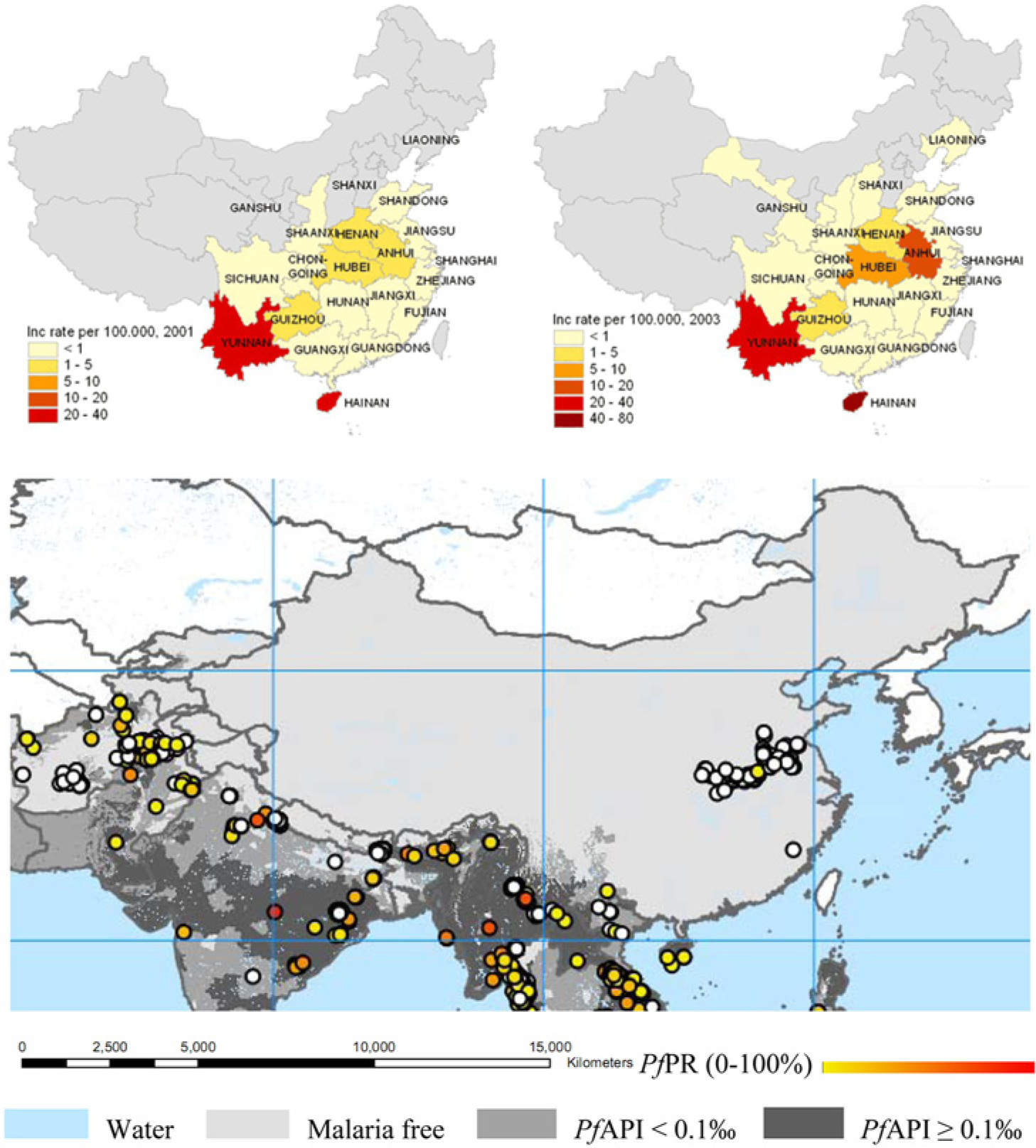
Malaria morbidity and mortality by endemicity areas in China 2001 and 2003. Spatial distribution of Plasmodium falciparum malaria endemicity in China and borders countries, 2007 endemicity map.
Malaria Morbidity and Mortality by Selected Provinces in China, 2008-2009. a
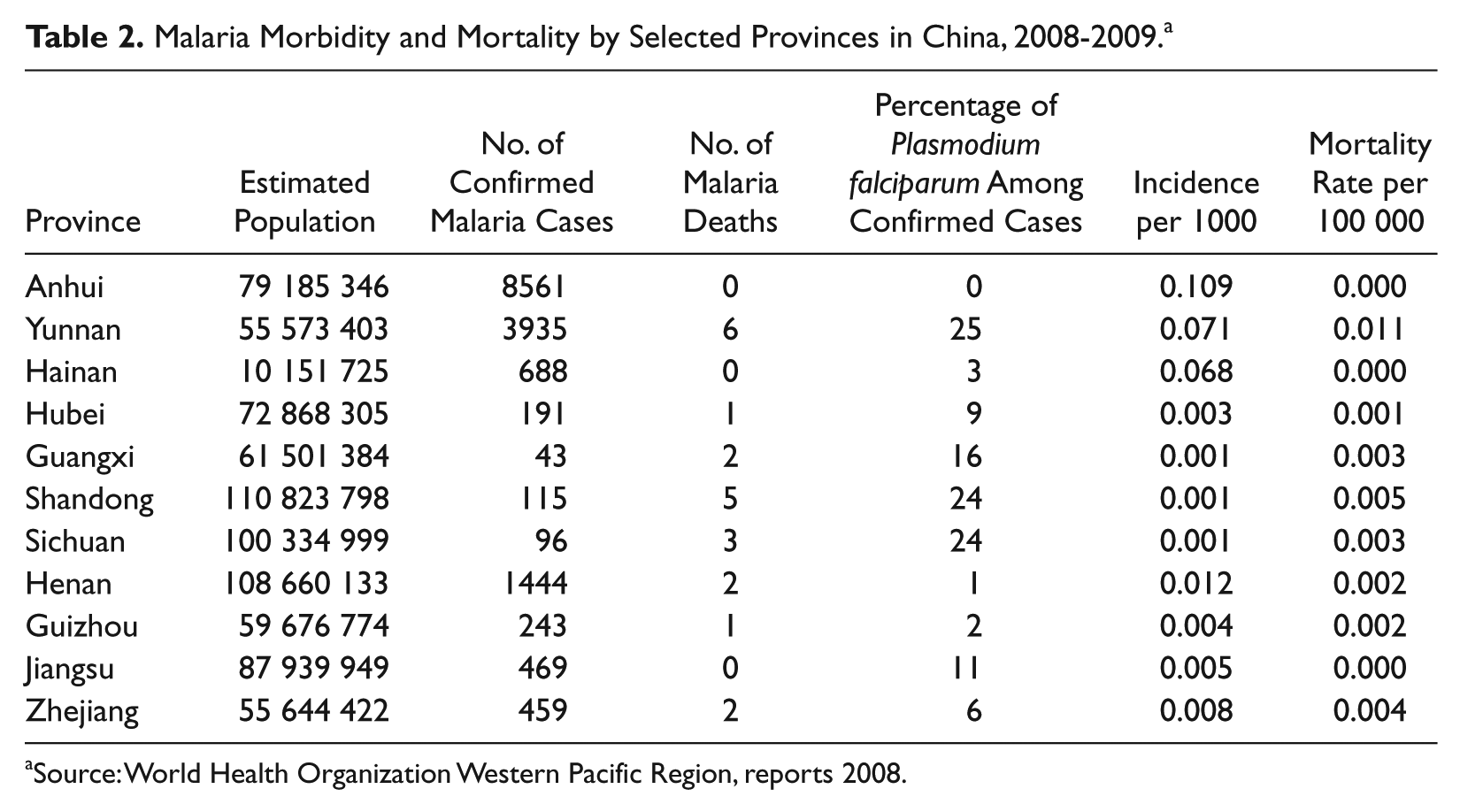
Source: World Health Organization Western Pacific Region, reports 2008.
Malaria Morbidity and Mortality in China, 2001-2009. a
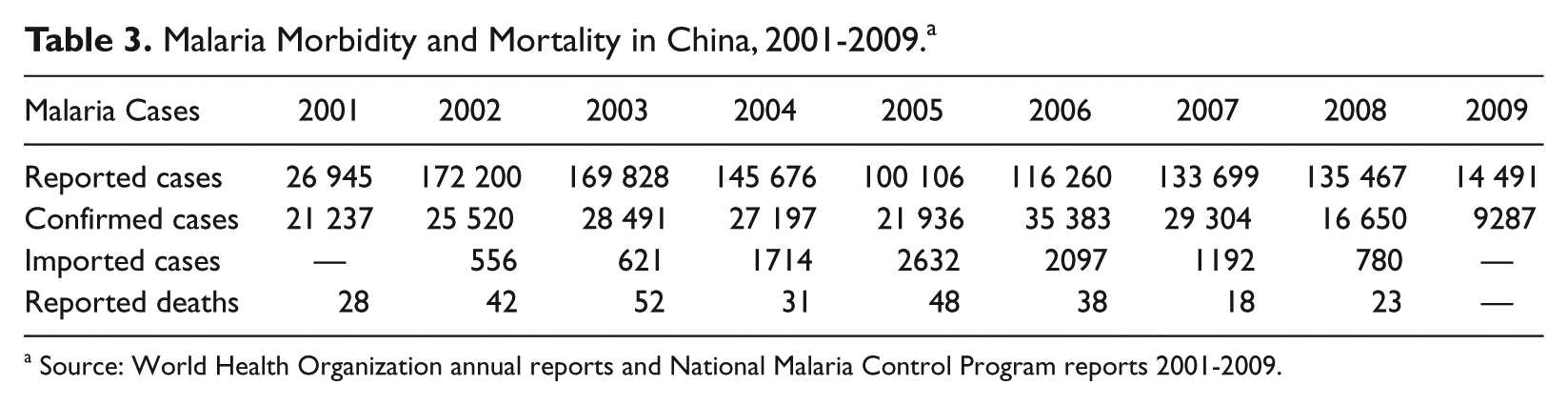
Source: World Health Organization annual reports and National Malaria Control Program reports 2001-2009.
Priority for Malaria Control Strategies and Classification, by Epidemiological Setting. a
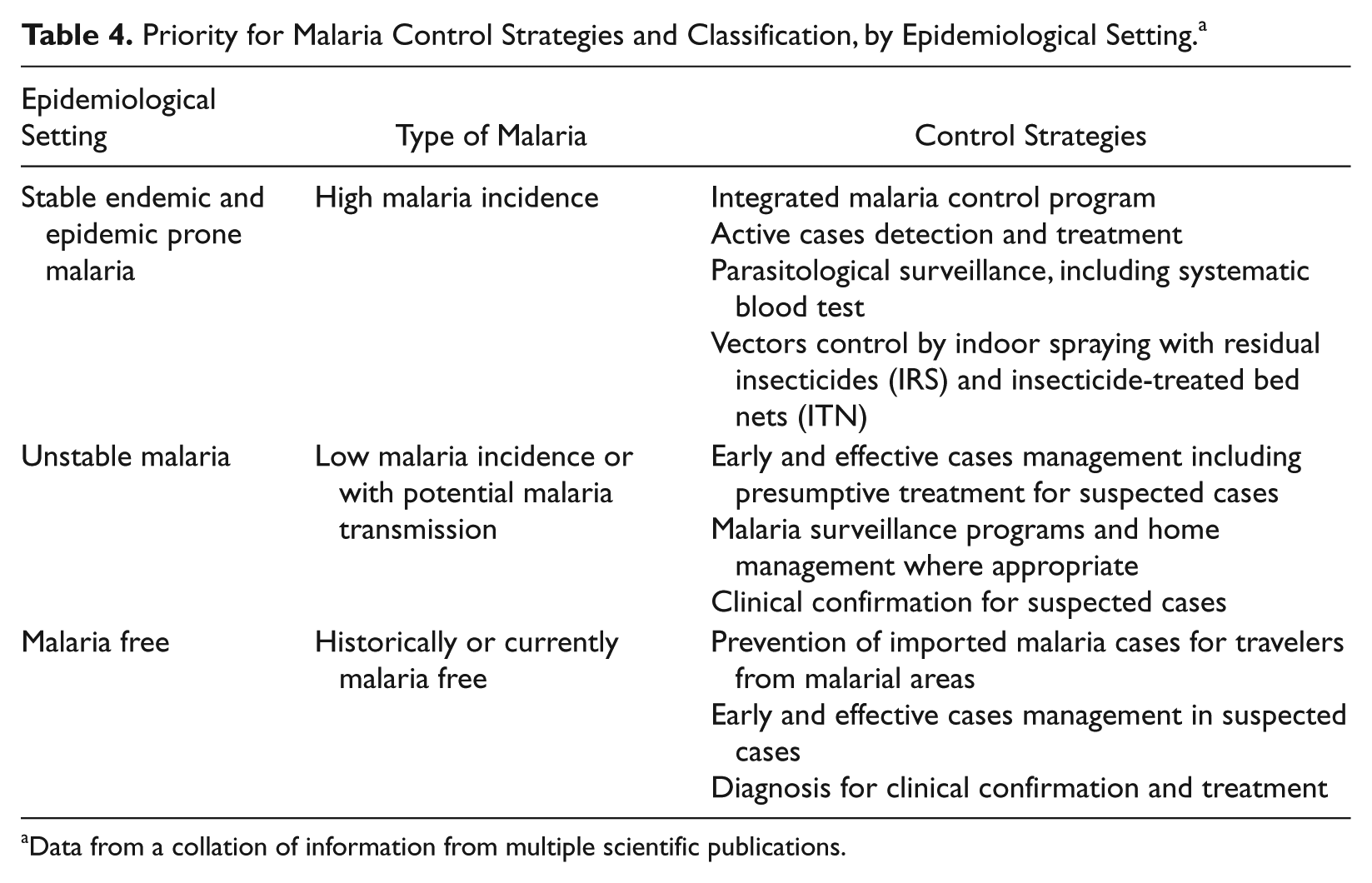
Data from a collation of information from multiple scientific publications.
Discussion
Malaria was historically an endemic disease China, 19 with prevalence varying from very high to low. The results reported here come from a strong national level monitoring and evaluation system developed through the National Malaria Control Program. We analyzed past and recent data from standardized national and regional surveys and explored factors associated with the geographical distribution of malaria around China.
In historical times, and as recently as the early to mid-20th century in southern Asia, continual malaria infection and reinfection had devastating effects on the mental, physical, social, and economic conditions of the individuals and communities affected. 20 This particular situation has galvanized the national government to establish programs for definitive eradication of the disease, under the broad direction and encouragement of the World Health Organization. 21 In the second half of the 20th century, China followed its own path. The emergence of strong national government and the absence of major warfare must have contributed significantly to the reductions of its malaria burden in the decades that followed the end of World War II. However, political turmoil within China in the late 1960s and early 1970s prevented major advances. Then, in the mid-1970s, a determined antimalaria campaign was initiated in which vector control was integrated with rigorous malaria case detection and treatment. 7 Malaria-related deaths in China may now be fewer than several hundred per year, compared with the hundreds of thousands that were sustained through the early decades of the century. The Chinese antimalaria campaign yielded another outstanding contribution. This was the development of the artemisinin derivatives of Quinhaosu, a traditional Chinese herbal medicine, to combat chloroquine-resistant P falciparum. A study has revealed that, in Vietnam, in Southeast Asia, in the early 1990s, artemisinin derivatives contributed dramatically to the reversal of a renewed rise in malaria mortality rates in the region. 22 Today these compounds are at the heart of attempts to reformulate global malarial drug policy based on drug combinations that include artemisinin derivatives as a means of combating the emergence and spread of antimalarial drug resistance.23,24
The incidence of malaria decreased dramatically during the 20th century in China. The epidemiology of the disease is extremely variable, and different situations require different malaria control strategies, adapted to risk groups, vector behaviors, local health infrastructure, and environmental conditions. Studies reveal that climatic conditions have been major factors influencing the distribution of malaria in Asia. 25 However, there is evidence of a reemergence of malaria since 2000, with more than 740 000 cases being notified in 2004. 26 A thorough examination of the situation and the data provided in the general literature reveals a real gap. There is uncertainty in the data provided, and the real burden of malaria in China is still unknown even though great efforts have been made. The actual number of reported cases is much higher than the reported cases. 27 One of the factors responsible for the reintroduction of malaria is a failure of malaria vigilance. The malaria early warning system is not well established in remote and mountainous areas, and the rapid response capability to malaria outbreak by local organizations is limited when cases occur in remote areas. 28 Another growing problem in the malaria control system in China, as in the Greater Mekong subregion, has been the proliferation of counterfeit antimalarial drugs on the market. In 2006-2007, an international multidisciplinary group consisting of World Health Organization officials, physicians, pharmacists, scientists, and Interpol officers conducted a joint investigation on counterfeit artesunate in the Mekong countries. From a sample of 391 artesunate collected between 1999 and May 2006 in Vietnam, Cambodia, Lao PDR, Myanmar, and the Thai–Myanmar border, a wide variety of fake artesunate was identified. Studies on the pharmaceutical ingredients in the counterfeits suggested that the manufacturing sites were based in China. 29
Conclusion
Substantial progress to reduce the morbidity and mortality cause by malaria in China has been made and encouraged by the National Malaria Control Program. However, elimination of malaria would be feasible if the technical and operational challenge to the permanent interruption of transmission could be overcome. A sufficiently high coverage of malaria intervention to interrupt local transmission and parasite transfer from malaria endemic to nonendemic areas is needed to assess the probability of malaria being reestablished.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.