
Abstract
Patient education concerning HIV and antiretroviral (ARV) medications is important for optimal outcomes. The authors assessed the knowledge and perceptions of HIV-infected patients in an ARV education program in Ho Chi Minh City, Vietnam. Of 185 patients, 64 (35%) receiving ARV medications, nearly 80% correctly answered questions regarding HIV. Correct responses were associated with higher education (P < .05) and longer duration of HIV diagnosis (P < .05). A lack of knowledge was observed in 40% of respondents who believed HIV and AIDS were the same and 70% of respondents who believed ARV medications cured HIV. Greater embarrassment of living with HIV was associated with female gender (P < .05) and lower education (P < .05). Patients were concerned over ARV medication use (27%) and its side effects (38%). The study population’s knowledge of HIV/AIDS and ARV medications, perceived stigmatization, and areas of knowledge deficits underscore the need for effective patient education programs addressing poorly understood issues around HIV/AIDS.
Introduction
As of 2004, Vietnam’s surveillance suggested that efforts to prevent the acceleration of the country’s HIV epidemic were inadequate. 1 Estimates reveal that HIV has infected more than 280 000 people in Vietnam and caused 24 000 AIDS deaths in 2007.2,3 Most of these reported HIV cases—17% of the national total—have originated from Ho Chi Minh City (HCMC).3,4 The start of the epidemic in Vietnam was associated with the highest HIV seroprevalent populations—injection drug users and commercial sex workers. However, heterosexual contact in Vietnam among younger individuals between 20 and 39 years and those who are not a part of the aforementioned risk groups now contributes to a large proportion of HIV infections. 2 As more individuals are infected with HIV and progress to clinical AIDS in Vietnam, antiretroviral (ARV) medication therapy has become a large focus for intervention because of their positive reduction of morbidity and mortality and dramatic improvement in quality of life of the patient.5,6
The Joint United Nations Programme on HIV/AIDS (UNAIDS) and the World Health Organization (WHO) estimate that Vietnam provides ARV medications to 28% of the HIV-infected population eligible for medical treatment. Preceding the WHO international campaign to increase universal access to ARV medications by 2010, a considerable effort to scale up ARV use in Vietnam was started in 2004 under the US President Emergency Plan for AIDS Relief (PEPFAR) program.3,7 Furthermore, Vietnam’s central government program—the National Strategy on HIV/AIDS Prevention and Control in Vietnam—doubled its domestic funding and commitment to scale up the use of ARV medications. 3 The continued financial support of PEPFAR, the Global Fund to Fight AIDS, and UNAIDS has helped Vietnam achieve a 6-fold increase in the provision of ARV therapy.3,7
Despite Vietnam’s growing provision of ARV medications, there have been concomitant fears that the rapid scale-up of ARV use under growing international and domestic initiatives8,9 would be plagued with poor patient education, adherence, and consequently the rapid emergence of HIV drug-resistant strains. 1 Unfortunately, after 5 years of rapid scale-up of ARV use, China has experienced an alarming immunologic failure rate and the development of resistant virus among patients. 10 In Vietnam, the existence of ARV medication–resistant HIV strains is currently low, but a study has shown that up to 28% of patients on ARV medications had not achieved HIV-1 virus suppression.11,12 Poor ARV adherence has been attributed to patient experiences of stigma, exaggerated fears of HIV infection, misperceptions about HIV transmission, and inadequate time and information during counseling.13-15 The increased use of ARV medications in developing countries such as Vietnam highlights the importance of providing comprehensive and effective patient education on the principles of ARV adherence and HIV transmission in preventing poor treatment outcomes.16,17
Several previous studies in Vietnam have assessed perceptions and knowledge regarding HIV/AIDS and ARV medications among members of the general population or physicians caring for these patients.18,19 Among physicians responsible for providing ARV drugs to their patients, some wrongly believed that HIV infection was curable, whereas most maintained that their patients are in need of higher education and intervention for the misuse of their medications. 20 Contrary to other resource-limited countries, 21 no such study has been conducted on HIV-infected individuals in Vietnam; therefore, the purpose of the present study was to evaluate the knowledge and perceptions regarding HIV/AIDS and ARV therapy of patients in an HIV outpatient clinic in HCMC, Vietnam. In addition, we explored the potential barriers to ARV adherence, including stigma, lack of knowledge, and misconceptions about HIV/AIDS and ARV treatment.
Methods
Study Design
We conducted a cross-sectional study collecting anonymous questionnaire data on knowledge and perceptions of HIV-infected patients toward HIV and ARV therapy between June and August 2008.
Setting
The government-run Hospital for Tropical Disease in HCMC is the main referral site for infectious diseases in southern Vietnam. The study was conducted in the hospital’s HIV Outpatient Clinic, which actively provided free medical care, enrolled patients into their education program, and administered ARV medications primarily to patients of middle to lower socioeconomic status and education level. The patient population mix is best represented in Table 1.
Patient Demographic and Clinical Characteristics of Total Sample and Based on Antiretroviral (ARV) Status (N = 185).
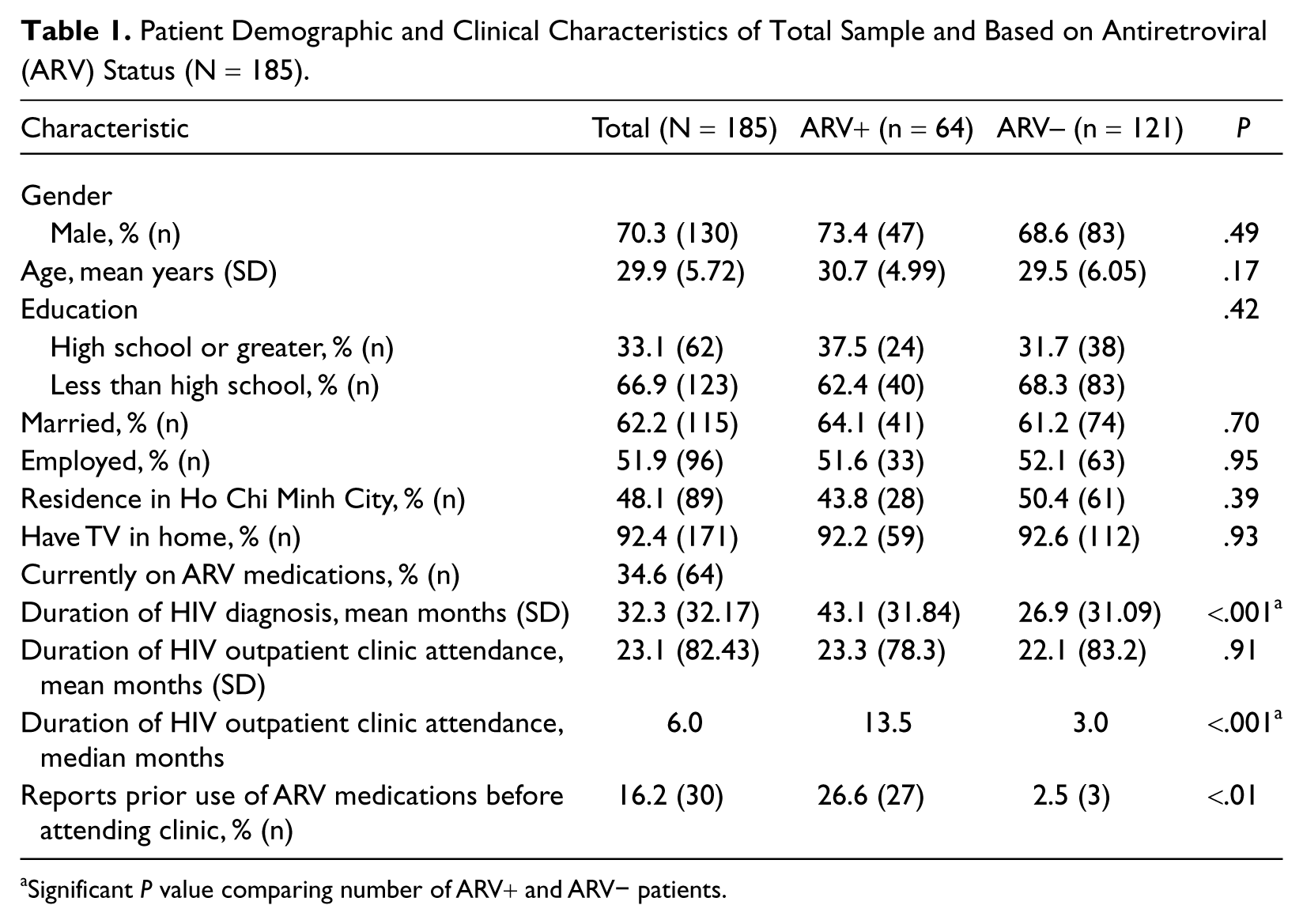
Significant P value comparing number of ARV+ and ARV− patients.
Study Participant Pool and the HIV Outpatient Clinic Antiretroviral Educational Program
Typically, HIV-positive patients queued at the clinic’s general patient holding area for routine clinical appointments with their physicians, classroom instruction, or one-on-one counseling sessions. The proportion of patients who had not started, those who had completed some, and those who entirely completed and passed the education program was not known. However, only patients who met the WHO 20063,4,7 clinical AIDS criteria were enrolled to complete a 5-part educational program, which began with 2 full days of classroom instruction in a group setting. The first class provided clearly outlined HIV/AIDS information, including clinical stages of HIV and AIDS, routes of transmission, CD4 lymphocyte count-based opportunistic infections, and mechanisms of ARV medications, goals of their use, side effects, and issues of adherence surrounding how and when to take medications. The second classroom day involved review of these lessons. Patients subsequently underwent two 1½-hour one-on-one counseling sessions. A trained ARV counselor reviewed classroom lessons, addressed patient issues regarding treatment and adherence to ARV medications, and evaluated patient understanding of why, how, and when they were to take their medications. The content of the education program adequately covered all topics surveyed by our questionnaire except for patient concerns and issues of stigma. The information was presented in a gender-neutral fashion, without addressing specific male or female issues or concerns. In the final component, patients were provided a final verbal exam. Those who were assessed by their counselor to have met the objectives of all 5 components of the educational program—2 classroom sessions, 2 counseling sessions, and the final exam—were initiated on ARV therapy the same day.
Study Questionnaire and Participant Recruitment
Subjects in the general patient holding area were blindly approached and provided information about the survey; those willing to participate were assisted by 1 of 2 interviewers in completing the questionnaire in Vietnamese. The patients were not discriminated based on the reason for their clinic visit, and therefore based on whether they had even started, completed some, or completed the entire patient education program (please see ARV status defined below). The survey instrument was adapted from a previously validated questionnaire used by Nachega et al, 21 in Soweto, South Africa. After adaptations of the questions to make them appropriate for Vietnam, our final questionaire consisted of 59 questions that required binary responses of agree or disagree. A few questions required an ordinal rank value response, and 4 questions solicited open-ended responses. Demographic information displayed in Table 1 was collected. Patients were asked questions regarding HIV transmission, the goals of HIV treatment, and the impact of ARV therapy on disease progression, the importance of medication adherence, and concerns about ARV use—all of which, except patients’ subjective concerns and issues of stigma, were instructional topics covered by the clinic education program. The Human Investigation Committee of Yale University School of Medicine and the Director of Research at the Hospital for Tropical Disease, HCMC, Vietnam, approved the conduct of this study.
Antiretroviral Status Defined
Patients were identified as either ARV+ or ARV−. Those patients who were ARV+ met the criteria of successful completion of all 5 parts of the HIV Outpatient Clinic ARV Educational Program and active use of ARV medication treatment prescribed by clinic physicians. ARV− patients were defined as individuals who had completed 0 or some parts of the aforementioned education program and had not yet started ARV treatment.
HIV and Antiretroviral Therapy Knowledge Composite Scoring System
Comparisons of correct answers to 22 important HIV knowledge questions and 9 ARV therapy knowledge questions were made. Composite scores for knowledge of HIV were calculated by adding the number of correct answers to the complete set of questions regarding HIV transmission, prevention, cause, and disease progression to AIDS. Each correct answer contributed 1 point, whereas incorrect answers contributed 0 points to the maximum total score of 22. Patient’s perceptions of benefits of ARV medications and consequences of nonadherence were also evaluated through a total composite score of 9 related questions.
Evaluation of Patient Stigma and Concerns
Patients were asked about any embarrassment from living with HIV. A Likert-type scale that consisted of 4 ordered response levels—not, little, somewhat, very—evaluated patient concerns over ARV use, efficacy, and side effects and their willingness to disclose personal ARV use to family, friends, and sexual partners. Furthermore, patients were asked to report on their own perceived state of health compared with their peers.
Statistical Methods
Means of continuous variables and frequencies of discrete variables were computed in descriptive data. Crude analysis involved t test to compare the means of age, duration of HIV diagnosis, and knowledge composite scores, whereas χ2 test or Fisher’s exact test were used to compare discrete demographic variables (categorized in Table 1) among the stratified ARV+ and ARV– patients.
Three main outcomes—overall HIV knowledge, knowledge and perception of ARV medications, and perceived stigmatization—were evaluated. Based on the aforementioned knowledge questions and composite scores, crude and adjusted odds ratios (ORs) were calculated to study the association of HIV and ARV knowledge outcomes with ARV status using logistic regression. Analysis of variance was used to compare mean difference of the scores. The outcome of perceived stigmatization, including self-health ratings as a whole population and stratified by ARV status, was evaluated using logistic regressions. Multivariate models adjusted for demographic covariates (Table 1).
A P value of <.05 was considered statistically significant. All analyses were performed with the SAS package, version 9.02.
Results
Demographic and Clinical Characteristics
A total of 185 HIV-infected patients older than 18 years completed the survey (Table 1). Of these 185 patients, all were of Vietnamese nationality, 70% were male, and 93% were between 20 and 39 years old (mean = 29 years). Only 33% of the surveyed patients completed some high school education or more, 62% were married, 52% were employed, and 48% of patients lived in HCMC. A total of 64 patients (35%) were currently receiving ARV medications. The mean duration since HIV diagnosis was 32 months. There were no statistically significant differences in characteristics between the ARV+ or ARV− status of patients at the time they completed the survey except for the mean duration of HIV diagnosis and median duration of attendance at the clinic. Those with an ARV+ status, patients who completed the education program and actively received ARV medications, had a diagnosis of HIV for approximately 16 months longer than those who had an ARV− status (43.0 vs 26.9 months; P < .001). Patients’ reported duration of attendance at the clinic was not normally distributed; the median duration in clinics is 6 months, of which 95% of patients were at the clinic for less than 36 months. ARV+ patients had a median duration at the clinic approximately 10.5 months longer than those with an ARV− status (13.5 vs 3.0 months; P < .001). In addition, 27% of those with ARV+ status reported having used ARV medications prior to enrollment in the clinic’s ARV education program as compared with 2.5% of those with ARV− status (P < .01).
HIV/AIDS Knowledge
Overall, more than 80% of the respondents (Table 2) were able to correctly answer most questions regarding HIV transmission, prevention, and causes as well as general HIV/AIDS knowledge. There were no statistically significant differences based on ARV status. Notably, there were some questions that a smaller proportion of respondents answered correctly. Only 75% of the total sample correctly answered that one could get HIV from a blood transfusion. Only 76% of those surveyed answered that HIV is caused by a virus. Questions meant to elicit the concept that HIV and AIDS are not the same condition revealed that only 61% of survey participants correctly agreed that someone can have a positive blood test for HIV and not have AIDS, whereas only 49% appropriately disagreed that an HIV-infected patient without symptoms can have AIDS.
Accuracy of HIV/AIDS Knowledge of Total Sample (N = 185).
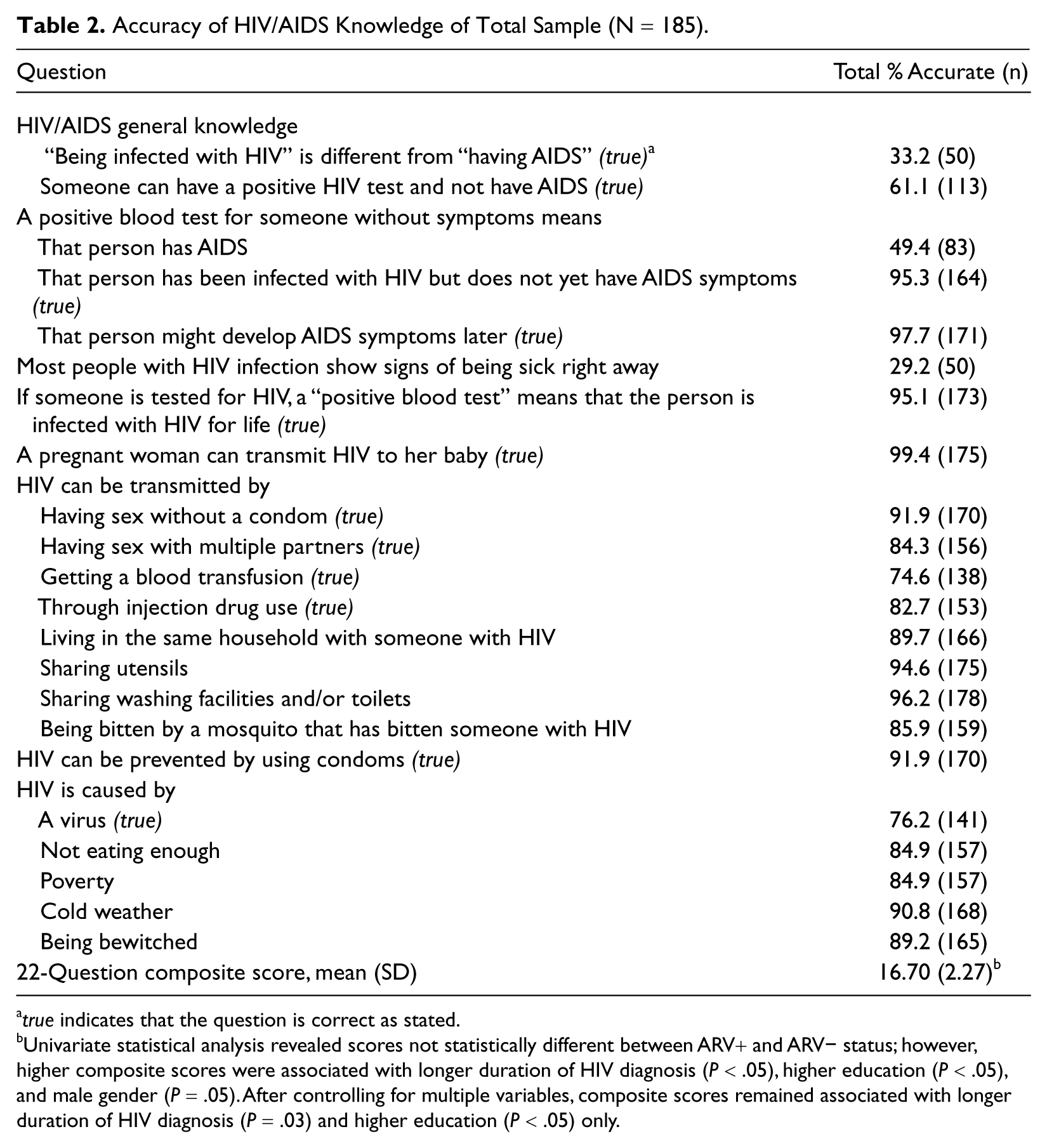
true indicates that the question is correct as stated.
Univariate statistical analysis revealed scores not statistically different between ARV+ and ARV− status; however, higher composite scores were associated with longer duration of HIV diagnosis (P < .05), higher education (P < .05), and male gender (P = .05). After controlling for multiple variables, composite scores remained associated with longer duration of HIV diagnosis (P = .03) and higher education (P < .05) only.
An unweighted composite score was created from all questions listed in Table 2 and considered knowledge of HIV transmission, its differentiation from AIDS, and its causes. The mean knowledge score was 16.7 out of 22 (SD = 2.27). There was a significant association of this score with higher education level (P < .05), longer duration of HIV diagnosis (P < .05), and male gender (P = .05), but not with patient age or ARV status. After adjusting for covariates (Table 1), the knowledge composite score remained associated with higher education level (P < .05) and longer duration of HIV diagnosis (P = .03).
Antiretroviral Medication Knowledge
A majority of patients correctly responded that ARV can prevent HIV progression (89%), prolong life (98%), and cause side effects (90%; Table 3). Regarding medication adherence, 86% of patients responded that not adhering to medication regimens leads to disease progression. A smaller percentage of patients identified the potential use of ARV for HIV prophylaxis in the case of mother-to-child transmission (60%) and postexposure (72%). Only 30% of those who were surveyed correctly identified that HIV could not be cured with the use of ARV medications; in other words, an alarming 70% of respondents incorrectly believed that HIV can be cured with the use of ARV medications.
Accuracy of Perceptions of Antiretroviral (ARV) Benefits and Importance of ARV Adherence of Total Sample (N = 185).
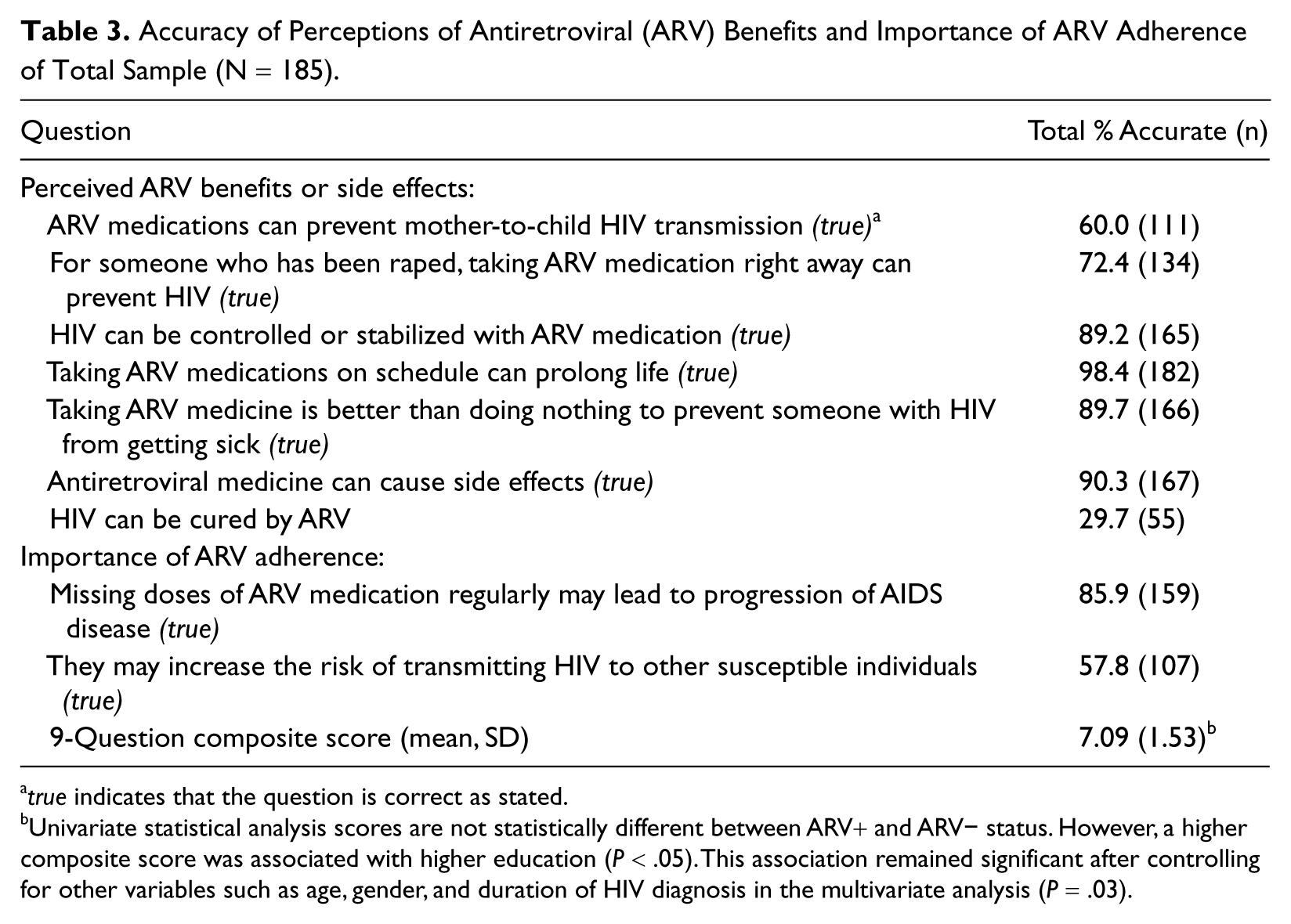
true indicates that the question is correct as stated.
Univariate statistical analysis scores are not statistically different between ARV+ and ARV− status. However, a higher composite score was associated with higher education (P < .05). This association remained significant after controlling for other variables such as age, gender, and duration of HIV diagnosis in the multivariate analysis (P = .03).
An unweighted composite score of questions in Table 3 was created to evaluate patient knowledge of ARV effects. The mean score was 7.09 out of 9 (SD = 1.53). Controlling for covariates in a multivariate model, we found a higher unweighted ARV knowledge composite score to be associated with higher education (P = .03), but not ARV status, age, gender, or duration of HIV diagnosis.
Perceived Embarrassment and Concern Over Taking Antiretroviral Medications
Several questions examined patient perception of embarrassment associated with HIV diagnosis and ARV use as well as general concern over ARV use. Nearly 43% of patients surveyed reported feeling embarrassed to be living with HIV, especially when their friends and family knew about their diagnosis. Multivariate analysis revealed that a higher level of embarrassment was associated with female gender (adjusted OR = 1.80; 95% confidence interval [CI] = 1.10-3.67) and lower education level (adjusted OR = 1.79; 95% CI = 1.20-3.47; Table 4). Although a majority of the patients surveyed expressed a Likert-type scale response level of little or no concern, a significant percentage of patients were concerned over taking ARV drugs (27%) and their side effects (38%). Although a majority reported little or no concern about others discovering their ARV use, significant percentages of patients did have concerns about friends (32%), their sexual partners (27%), or family (23%) finding out. Regarding self-health rating, those not taking ARV medications expressed a lower health rating (P = .03); those who were on ARV drugs were more likely to report feeling and being healthy (adjusted OR = 2.13, 95% CI = 1.09-4.14; Table 5).
Living With the HIV Infection Is Embarrassing.
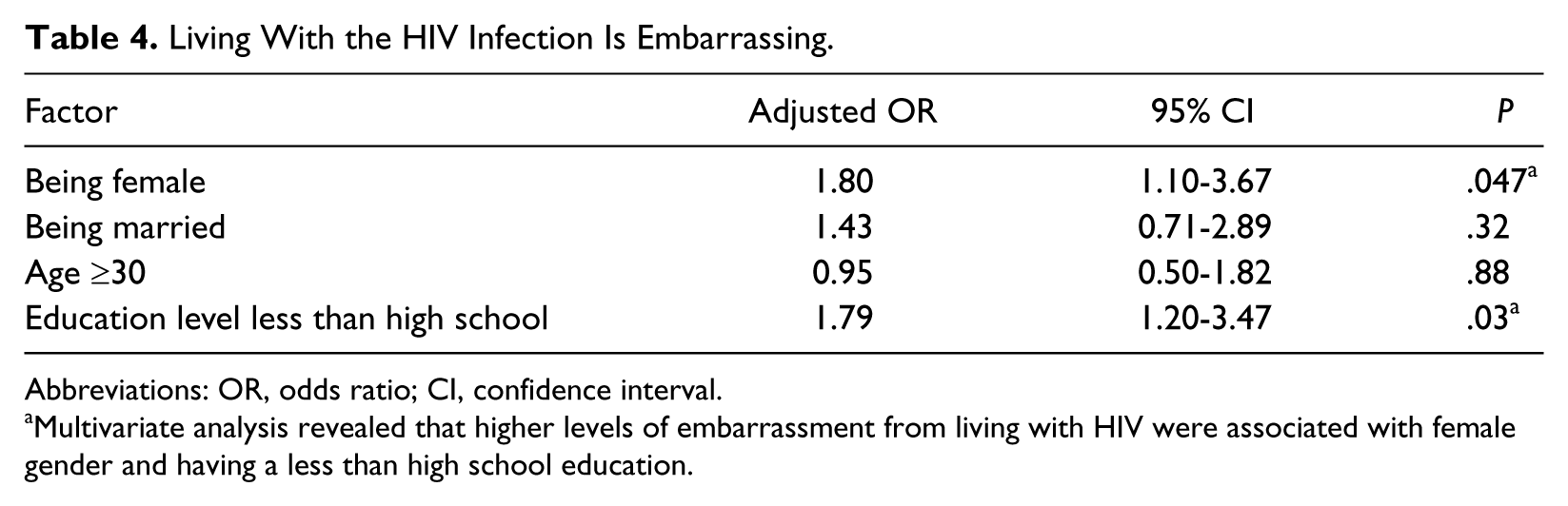
Abbreviations: OR, odds ratio; CI, confidence interval.
Multivariate analysis revealed that higher levels of embarrassment from living with HIV were associated with female gender and having a less than high school education.
Patient Perceived Self-Health Rating: Feeling Less Healthy and Worse Than Their Peers.
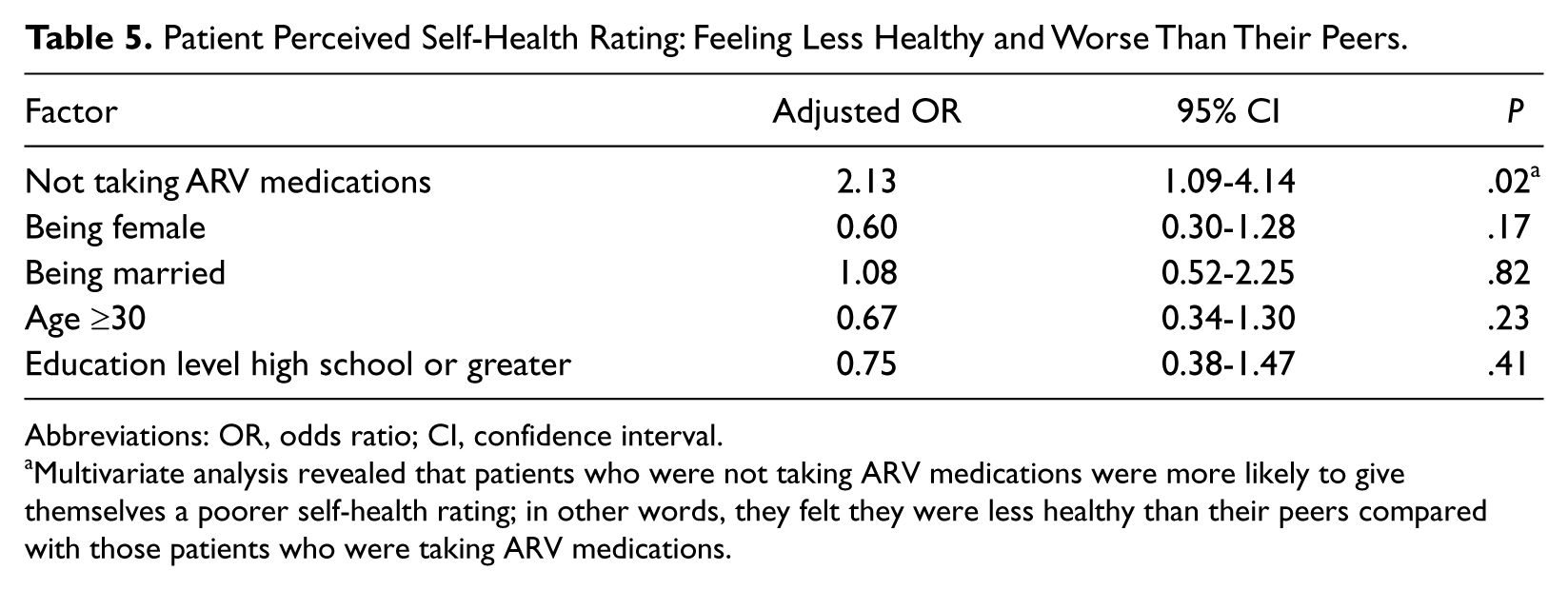
Abbreviations: OR, odds ratio; CI, confidence interval.
Multivariate analysis revealed that patients who were not taking ARV medications were more likely to give themselves a poorer self-health rating; in other words, they felt they were less healthy than their peers compared with those patients who were taking ARV medications.
Discussion
To the best of our knowledge, this is the first report of its kind on the knowledge and perceptions of HIV and ARV medications among HIV-infected patients in Vietnam. Our survey results demonstrate that, in general, our study patients’ knowledge was fairly high with a few targetable misconceptions. No significant differences were found in their level of knowledge based on their ARV status in the hospital-based education program; however, increased general HIV/AIDS knowledge was associated with higher educational level and longer duration of HIV diagnosis, whereas general ARV knowledge was associated with higher education level only. These are expected findings as higher education levels reasonably predispose patients to both a broader knowledge base and a greater capacity to gain information. Also, a longer known HIV diagnosis period understandably affords patients more exposure, awareness, and time to adjust and understand issues surrounding their disease, again promoting their knowledge level.
Despite the overall knowledge levels being relatively high, there should be some concern over specific knowledge gaps—study questions that received an alarmingly less number of correct responses. Only a minority could identify the viral cause of their illness; fewer could clinically distinguish HIV from AIDS. Questions concerning prophylactic ARV use and its complex mechanistic properties resulted in an increase in incorrect responses. More frighteningly, a lopsided percentage of surveyed patients believed incorrectly that ARV treatment cures HIV despite the education program instructing on the mechanisms and goals for ARV treatments; it remains unclear whether this represents exaggerated optimism in the medications, or less likely, whether this is due to confusion in the language used surrounding “cure.” Patients in the education program were explicitly instructed that HIV can never be rid from the body but that ARV therapy can reduce the viral load, prevent the development of AIDS, and extend life expectancy to normal. Furthermore, this survey was done in translation, but multiple, Vietnamese-fluent individuals reviewed it to ensure that the interpretations were as terminologically correct as possible. Consequently, these findings highlight vital areas of patient education, which need reinforcement as those matters have important long-term survival implications.
The collected responses further reveal a noteworthy amount of patient concern and apprehension over living with HIV/AIDS and smaller but significant percentages regarding ARV use. Addressing patient concerns should remain an important clinical priority. However, for the majority of patients responding without concerns over ARV but willingness to acknowledge their use of ARV medications to friends and family, this alludes to a potentially important area for HIV care intervention involving support persons, which has been shown to have a positive impact on patient ARV adherence. 15
We found our sample to be representative of the patient profile described in other studies conducted at an HIV outpatient clinic in a neighboring district in HCMC, 22 specifically observing an overrepresentation of males (70% of participants), which is similar to national sources identifying that males make up a large majority of patients living with HIV.3,4 The knowledge level of our study patients is significantly higher than those of the general population; a national study in Vietnam (not confined to HIV-positive individuals) found that only 46% of young individuals correctly identified ways of preventing transmission of HIV and rejected major misconceptions about HIV transmission (compared with >80% of our patients). 3 In comparison with respondents of a similar study in Soweto, South Africa, the response rates of our patients fared worse. 21 Only 16% of Soweto patients did not know that HIV and AIDS are distinct clinical entities compared with 50% of our patients. Only 6% of Soweto respondents versus 40% of our patients could not identify the use of ARV medications for vertical transmission prophylaxis. Overall, 70% of our patients alarmingly held the incorrect belief that HIV can be cured by ARV medications compared with only 49% of Soweto patients. 21 Alarmed by such data, we examined the hypothesis that if patients are confused by the distinction of HIV and AIDS, then they may mistakenly think that the prevention of AIDS symptoms by ARV conveys that HIV is a curable disease; we ran a correlation analysis and statistical test but found no associations between believing that HIV is curable and not being able to distinguish HIV and AIDS as separate clinical entities (φ coefficient correlation = .13. χ2 test P = .09). We can only speculate that such misconception, however, is based on specific information taught about HIV and its relationship with AIDS. ARV knowledge was not found to be associated with any particular variable in their multistep logistic regression model 21 ; we found that higher education was associated with greater HIV and ARV knowledge. Again, these findings highlight areas of improvements for the Vietnamese education program as well as fundamental knowledge that directly affect patients’ quality of life and behaviors regarding HIV transmission and medication adherence.
The trend toward a gender gap in knowledge that our study revealed has been demonstrated in other studies and nationally reported values.3,18,23 In Vietnam, gender roles and expectations that hold women to high sexual standards likely contribute to the observed differences in knowledge and attitudes toward men and women’s sexual activity. These cultural and societal expectations and norms may expose men to more information than women 23 ; this may translate to gender-related differences in perceptions of stigma as well. Despite these differences, alternatives to gender-specific interventions may need to be developed—which currently were not made available—in order to increase women’s knowledge and reduce stigma. 24
Our findings of embarrassment around HIV infection and ARV use are similar to what have been discussed in other studies.13- 15 ,24,25 Embarrassment of living with HIV was found to be higher among female respondents. Current literature reveals mixed evidence. One study identified that overall men internalized HIV/AIDS stigma more than women possibly because of greater discrimination experiences; however, women were more likely to become depressed despite having greater social support. 26 Our finding of concerns over disclosing ARV use to support a person will be important to address as studies have shown that the lack of self-perceived social support from friends, family, and significant others has been associated with poorer ARV use compliance. 27
Patients, not on ARV medications, who reported feeling less healthy than their peers is consistent with HIV/AIDS research findings. ARV treatment has the potential to improve patient perception of quality of life and health, whereas those who are not receiving them show less favorable changes in perceived quality of life. 28 Perhaps medication use and having to be proactive about one’s health makes a patient feel healthier, resembling a placebo effect; alternatively, patients may actually be physically better because of medication efficacy. Many studies have reiterated that successful adherence to ARV medications involves not only developing the support of friends and loved ones but also adequate provider–patient collaboration and education to address patient experiences of stigma, exaggerated fears of HIV infection, misperceptions about HIV transmission, the efficacy of antiretroviral regimens, and medication side effects.13-15 Although the rapid scale-up of ARV use may reduce patients’ sense of self-stigma, there is evidently an increase in societal stigma regarding ARV provision, specifically increased fears of promiscuity and spread of HIV by healthy HIV-positive patients.29,30
All individuals who attended the course inevitably went on to receive ARV treatment; patients who failed to attain classroom and counselor objectives were quickly remediated with one-on-one counseling to optimize patient understanding, and then offered a chance to retest. Although each patient eventually passed the exam and went on to receive treatment, the testing process became less discriminatory with subsequent remediation and retesting. This bolsters concerns over poor patient education standards and made our evaluation of patient knowledge as an outcome of education all the more important. The continued gaps in patient knowledge despite the systematic educational intervention are of further concern that the level of knowledge of patients before they receive clinic interventions is likely lower. We believe that the current patient education at the very least provides vital basic HIV/AIDS knowledge and instructions on the use of and importance of adhering to ARV treatment—efforts that undeniably contribute to the success of ARV intervention of the HIV epidemic. As such, the current education model appears to be working and our findings simply highlight that the program can be augmented further to be more effective.
This study has several limitations. First, our sample of 185 HIV-infected patients may not be completely generalizable to the HIV-infected population of HCMC or nationally 3 because heterogeneity may exist between clinics and between cities in Vietnam. Despite this finding, we did ascertain our sample to be consistent with other patient cohorts described in another study conducted at an HIV outpatient clinic in a neighboring district in HCMC. 22 In addition, a number of our findings were similar to those reported in the aforementioned studies and we believe are valuable in terms of their implications for educational programs focused on HIV and ARV treatment in many geographic locations. Second, the patients surveyed were currently at various stages of patient education and clinical treatment; their status with regard to whether they had not started education or completed some education could not be accurately assigned. We used ARV use as a proxy measure to divide the patients into 2 groups: those who completed the education program versus those who had some or no education. Furthermore, presumably, some patients may have been in a gray zone where they completed the education program but had not yet started ARV treatment. These may have limited the study from being able to draw any direct conclusions about the efficacy of the education program in place. However, as the knowledge among our study participants was significantly higher than in the general population, this provides indirect support of the value of the education program. Last, our small sample size may not have had the power to detect significant associations.
In summary, the present study demonstrates that the HIV outpatient participants we surveyed have, in general, higher knowledge than reported national levels about HIV/AIDS, disease progression, transmission, and the use of ARV medications. Despite our belief in the value and effectiveness of the patient education program conducted at this HCMC hospital, there are patient knowledge and perception inaccuracies, which need to be addressed as they have the potential of seriously affecting patient clinical outcomes. In addition, patient embarrassment about their HIV diagnosis and concerns over ARV use are present and may influence patient behavior around disclosing their diagnosis and comfort around taking ARV medications. Therefore, our findings highlight not only areas of strength but also areas that need further evaluation, focus, and intervention in ongoing and future educational efforts.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
Support provided by the Wilbur Downs International Student Travel Fellowship and Yale Student Summer Research Fund.